

Abstract
Pakistan's National Tuberculosis Control Programme (NTP) is missing data on many tuberculosis (TB) cases who visit private providers. A survey on the incidence and under-reporting of TB in Pakistan provided a database for exploring the investigation and referral of presumptive TB cases by private health providers. The survey showed that private health providers requested both sputum smear and X-ray for diagnostic investigations. Of 2161 presumptive TB cases referred, 1189 (55%) were sent for investigations to a district NTP TB centre, of whom only 314 (26.4%) were registered. This indicates an urgent need to strengthen the link between private health providers and NTP to enhance TB notification.
Keywords: tuberculosis, diagnoses, referral, case detection
Abstract
Le Programme national de lutte contre la tuberculose (PNT) du Pakistan manque de nombreux cas de tuberculose (TB) soignés par des prestataires de soins privés. Une enquête sur l'incidence et la sous-déclaration de la TB au Pakistan a fourni une base de données afin d'explorer les investigations réalisées en cas de présomption de TB et leur référence par les prestataires de soins privés. L'enquête a montré que les prestataires privés demandaient à la fois un frottis de crachats et une radiographie pour le diagnostic. Sur 2161 cas suspects de TB référés, 1189 (55%) ont été envoyés pour investigations à un centre anti-tuberculeux de district (PNT), parmi lesquels seulement 314 (26,4%) ont été enregistrés. Ceci met en évidence le besoin urgent de renforcer les liens entre les prestataires privés et les PNT afin d'améliorer la déclaration de la TB.
Abstract
En el Programa Nacional contra la Tuberculosis (PNT) del Pakistán se están pasando por alto muchos casos de tuberculosis (TB) que acuden a los profesionales del sector privado. A partir de una encuesta sobre la incidencia de TB y la tasa de subnotificación en el país, se examinó la investigación de los casos y la remisión de las personas con presunción diagnóstica de TB por parte de los profesionales del sector privado. Se puso en evidencia que en el sector privado, los profesionales investigan la TB mediante la solicitud de la baciloscopia del esputo y además la radiografía de tórax. De los 2161 casos referidos por presunción diagnóstica, 1189 (55%) se remitieron para estudio al centro distrital PNT de TB y de ellos solo se registraron 314 (26,4%). Estos resultados indican la urgencia que existe de fortalecer los vínculos entre los profesionales del sector privado y el PNT, con el fin de mejorar la notificación de los casos de TB.
According to the 2013 World Health Organization (WHO) global tuberculosis (TB) report, Pakistan has an estimated TB prevalence of 376 per 100 000 population, and an incidence of 231/100 000, giving a case detection rate of 65% for all types of TB cases.1 The most important challenges to TB control in Pakistan are a lack of community involvement, limited engagement of the private sector and increasing numbers of multidrug-resistant TB (MDR-TB) cases.2
Private providers in Pakistan contributed 21% of TB notifications in 2012;1 however, research shows that 75% of detected cases in Pakistan first sought help from a private provider.3 Case reporting (notification) can be improved by encouraging all those care providers not involved with the National Tuberculosis Control Programme (NTP) to work with the NTP (public-private mix approach).3,4 Involving private providers is often difficult and is associated with many challenges, such as low socio-economic status of the country, alternative and informal providers, level of commitment to public health among private providers and low motivation among many general practitioners.3
A recent study that identified TB cases among all non-NTP sectors in 12 districts of Pakistan showed that only 73% of cases were notified to the NTP, 27% of cases identified were not reported to the NTP and 32% of all identified cases were diagnosed in the non-NTP sector.5
The present study aimed to explore the investigation and referral practices of private providers in the management of presumptive TB cases.
STUDY POPULATION AND METHODS
In a recent study in Pakistan that assessed TB prevalence in both the public and private sectors,5 a prospective longitudinal surveillance system was established among all non-NTP private and public providers in a random sample of 12 districts from January to March 2012: 3674 non-NTP facilities in the selected districts were mapped and consenting private health providers were enrolled. Modified suspect and laboratory registers were provided to record all presumptive TB cases and their management, without changing their routine practice. The facilities were visited weekly by field officers and district TB coordinators (DTCs) to check records, with instructions to collect missing names for accurate record linkage, evaluate the accuracy and notification status of TB cases and verify diagnoses per NTP criteria. The present study is an analysis of the subset of private health facilities from among all facilities that figure in the database. The current study focused on the practices of private health providers in the management of presumptive TB cases from the survey.
RESULTS
From January to March 2012, 3048 presumptive TB cases were identified by private health providers from 12 districts of Pakistan. Table 1 lists the districts with the number of presumptive TB cases detected by private health providers. Table 2 shows the manner in which the presumptive TB cases were investigated by the private health providers: 39.3% were referred for both sputum smear and X-ray, 19.6% were referred only for sputum smear examination, 24% were referred for X-ray only, 0.5% were referred for culture and 16.6% of cases were referred for other tests.
TABLE 1.
