

Abstract
Objectives. We examined internal and external determinants of state’s adoption of impaired driving laws.
Methods. Data included 7 state-level, evidence-based public health laws collected from 1980 to 2010. We used event history analyses to identify predictors of first-time law adoption and subsequent adoption between state pairs. The independent variables were internal state factors, including the political environment, legislative professionalism, government capacity, state resources, legislative history, and policy-specific risk factors. The external factors were neighboring states’ history of law adoption and changes in federal law.
Results. We found a strong secular trend toward an increased number of laws over time. The proportion of younger drivers and the presence of a neighboring state with similar laws were the strongest predictors of first-time law adoption. The predictors of subsequent law adoption included neighbor state adoption and previous legislative action. Alcohol laws were negatively associated with first-time adoption of impaired driving laws, suggesting substitution effects among policy choices.
Conclusions. Organizations seeking to stimulate state policy changes may need to craft strategies that engage external actors, such as neighboring states, in addition to mobilizing within-state constituencies.
Recent estimates suggest that as many as 20 000 people in the United States are killed annually in motor vehicle crashes because of a failure to adopt the full range of existing evidence-based approaches to enhance motor vehicle safety.1 Part of this policy gap may be explained by the wide variation in traffic safety laws across US states.2 Although there is considerable evidence that enhancing state laws and other policies on traffic safety can yield health dividends,3 there is little evidence explaining how and why states have approached the regulation of motor vehicle safety in such different ways.
Understanding the drivers of state policy variations could yield insights into numerous important questions. For instance, which state characteristics predict passage of new health laws and policies? How do external factors, such as the behaviors of neighboring states, influence state health policy adoption and diffusion? Do states that have strong laws in a particular health area (e.g., tobacco) also have strong laws in other areas (e.g., alcohol)? Following Louis Brandeis’s claim that states could serve as the learning laboratories of democracy,4 researchers have investigated state action on such things as lotteries, abortion,5 education reform,6 same-sex marriage,7 and the death penalty,8 creating a rich literature to explain how and why states take action.
In the majority of these studies, single policies have been examined without reference to other policies targeting the same issue or behavior. Few studies have investigated the adoption of multiple laws within a single policy domain or how action in a single policy area might facilitate (or complicate) the adoption of laws in another. Neglecting a state’s prior legislative actions to address an issue may obscure patterns and predictors of policy adoption for new policies. As a result, the generalizability of studies of specific determinants of policy diffusion may be limited.
We have argued elsewhere that patterns of state health policy adoption need to be understood as more than simply a response to emerging evidence from the scientific community.9 Variation in state responses may reflect their experience in using different policy tools within a single domain, government agency cooperation across state boundaries for mutual benefit, or long-term learning about the effectiveness of different policy tools that is later extended to new health issues.10 A state’s position as an early policy adopter or laggard may also vary by policy issue, contributing to the complex and often fragmented health policy environment encountered in many states.
We tested several hypotheses about the adoption and diffusion of state policy by examining laws related to impaired driving. Impaired driving laws reflect public health priorities because of the burden of deaths and injuries stemming from motor vehicle crashes in which alcohol or other drugs are involved.11 These laws are also a particularly useful case because driving under the influence of alcohol is illegal in all states; what differs is how states choose to approach this public health challenge.
We examined several impaired driving laws, including the definition of legal blood alcohol content levels, setting a lower blood alcohol content limit for underage drivers (often known as zero tolerance laws), prohibiting open alcoholic beverage containers in motor vehicles, charging mandatory fines for driving under the influence violations, applying civil penalties such as mandatory community service, and mandating criminal penalties such as jail time (detailed description available as a supplement to the online version of this article at http://www.ajph.org). Although these approaches are intended to discourage and sanction impaired driving, the presence of any or all of them, the extent to which they are discretionary or mandatory, and the amount of fines, length of jail terms, and amount of community service differ among states and within states over time.
