

Abstract
Aims: This study is to investigate the expression levels of vascular endothelial growth factor (VEGF) and cancer antigen 125 (CA125) in serum of adenomyosis patients before and after interventional therapy. The role of serum levels of VEGF and CA125 for the prognosis of adenomyosis is further studied. Methods: A total of 80 adenomyosis patients treated with interventional therapy and 40 healthy individuals were enrolled in this study. Enzyme-linked immunosorbent assay was performed to detect the expression levels of VEGF and CA125. Receiver operating characteristic analysis was used to determine the treatment effect on adenomyosis. Kaplan-Meier analysis was used to analysis the progression-free survival curve for prognosis of adenomyosis. Results: The expression levels of VEGF and CA125 in serum of patients with adenomyosis was increased when compared with those of healthy individuals before interventional therapy (P < 0.05). Levels of hemoglobin in adenomyosis patients after surgery was increased compared with those before surgery (P < 0.05). The blood volume of menstruation, pain intensity, and volume of uterus in adenomyosis patients after surgery was significantly decreased when compared with those before surgery (P < 0.01). The survival rate of adenomyosis patients with high VEGF and CA125 levels was decreased. Serum levels of VEGF and CA125 had a high sensitivity and specificity for the prognosis of adenomyosis. Conclusions: The serum expression levels of VEGF and CA125 are related to the development of adenomyosis. VEGF and CA125 serum levels can be used for predicting the prognosis of adenomyosis.
Keywords: Adenomyosis, interventional therapy, vascular endothelial growth factor and cancer antigen 125
Introduction
Adenomyosis, as one of common gynecological diseases, is mainly caused by the invasion of the endometrial glands and mesenchyme to the myometrium. Adenomyosis results in dysmenorrhea, increased menstrual flow, menostaxis and secondary anemia, which seriously affects the quality of life of female patients. Abnormal cell proliferation, invasion, and infiltration occur in the myometrium of patients with adenomyosis. In recent years, the incidence of adenomyosis varies widely, fluctuating between 10%-60% in different countries and hospitals. The overall trend of incidence has been increasing [1]. Interventional technique has been used in the treatment of adenomyosis in recent years [2]. The mechanism of interventional therapy for adenomyosis is inhibiting the blood supply of the lesions, eventually leading to the necrosis of ectopic endometrial. Interventional therapy can reduce the volume of uterine, menstrual flow, and alleviate dysmenorrheal. Previous study showed that, for the adenomyosis patients with interventional therapy, the lesion became smaller or disappeared. The symptoms of adenomyosis were gradually reduced [3].
Vascular endothelial growth factor (VEGF) is one of important factors inducing angiogenesis. Expression levels of VEGF in tissues can reflect the activity of angiogenesis [4,5]. Previous study showed that VEGF also induced angiogenesis in tumor tissues [6]. Therefore, the promotion function of VEGF to angiogenesis provides nutrients to the grown of ectopic endometrial glandular epithelial cells [7]. VEGF promotes the ability of proliferation and infiltration into the myometrium, thereby increasing the depth and scope of the lesion.
Cancer antigen 125 (CA125) is used as a traditional molecular marker for the detection of ovarian cancer. Recent study showed that the levels of CA125 were closely related to the development of the endometrium [8,9]. The expression levels of CA125 are also related to the different type of adenomyosis patients [10,11]. Detection of CA125 expression levels in serum plays an important role in the diagnosis of adenomyosis.
In this study, the expression levels of VEGF and CA125 have been determined in serum of patients with adenomyosis. Receiver operating characteristic (ROC) analysis has been used to analyze the treatment effect on adenomyosis according to the levels of VEGF and CA125 in serum. The role of VEGF and CA125 has been further studied by the progression-free survival analysis for prognosis of adenomyosis.
Materials and methods
Patients
A total of 80 adenomyosis patients treated with interventional therapy were enrolled in this study. The patients with adenomyosis included 30 unmarried cases and 22 married cases. The age of these 80 patients ranged from 27 to 50 years, with an average age of 39.6 years. For control, 40 healthy individuals were enrolled in this study. Prior written and informed consent were obtained from every patient and the study was approved by the ethics review board of Xi’an Jiaotong University.