Population and presumptive TB cases detected by private health providers in selected districts participating in a survey in Pakistan, January–March 2012
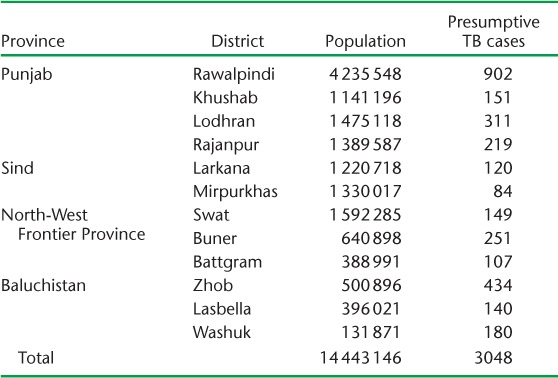
TABLE 2.
Investigation and referral of presumptive TB cases in selected districts managed by private health providers participating in a survey in Pakistan, January–March 2012

Private health providers treated 29.1% of the presumptive TB cases, while the remainder (n = 2161) were referred. Of the referred cases, 55% were referred for diagnosis to NTP diagnostic centres, 27.8% were referred to non-NTP private laboratories and 15% were referred to non-NTP public laboratories (Table 2). Among referred cases, only 314 (26.4%) were registered with the district TB centre (NTP). The majority of the cases (76.1%) were referred to confirm the diagnosis of TB.
Table 2 also shows the types of TB cases diagnosed by private health providers: 23.4% of the presumptive TB cases were diagnosed as smear-positive pulmonary TB, 16.9% were diagnosed as smear-negative pulmonary TB, and 4.5% were extra-pulmonary TB cases. Of the cases, 26.9% were diagnosed based on X-ray or other non-standard tests.
DISCUSSION
In Pakistan, the majority of private health providers manage TB cases that are often not notified to the NTP;5 effective control of TB in the country therefore requires greater collaboration between the private sector and the NTP. In this study, it was observed that a high proportion (39%) of private health providers prescribed both sputum microscopy and chest X-ray for TB diagnosis. Another study conducted in Karachi showed that only 20% of private health providers prescribe these examinations.6 This shows that TB control and management practices among private health providers in Pakistan are suboptimal, but that there is potential for scaling up public-private mix. To avoid development of drug resistance, the case management practices of private health providers need to be better focused and follow national guidelines.7
Another important finding of the study was that private health providers referred the majority (70.9%) of all presumptive TB cases and treated only 29.1%. Of the presumptive TB cases who were referred, 55% were referred for diagnosis to district NTP TB centres; however, as we were unable to trace all of them in the NTP registers, we do not know whether they actually attended the centres to which they had been referred. This problem needs to be resolved by strengthening the link between private health providers and the NTP. Private health providers in Pakistan do not always follow NTP guidelines for TB management, and the motivation of providers to manage TB in clinics varies.3,8 Proper training of private health providers and encouraging a public-private mix approach could reduce the observed under-reporting.
CONCLUSION
This study showed that many private health providers are treating TB cases without notifying them to the NTP, although they rely on NTP laboratories for diagnosis. The fact that private providers rely on smear microscopy as well as chest X-ray for diagnosis is promising and suggests that further training could help strengthen the public-private mix approach.
Acknowledgments
The authors are grateful to the implementers in the field for their efforts and to the University of Bergen, Bergen, Norway and the World Health Organization Eastern Mediterranean Office for funding for the main survey.
Footnotes
Conflict of interest: none declared.
References
- 1.World Health Organization. Global tuberculosis report, 2013. Geneva, Switzerland: WHO; 2013. WHO/HTM/TB/2013.11. [Google Scholar]
- 2.Vermund S H, Altaf A, Nawaz R S et al. Tuberculosis in Pakistan: a decade of progress, a future of challenge. J Pak Med Assoc. 2009;59(Suppl 1):S1–S8. [Google Scholar]
- 3.Naqvi S A, Naseer M, Kazi A et al. Implementing a public-private mix model for tuberculosis treatment in urban Pakistan: lessons and experiences. Int J Tuberc Lung Dis. 2012;16:817–821. doi: 10.5588/ijtld.11.0440. [DOI] [PubMed] [Google Scholar]
- 4.Quy H L, Lönnroth K, Buu T, Dieu T, Hai L. Public-private mix for improved TB control in Ho Chi Minh City, Viet Nam: an assessment on its impact on case detection. Int J Tuberc Lung Dis. 2003;7:464–471. [PubMed] [Google Scholar]
- 5.Fatima R, Harris R J, Enarson D A et al. Estimating tuberculosis burden and case detection in Pakistan. Int J Tuberc Lung Dis. 2013;18:55–60. doi: 10.5588/ijtld.13.0198. [DOI] [PubMed] [Google Scholar]
- 6.Ahmed M, Fatmi Z, Ali S, Ahmed J, Ara N. Knowledge, attitude and practice of private practitioners regarding TB-DOTS in a rural district of Sindh, Pakistan. J Ayub Med Coll Abbottabad. 2009;21:28–31. [PubMed] [Google Scholar]
- 7.Uplekar M. Involving private health care providers in delivery of TB care: global strategy. Tuberculosis (Edinb) 2003;83:156–164. doi: 10.1016/s1472-9792(02)00073-2. [DOI] [PubMed] [Google Scholar]
- 8.Khan J, Malik I A, Hussain I H, Ali I N, Akbani I F. Tuberculosis diagnosis and treatment practices of private physicians in Karachi, Pakistan. East Mediterr Health J. 2003;9:769–775. [PubMed] [Google Scholar]