We included blood alcohol content of 0.08 and zero tolerance laws as special cases in which federal legislation and incentives eventually influenced all states to adopt these provisions by 1998 and 2006, respectively. We selected these laws because there is empirical evidence of their public health impact, data on state adoption were available for the entire study period, and there was sufficient state-to-state diffusion by the end of the study period.
We defined policy adoption as taking place when a state legislature enacted a new law or, in the case of penalties, substantially modified an existing one (e.g., increasing fines), and we limited our analysis to evidence-based laws that were actually passed (as opposed to proposed). We defined policy diffusion as the spread of an evidence-based law to other states after having been adopted by the first state (or states).
We tested the following hypotheses regarding state health policy adoption and diffusion:
The policy hurdle hypothesis. The theory of punctuated equilibrium suggests that most policy change is incremental, with infrequent periods of dramatic shifts in actors and institutions that permit large-scale change.12 Thus, we hypothesized that the factors associated with any particular state’s likelihood to pass the first policy in a particular area would be different from those associated with the state’s likelihood to pass additional policies after they had passed this first policy hurdle.
The political context hypothesis. Although health issues such as abortion and gun control have generated vigorous national debate and intense political partisanship, many public health policies fly below the radar of political party priorities. We hypothesized that for health issues that do not have strong national resonance in political platforms, state political ideology, level of government professionalism, and congruence among parties within the state legislature would not be associated with their adoption.
The shared geography hypothesis. Much of the literature on state policy diffusion focuses on cooperation and competition between states, either to attract more business or to avoid attracting welfare recipients.13 Public health policy may be less explicitly tied to economic cooperation or competition, but there are important instances in which states have an incentive to work together, such as when they share a highway, have large bordering cities or have the potential for cross-border purchasing of such products as alcohol. We hypothesized that diffusion among neighboring states is likely to occur for policies that have potential spillover effects.
The policy silo hypothesis. Policy learning is often framed in the context of states learning from other states. However, it is also possible that a state may learn from having passed similar laws affecting a different health domain (e.g., applying lessons from alcohol excise taxes to those on cigarettes), and public health leaders have begun to encourage such cross-issue thinking about regulation.14 Yet in the public health field, advocacy communities have been devoted to specific health issues or problems, with deep expertise in a single area. We hypothesized that previous state policy actions in a single health area are unlikely to influence policy adoption in a different heath area.
The policy appetite hypothesis. There is extensive literature that seeks to explain why some government bodies are at the forefront of change whereas others are locked into a path they adopted early on.15 We hypothesized that states with more policies at any particular time would be the most likely to continue to pass subsequent policies, regardless of measurable internal characteristics.
METHODS
We used event history analysis to model patterns and predictors of policy adoption in each state. In this model, we considered all states at risk for adopting the policy under analysis.16 Conveniently, once data are properly set up, event history models with time-varying covariates can be estimated via logistic regression.17 The basic model for state i in year t is
 |
where ρ is the probability of adoption of any specific policy in state i at year t, x is a time-varying covariate (i.e., demographics, resources, political characteristics), z is a fixed covariate (i.e., geographic region), β and γ are their respective coefficients, and α is the intercept. To account for repeat observations of each state, we estimated the model using robust SEs (clustered on each state), and we controlled duration dependence by including linear and quadratic terms for time.18 To account for geographic clustering, we included a term to represent the 9 US census divisions.
We modified the data to contain directed dyads, which consisted of a panel of state pairs for each year. Thus, the units of analysis were state dyad–years. This approach allowed us to compare each state with every other state, meaning that each state could serve as both a sender and a receiver of any particular law and that we could assess the contribution of different state characteristics in terms of their contribution to the likelihood of a state learning from or emulating the other state in its dyad.19
We assessed first-time adoption using single-failure approaches for each law. As in survival analysis, subjects (in this case, states) drop out of the analysis once they are no longer at risk. Traditionally this is because of death or loss to follow-up. In our analysis, states dropped out of the risk set once they adopted the policy in question.