Interventional therapy
The surgery of interventional therapy was performed 3-5 days after menstruation. The patients were supine on the operating table. After routine disinfection and local anesthesia, artery puncture catheter was inserted through the internal iliac artery to reach the uterine artery. Bleomycin was injected into the catheter. The lesions of small blood vessels were embolized by alginate microspheres. The main uterine artery was embolized by gelatin sponge. Postoperative patients were routinely given antibiotics to prevent infection, abdominal pain, fever and other symptoms for three to five days.
Evaluation and follow-up
Patients were followed-up at one month, six months, and twelve months after interventional therapy. The volume of uterus, lesions was evaluated by ultrasound, CT or MRI examination. Hemogram and blood flow were also evaluated. During the follow-up time, 18 patients were censored. Patients died of other causes, lost to follow-up at the time of last contact or before study cut-off were censored.
Enzyme-linked immunosorbent assay (ELISA)
Peripheral blood was collected from adenomyosis patient and healthy individuals before and after surgery. The peripheral blood was centrifuged at 15000 rpm for 15 min. The supernatant was transferred to a new tube and stored in -40°C.
ELISA assay was carried out according to the manual provided by the ELISA kit (Roche, Basel, Switzerland). Briefly, the serum was added to the microplate and incubated at 4°C overnight. After washing for 5 times, detection antibody was added to the wells. After incubation at room temperature for 1 h, the microplate was washed again. Then HRP conjugated antibody was added and incubated at room temperature for 30 min. After washing for 5 times, substrate solution was added and incubated at room temperature for 15 min. Finally, stop solution was added to stop color development and the plate was read at 450 nm with American ACS-1800SE automated chemiluminescence analyzer (Bayer Corporation, Tarrytown, NY, USA). The standard curve was generated by 2-fold serial dilutions of the standard samples. The levels of VEGF and CA125 were calculated according to the standard curve.
Statistical analysis
All results were expressed as mean ± standard deviation. All statistical analyses were performed with SPSS version 17.0 for Windows (SPSS Inc., Chicago, IL, USA). Paired t-test was used to analyze comparisons between groups and analysis of paired data. ROC analysis was used to determine the treatment effect on adenomyosis according to the levels of VEGF and CA125 in serum. Kaplan-Meier analysis was used to analysis the progression-free survival curve for prognosis of adenomyosis. P value less than 0.05 was considered to be significantly different.
Results
General data of patients with adenomyosis
A total of 80 adenomyosis patients treated with interventional therapy were enrolled in this study. General data of patients with adenomyosis was showed in Table 1. Among them, there were 56 cases of simple adenomyosis, 24 cases of adenomyosis complicated with uterine fibroids, 38 cases of adenomyosis with focal adenomyosis, and 42 cases of adenomyosis with diffuse lesions. The age of these 80 patients ranged from 27 to 50 years, with an average age of 39.6 years. The patients with adenomyosis included 30 unmarried patients and 22 married patients. The levels of hemoglobin ranged from 55.3 to 101. 2 g/l, with an average level of 80.2 g/l.
Table 1.
General data of patients with adenomyosis
| Clinical characteristics | Case numbers | |
|---|---|---|
| Ages (years) | ≥ 27, < 50, 39.6 ± 7.69 | 80 |
| Adenomyosis complicated with fibroid | No | 56 |
| Yes | 24 | |
| Degrees of anemia | Mild | 51 |
| Moderate | 19 | |
| Severe | 10 | |
| Numbers of lesions | Focal | 38 |
| Diffuse | 42 | |
Note: Mean ± standard deviation.
Expression levels of VEGF and CA125 in serum before and after surgery
To investigate the expression levels of VEGF and CA125 in serum before and after surgery, enzyme-linked immunosorbent assay was performed. As shown in Table 2, the expression levels of VEGF and CA125 in serum of patients with adenomyosis was increased when compared with those of healthy individuals before interventional therapy (P < 0.05). The expression levels of VEGF and CA125 in serum of patients with adenomyosis at one month after interventional therapy was decreased when compared with those before interventional therapy (P < 0.05). The expression levels of VEGF and CA125 in serum were gradually decreased after interventional therapy. These results indicate that the serum expression levels of VEGF and CA125 is related to the development of adenomyosis.
Table 2.