We modeled subsequent law adoption using a repeated-failures context in which states remained in the risk set as long as any additional policy adoptions were still possible. We sought to identify factors that helped explain why some states adopted a larger number of policies and others did not.
Finally, to illustrate the substantive meaning of regression models, we plotted predicted probabilities combining the main variables found to be significant in first-time and subsequent law adoption.
We abstracted data on all state health laws and other state characteristics from the State Health Policy Research Dataset, a publicly available data set that combines extensive secondary data sources with original legal research.20 State health laws included only those with empirical evidence of their public health impact (data available as a supplement to the online version of this article at http://www.ajph.org). We derived other data from existing secondary sources, including the US Census. We took motor vehicle fatalities for each state and year from the Fatality Analysis Reporting System; these are expressed as fatalities per vehicle miles traveled.
All regression models controlled for a set of internal state population factors affecting impaired driving risks (alcohol consumption), demographic risk factors (younger driving population of those aged 15 to 24 years, natural logarithm of the state population size), factors affecting driving volume (unemployment rates, miles of road per capita), regional effects (dummy variables for the 9 US census divisions), and the overall motor vehicle fatality rate.
To test the policy hurdle hypothesis we examined whether the range of internal predictors (including political context variables) differed between first and subsequent adoption models.
We tested the political context hypothesis by assessing the contribution of state political factors to either first or subsequent policy adoption. We measured state policy context by (1) whether branches of state government were politically unified (i.e., the governor and majority party in power in all state legislative houses were the same), operationalized with unified Democrats functioning as the reference category; (2) state political ideology (measured using Berry’s21 state policy scales, in which 0 represents the most conservative and 100 the most liberal); (3) legislative professionalism (measured using the Squire index derived from variables including length of time in session, payment for legislators, professional staff)22; and (4) government capacity and resources (measured using a proxy of total tax revenue per capita).
We assessed the shared geography hypothesis by measuring neighboring states’ history of prior (related) law adoption, operationalized as the proportion of those states that previously adopted the particular health law.
To test the policy silo hypothesis, we included the presence of any (1-year lagged) state smoking, alcohol, or motor vehicle occupant law. These variables (description available as a supplement to the online version of this article at http://www.ajph.org) included laws in similar domains (driving safety laws, e.g., graduated drivers licenses; motor vehicle occupant safety laws, e.g., those requiring seatbelts or infant car seats), alcohol regulations (beer tax rate, Sunday sales bans, keg registration), and laws in other public health domains, such as those that regulate smoking (clean indoor air laws, cigarette taxes).
We tested the policy appetite hypothesis 2 ways. First, we tested the significance of a newly updated measure of state innovativeness that Boehmke and Skinner23 derived from a long time series of the proportion of more than 180 public policies adopted by each state each year since 1912. Second, we tested the significance of a measure of the state’s legislative history (the number of policies regulating impaired driving previously adopted) in models examining subsequent adoption of impaired driving policies.
We built models sequentially and added new blocks of variables to test subsequent hypotheses. We used fit statistics (Akaike information criterion and Bayesian information criterion) to determine whether additional blocks of variables improved model fit. We carried out our analyses using Stata version 13.1 (StataCorp LP, College Station, TX).
RESULTS
Figure 1 displays the number of states adopting laws on alcohol-impaired driving over the 30-year study period. State adoption of all laws increased over the study period. Overall, the pattern of state adoption varied by law, and only 2 laws (blood alcohol content of 0.08 and zero tolerance) were eventually adopted by all states.
FIGURE 1—
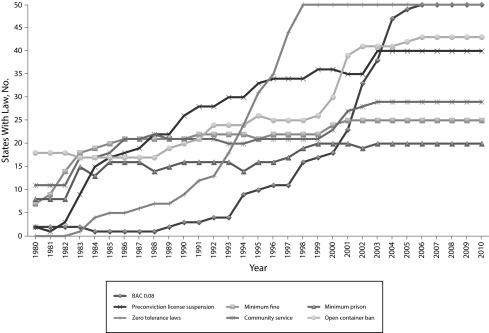
Number of states with alcohol-impaired driving policies, by policy and year: US states, 1980–2010.
Note. BAC = blood alcohol content; DUI = driving under the influence (of alcohol). BAC = 0.08 means that BAC ≥ 0.08; community service refers to mandatory community service for DUI; minimum fine refers to the minimum fine for DUI; minimum prison refers to minimum prison days for DUI; open container ban refers to ban on open alcoholic containers in motor vehicles; preconviction refers to license suspension for DUI (preconviction); zero tolerance laws refers to lower BAC for drivers younger than 21 years.
Source. Silver and Macinko, State Health Policy Research Dataset (SHEPRD): 1980–2010.20
Table 1 presents the variable means and SDs at 4 points in time. Although overall population size increased steadily over the 30-year period, the percentage of the population aged 15 to 24 years (the target of many of the laws) declined significantly from 1980 to 2000, leveling in 2010. Consistent with national trends, state unemployment dropped significantly between 1990 and 2000 and then grew significantly until 2010. The average state motor vehicle fatality rate (per vehicle miles traveled) declined significantly each decade, dropping by two thirds over the period, whereas state averages of gallons of alcohol consumed per capita declined between 1980 and 2000 but increased again by 2010.
TABLE 1—
Mean (SD) and Number of States of Study Variables: United States, 1980–2010
| Variable | 1980 Mean (SD) or No. States | 1990 Mean (SD) or No. States | 2000 Mean (SD) or No. States | 2010 Mean (SD) or No. States |
| Population, aged 15–24 y, % | 19.18 (0.95) | 14.77*** (0.99) | 14.39* (1.31) | 14.09 (0.87) |
| Unemployment rate, % | 6.48 (1.86) | 5.76 (1.27) | 3.90*** (0.94) | 8.84*** (2.04) |
| MVC death rate per 100 million VMT | 3.54 (0.78) | 2.15*** (0.49) | 1.60*** (0.43) | 1.13*** (0.37) |
| Alcohol consumption, gallons per capita | 2.81 (0.80) | 2.47*** (0.57) | 2.25*** (0.45) | 2.52*** (0.47) |
| Unified Republican | 4 | 4 | 15* | 10* |
| Unified Democrat | 19 | 16 | 9 | 14 |
| Divided government | 27 | 30 | 26 | 26 |
| Liberal state ideology, 0–100 | 42.43 (15.95) | 48.39*** (13.15) | 43.25*** (14.66) | 49.44*** (15.21) |
| Squire index | 0.21 (0.10) | 0.22 (0.14) | 0.18 (0.12) | 0.19 (0.13) |
| Tax revenues per capita | 655.21 (471.41) | 768.15*** (241.70) | 922.19*** (192.63) | 978.59 (381.17) |
| Policy innovativeness score | 1.68 (1.42) | 3.62** (3.08) | 8.71*** (5.38) | 8.25 (17.42) |
| Any smoking policies | 1 | 39* | 46 | 50 |
| Any motor vehicle safety policies | 5 | 26 | 40 | 48 |
| Any alcohol policies | 28 | 50* | 50 | 50 |
Note. MVC = motor vehicle crash; VMT = vehicle miles traveled.
*P < .05; **P < .01; ***P < .001.