Expression levels of VEGF and CA125 in serum before and after surgery
| Groups | VEGF (pg/ml) | P value | CA125 (ku/l) | P value |
|---|---|---|---|---|
| Control | 62.1 ± 26.4 | 77.9 ± 34.8 | ||
| Before surgery | 170.3 ± 39.4 | 0.001 | 115.4 ± 54.9 | 0.05 |
| One month after surgery | 152.2 ± 25.4 | 0.001 | 76.2 ± 23.3 | 0.05 |
| Six months after surgery | 128.3 ± 38.8 | 0.001 | 43.5 ± 32.7 | 0.05 |
| Twelve months after surgery | 101.6 ± 43.1 | 0.001 | 26.7 ± 12.1 | 0.05 |
Note: Mean ± standard deviation.
Treatment effect of interventional therapy for adenomyosis
To evaluate the treatment effect of interventional therapy for adenomyosis patients, the blood volume of menstruation, levels of hemoglobin, the volume of uterus, and the pain intensity was measured at 12 months after surgery. As shown in Table 3, levels of hemoglobin in adenomyosis patients after surgery was increased when compared with those before surgery (P < 0.01). The blood volume of menstruation in adenomyosis patients after surgery was significantly decreased when compared with those before surgery (P < 0.01). After surgery, the pain intensity and volume of uterus were significantly decreased (P < 0.01). These results suggest that the interventional therapy have a good effect on the adenomyosis treatment.
Table 3.
Treatment effect of interventional therapy for adenomyosis
| Volume of menstruation (%) | Hemoglobin (g/l) | Pain intensity (scores) | Volume of uterus (cm3) | |
|---|---|---|---|---|
| Before surgery | 100.0 | 72.3 ± 10.5 | 95.3 ± 3.6 | 256.8 ± 115.3 |
| After surgery | 46.7 ± 19.5 | 130.4 ± 12.5 | 12.6 ± 5.7 | 13 6.7 ± 63.6 |
| P value | < 0.01 | < 0.01 | < 0.01 | < 0.01 |
Note: Mean ± standard deviation.
ROC analysis for analyzing the treatment effect on adenomyosis
To analysis the treatment effect of interventional therapy on adenomyosis, ROC analysis was performed according to the levels of VEGF and CA125 in serum.
As shown in Figure 1, the area under ROC curve was 88.8% and 84.6% for the serum levels of VEGF and CA125, respectively. The optimal cut-off value of the serum levels of VEGF and CA125 was 160.8 pg/ml and 100.4 ku/l. These results indicate that the prognosis of adenomyosis can be predicted according to the optimal cut-off value of the serum levels of VEGF and CA125.
Figure 1.
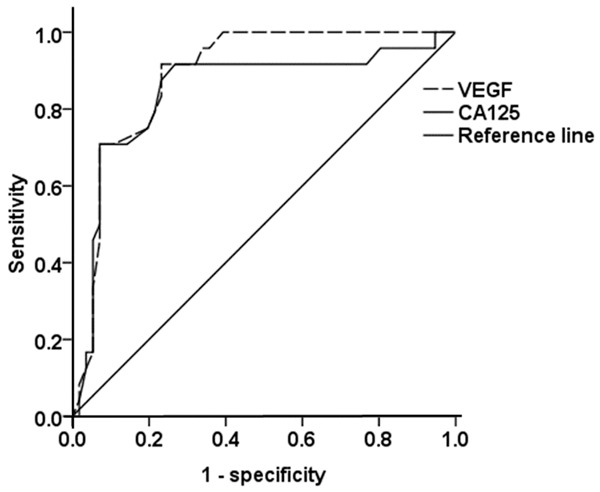
ROC analysis for analyzing the treatment effect on adenomyosis. ROC analysis was analysis the treatment effect of interventional therapy on adenomyosis according to the levels of VEGF and CA125 in serum. The area under ROC curve was 88.8% and 84.6% for the serum levels of VEGF and CA125, respectively. The optimal cut-off value of the serum levels of VEGF and CA125 was 160.8 pg/ml and 100.4 ku/l.
Progression-free survival analysis for the prognosis of adenomyosis
To evaluate the role of VEGF and CA125 for the prognosis of adenomyosis patients, Kaplan-Meier method was performed to analyze the progression-free survival of patients. A total of 80 patients were followed up 12 months after interventional therapy. Based on the serum levels of VEGF and CA125 before surgery, the median levels of VEGF and CA125 were 168 pg/ml and 110 ku/l, respectively. There were 39 patients with serum VEGF level ≥ 168 pg/ml and 41 patients with serum VEGF level < 168 pg/ml. There were 35 patients with serum CA125 level ≥ 110 ku/l and 45 patients with serum CA125 level < 110 ku/l. As shown in Figure 2, survival rate of patients with more than median levels of VEGF and CA125 was significantly lower than that with less than median levels of VEGF and CA125 (P < 0.05). These results indicate that the survival rate of adenomyosis patients with high VEGF and CA125 levels is decreased. The prognosis of these patients is poor.