Between 1990 and 2000, the number of states with unified Republican governments grew significantly, from 4 to 15, and dropped again in 2010, to 10. The number of states in which the legislature and governor were of different political parties remained fairly constant at about half through the study period. Between 1980 and 1990, state ideology became significantly more liberal, became less liberal between 1990 and 2000, and became more liberal again by 2010. The level of state government professionalism, measured by the Squire index, changed negligibly throughout the period, whereas tax revenues per capita grew steadily until 2000, with only a small (and not statistically significant) increase in 2010. The policy innovativeness score rose dramatically from 1980 to 2000 and then declined slightly from 2000 to 2010. Finally, public health policies regulating smoking, alcohol, and motor vehicle safety all increased significantly from 1980 to 1990, with most states having at least 1 policy in each area by 2000.
Table 2 presents results from models predicting first-time state policy adoption. As seen in the baseline model, the proportion of the population aged 15 to 24 years was positively associated with first-time adoption of impaired driving laws, conditional on other covariates. Political variables such as a Republican or divided government, measures of legislative professionalism, and government resources (taxes per capita) were not significant. The number of state neighbors with similar alcohol-impaired driving regulations was associated with a 12% greater odds that a state will adopt such a law. The presence of any previous alcohol policy was inversely related to the state’s enactment of its first impaired driving laws. This relationship persisted in the next model, for which measure of the overall state innovativeness with respect to nonpublic health laws was not significant.
TABLE 2—
Predictors of First-Time Adoption of Impaired Driving Laws: US States, 1980–2010
| Variable | Baseline Model (n = 5232), OR (95% CI) | Political Hypothesis (n = 5232), OR (95% CI) | Neighbor Hypothesis (n = 5232), OR (95% CI) | Policy Silo Hypothesis (n = 5232), OR (95% CI) | Innovativeness Hypothesis (n = 5206), OR (95% CI) |
| Population aged 15–24 y, % | 1.18* (1.03, 1.35) | 1.21* (1.03, 1.42) | 1.23* (1.04, 1.45) | 1.20* (1.03, 1.41) | 1.29* (1.03, 1.41) |
| Unemployment rate, % | 1.01 (0.94, 1.07) | 1.01 (0.94, 1.08) | 1.01 (0.95, 1.09) | 1.02 (0.96, 1.09) | 1.02 (0.96, 1.09) |
| Risk factors, MVC deaths per 1000 population | 1.01 (0.98, 1.03) | 1.00 (0.96, 1.03) | 0.99 (0.96, 1.03) | 0.99 (0.95, 1.02) | 0.99 (0.95, 1.02) |
| Health behaviors, alcohol consumption | 0.96 (0.71, 1.32) | 0.97 (0.69, 1.36) | 0.98 (0.70, 1.36) | 0.98 (0.68, 1.42) | 0.98 (0.68, 1.43) |
| Unified Republican government | 0.82 (0.32, 2.11) | 0.87 (0.34, 2.25) | 0.88 (0.35, 2.23 | 0.88 (0.34, 2.24) | |
| Divided government | 1.1 (0.68, 1.77) | 1.13 (0.70, 1.84) | 1.14 (0.70, 1.84) | 1.14 (0.70, 1.86) | |
| Liberal state ideology (0–100) | 1.01 (0.98, 1.03) | 1.01 (0.98, 1.04) | 1.01 (0.98, 1.03) | 1.01 (0.98, 1.03) | |
| Squire index | 1.2 (0.87, 1.66) | 1.23 (0.87, 1.73) | 1.2 (0.87, 1.66) | 1.19 (0.86, 1.66) | |
| Log tax per capita, $1000 | 0.78 (0.45, 1.36) | 0.8 (0.45, 1.42) | 0.71 (0.39, 1.28) | 0.71 (0.39, 1.29) | |
| Neighbors with the same policy | 1.12* (1.02, 1.22) | 1.13** (1.04, 1.24) | 1.13** (1.04, 1.23) | ||
| Has any smoking policies | 0.79 (0.55, 1.13) | 0.79 (0.56, 1.13) | |||
| Has any alcohol policies | 0.41*** (0.29, 0.58) | 0.41*** (0.29, 0.59) | |||
| Has any motor vehicle occupant safety policies | 0.94 (0.66, 1.32) | 0.93 (0.66, 1.32) | |||
| Overall policy Innovativeness score | 1.03 (0.92, 1.16) | ||||
| Federal minimum legal drinking age of 21 y, 1988 | 0.31** (0.12, 0.83) | 0.32** (0.12, 0.86) | 0.32** (0.12, 0.85) | 0.37 (0.14, 0.99) | 0.38 (0.14, 1.00) |
| AIC | 2224.896 | 2229.677 | 2225.454 | 2209.111 | 2202.806 |
| BIC | 2290.522 | 2328.115 | 2330.454 | 2333.799 | 2333.957 |
Note. AIC = Akaike information criterion; BIC = Bayesian information criterion; CI = confidence interval; MVC = motor vehicle crash; OR = odds ratio. Models also control for log population size, miles of road per capita, time, time2, and geographic divisions.
*P < .05; **P < .01; ***P < .001.
Table 3 presents results from our analyses of additional laws on impaired driving, conditional on first adoption. Of the state’s internal conditions, only alcohol consumption was significantly and positively associated with likelihood of repeat impaired driving law adoption. State political resources and orientation were not significant. A state’s neighbor’s passage of an impaired driving law increased the odds that a state would adopt the same law by 23%, conditional on other covariates. Each previous law that the state adopted in the domain increased the odds of subsequent adoption by 97%. However, neither the presence of additional public health laws nor state policy innovativeness was associated with subsequent adoption of impaired driving laws.
TABLE 3—
Predictors of Repeat Adoption: US States, 1980–2010
| Variable | Baseline Model (n = 10 500), OR (95% CI) | Political Hypothesis (n = 10 500), OR (95% CI) | Neighbor Hypothesis (n = 10 500), OR (95% CI) | Policy Silo Hypothesis (n = 10 500), OR (95% CI) | Innovativeness Hypothesis (n = 10 381), OR (95% CI) |
| Population aged 15–24 y, % | 1.01 (0.85, 1.20) | 1.01 (0.86, 1.17) | 1.01 (0.86, 1.19) | 1.04 (0.94, 1.15) | 1.04 (0.94, 1.15) |
| Unemployment rate, % | 1.05 (0.98, 1.12) | 1.05 (0.98, 1.12) | 1.06 (0.99, 1.14) | 1.04 (1.00, 1.08) | 1.04 (1.00, 1.08) |
| Risk factors, MVC deaths per 1000 population | 1.00 (0.97, 1.04) | 0.99 (0.96, 1.03) | 0.99 (0.95, 1.03) | 0.98 (0.96, 1.01) | 0.99 (0.96, 1.01) |
| Health behaviors, alcohol consumption | 1.11 (0.75, 1.63) | 1.11 (0.76, 1.64) | 1.18 (0.82, 1.68) | 1.24* (1.01, 1.52) | 1.24* (1.01, 1.52) |
| Unified Republican government | 0.78 (0.45, 1.35) | 0.94 (0.51, 1.73) | 1.08 (0.71, 1.66) | 1.10 (0.72, 1.68) | |
| Divided government | 0.93 (0.68, 1.27) | 0.99 (0.70, 1.40) | 1.03 (0.84, 1.25) | 1.04 (0.85, 1.26) | |
| Liberal state ideology (0–100) | 0.99 (0.98, 1.01) | 1.00 (0.98, 1.02) | 1.00 (0.99, 1.02) | 1.01 (0.99, 1.02) | |
| Squire index | 0.89 (0.57, 1.40) | 0.90 (0.55, 1.49) | 1.09 (0.77, 1.56) | 1.10 (0.77, 1.56) | |
| Log tax per capita, $1000 | 1.14 (0.57, 2.27) | 1.29 (0.61, 2.74) | 1.12 (0.75, 1.66) | 1.10 (0.74, 1.63) | |
| Neighbors that have the same policy | 1.23*** (1.11, 1.37) | 1.30*** (1.18, 1.44) | 1.30*** (1.18, 1.44) | ||
| No. previous laws adopted | 1.97*** (1.81, 2.14) | 1.96*** (1.80, 2.13) | |||
| Has any smoking policies | 1.07 (0.81, 1.40) | 1.06 (0.81, 1.39) | |||
| Has any alcohol policies | 0.90 (0.72, 1.11) | 0.90 (0.72, 1.12) | |||
| Has any motor vehicle occupant safety policies | 1.18 (0.95, 1.46) | 1.18 (0.95, 1.46) | |||
| Overall policy innovativeness score | 1.02 (0.98, 1.06) | ||||
| Federal minimum legal drinking age of 21 y, 1988 | 1.05 (0.92, 1.20) | 1.05 (0.92, 1.20) | 0031.05 (0.91, 1.21) | 0.93 (0.84, 1.04) | 0.94 (0.85, 1.05) |
| AIC | 12 782.240 | 12 784.022 | 12 572.109 | 11 458.148 | 11 345.029 |
| BIC | 12 854.830 | 12 892.909 | 12 688.255 | 11 603.330 | 11 497.231 |
Note. AIC = Akaike information criterion; BIC = Bayesian information criterion; CI = confidence interval; MVC = motor vehicle crash; OR = odds ratio. Models also control for population size, miles of road per capita, time, time2, and geographic division.