Figure 2.
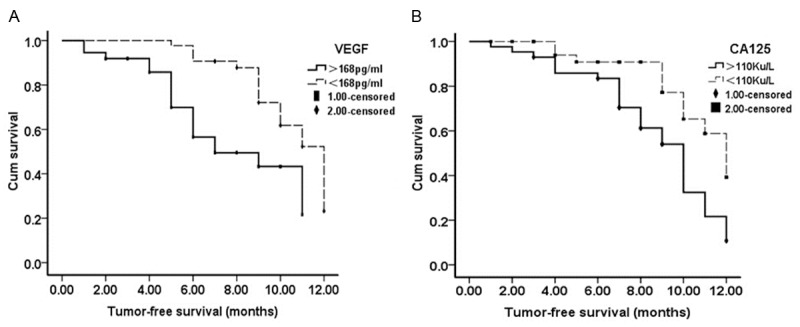
Progression-free survival analysis for the prognosis of adenomyosis. Kaplan-Meier method was performed to analyze the progression-free survival rate for the prognosis of adenomyosis patients according to the levels of VEGF and CA125 in serum. A total of 80 patients were followed up 12 months after interventional therapy. Based on the serum levels of VEGF and CA125 before surgery, the median levels of VEGF and CA125 were 168 pg/ml and 110 ku/l, respectively.
Discussion
The expression levels of VEGF and CA125 are closely related to the occurrence and development of adenomyosis. The activity of angiogenesis in endometrium and muscularis of adenomyosis patients is significantly increased [12]. Previous studies showed that the effect of interventional therapy on adenomyosis is closely related to the volume of uterus. The serum levels of CA125 are continuously decreased after interventional therapy [13,14]. In this study, our results showed that serum levels of VEGF and CA125 were gradually decreased after interventional therapy. After embolotherapy, the supply of nutrients for the uterine muscle fiber cells was blocked, which lead to the necrosis of ectopic endometrial, thereby reducing the volume of uterine, menstrual flow, and alleviating dysmenorrheal.
The remission rate of interventional therapy reached 100%. In patients with adenomyosis, the source of VEGF and CA125 expression is different. The specificity is not high for the detection of serum CA125 alone. Complicate analysis of VEGF and CA125 serum levels can improve the specificity and sensitivity for the prognosis of adenomyosis and evaluation of treatment effect. High expression levels of VEGF and CA125 indicate a poor prognosis [15]. Therefore, by making effective assessment of serum levels VEGF and CA125 preoperatively, the clinical value of these molecular markers can be greatly improved.
Progression-free survival analysis results showed that survival rate of patients with more than median levels of VEGF and CA125 was significantly lower than that with less than median levels of VEGF and CA125. These results indicate that survival rate of adenomyosis patients is closely related to the serum expression levels of VEGF and CA125. The survival rate of adenomyosis patients with high VEGF and CA125 levels is decreased. The prognosis of these patients is poor. ROC analysis results showed that the area under ROC curve was 88.8% and 84.6% for the serum levels of VEGF and CA125, respectively. The critical value is similar to the median levels of VEGF and CA125 in serum. The threshold of the optimal cut-off value had a high sensitivity and specificity. These results suggest that detection of serum levels of VEGF and CA125 have a high sensitivity and specificity for the prognosis of adenomyosis. The clinical diagnosis of the disease by the detection of serum levels of VEGF and CA125 has important guiding significance.
In conclusion, the serum expression levels of VEGF and CA125 are related to the development of adenomyosis. VEGF and CA125 serum levels may be used for predicting the prognosis of adenomyosis.
Acknowledgements
This work was supported by the fund of Department of Education in Inner Mongolia Autonomous Region (Grant No. NJ09166).
Disclosure of conflict of interest
None.
References
- 1.Bai H, Zhao LY. Progress in the etiology and pathogenesis of adenomyosis. Chinese Journal of Clinical Obstetrics and Gynecology. 2003;4:460–463. [Google Scholar]
- 2.Revel A. Multitasking human endometrium: a review of endometrial biopsy as a diagnostic tool, therapeutic applications, and a source of adult stem cells. Obstet Gynecol Surv. 2009;64:249–57. doi: 10.1097/OGX.0b013e318195136f. [DOI] [PubMed] [Google Scholar]
- 3.Taran FA, Stewart EA, Brucker S. Adenomyosis: Epidemiology, Risk Factors, Clinical Phenotype and Surgical and Interventional Alternatives to Hysterectomy. Geburtshilfe Frauenheilkd. 2013;73:924–931. doi: 10.1055/s-0033-1350840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ushio-Fukai M, Urao N. Novel role of NADPH oxidase in angiogenesis and stem/progenitor cell function. Antioxid Redox Signal. 2009;11:2517–33. doi: 10.1089/ars.2009.2582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Beckmann R, Houben A, Tohidnezhad M, Kweider N, Fragoulis A, Wruck CJ, Brandenburg LO, Hermanns-Sachweh B, Goldring MB, Pufe T, Jahr H. Mechanical forces induce changes in VEGF and VEGFR-1/sFlt-1 expression in human chondrocytes. Int J Mol Sci. 2014;15:15456–74. doi: 10.3390/ijms150915456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jin X, Liang B, Chen Z, Liu X, Zhang Z. The dynamic changes of capillary permeability and upregulation of VEGF in rats following radiation-induced brain injury. Microcirculation. 2014;21:171–7. doi: 10.1111/micc.12103. [DOI] [PubMed] [Google Scholar]
- 7.Abe Y, Ozaki Y, Kasuya J, Yamamoto K, Ando J, Sudo R, Ikeda M, Tanishita K. Endothelial progenitor cells promote directional three-dimensional endothelial network formation by secreting vascular endothelial growth factor. PLoS One. 2013;8:e82085. doi: 10.1371/journal.pone.0082085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Toyabe S, Seki S, Iiai T, Takeda K, Shirai K, Watanabe H, Hiraide H, Uchiyama M, Abo T. Requirement of IL-4 and liver NK1+ T cells for concanavalin A-induced hepatic injury in mice. J Immunol. 1997;159:1537–42. [PubMed] [Google Scholar]
- 9.Kraśnicki D. Serum and peritoneal fluid CA-125 concentration in women with endometriosis. Ginekol Pol. 2001;72:1365–9. [PubMed] [Google Scholar]
- 10.Kaneko Y, Harada M, Kawano T, Yamashita M, Shibata Y, Gejyo F, Nakayama T, Taniguchi M. Augmentation of Valpha14 NKT cell-mediated cytotoxicity by interleukin 4 in an autocrine mechanism resulting in the development of concanavalin A-induced hepatitis. J Exp Med. 2000;191:105–14. doi: 10.1084/jem.191.1.105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bonder CS, Ajuebor MN, Zbytnuik LD, Kubes P, Swain MG. Essential role for neutrophil recruitment to the liver in concanavalin A-induced hepatitis. J Immunol. 2004;172:45–53. doi: 10.4049/jimmunol.172.1.45. [DOI] [PubMed] [Google Scholar]
- 12.Han Y, Zhou Y, Zheng S. Study on the expression of vascular endothelial growth factor in patients with adenomyosis of the uterus. Zhonghua Fu Chan Ke Za Zhi. 2002;37:539–41. [PubMed] [Google Scholar]
- 13.Kremer M, Hines IN, Milton RJ, Wheeler MD. Favored T helper 1 response in a mouse model of hepatosteatosis is associated with enhanced T cell-mediated hepatitis. Hepatology. 2006;44:216–27. doi: 10.1002/hep.21221. [DOI] [PubMed] [Google Scholar]
- 14.Jing GM, Han JL, Zhu YH. The Clinical Value of Serum CA125 and PRL in the Treatment of Adenomyosisby Interventional Therapy. Chinese Journal of Hemorheology. 2007;17:142–143. [Google Scholar]
- 15.Karavasilis V, Malamou-Mitsi V, Briasoulis E, Tsanou E, Kitsou E, Pavlidis N. Clinicopathologic study of vascular endothelial growth factor, thrombospondin-1, and microvessel density assessed by CD34 in patients with stage III ovarian carcinoma. Int J Gynecol Cancer. 2006;16(Suppl 1):241–6. doi: 10.1111/j.1525-1438.2006.00316.x. [DOI] [PubMed] [Google Scholar]