*P < .05; ***P < .001.
Figure 2 displays the predicted probabilities of a state passing an impaired driving law for the first time and subsequently. Figure 2a demonstrates that the probability of the first law being adopted increases significantly with the presence of neighbors with impaired driving laws. That shrinks if the state already had an alcohol regulation in place (Figure 2b). Figure 2c demonstrates the importance of policy appetite and neighbors’ behaviors. The predicted probability of passing additional impaired driving laws increased with the presence of neighbors with similar laws, especially if the state itself had already passed 2 or more laws in this domain (Figure 2d).
FIGURE 2—

Predicted probabilities and 95% confidence intervals of impaired driving laws at (a) first adoption with no prior alcohol laws, (b) first adoption with ≥ 1 prior alcohol law, (c) subsequent adoption with < 2 prior impaired driving laws, and (d) subsequent adoption with ≥ 2 prior impaired driving laws: United States, 1980–2010.
DISCUSSION
We found substantial variation across states in the types of evidence-based policies they adopted to reduce impaired driving, with substantial gaps between states across the entire period. As a result of these gaps, states offer their residents very different levels of legal protection from the risks of impaired driving.
At the same time, our study confirms a strong secular trend toward greater regulation of impaired driving over time and support for several of our hypotheses regarding policy adoption and diffusion in this domain. The strongest predictors of adoption of new policies aimed at reducing impaired driving are pressures from neighboring states combined with past adoption of at least 1 policy in this arena, demonstrating strong support for the shared geography and policy appetite hypotheses.
We found that internal state population risk factors operate differently for first-time versus subsequent policy adoption in this arena, providing some evidence in support of the policy hurdle hypothesis. Thus, although we did not find the overall traffic-related fatality rate to predict policy adoption, the size of the population aged 15 to 24 years—the group most at risk for death and injury from impaired driving—was associated with first-time (but not repeated) policy adoption, suggesting that states might be initially more receptive to regulation when it involves protecting younger populations.
We also found limited evidence to support the policy silo hypothesis: policy action regulating either motor vehicle protections or tobacco was unrelated to action on impaired driving. However, alcohol regulations were negatively associated with first-time impaired driving policy adoption. One explanation for this might be a substitution effect: because of the limited time and attention policymakers can pay to any given topic, action on other aspects of alcohol regulation (particularly those targeted to youths drinking, e.g., keg registration, beer taxes) may substitute for action on impaired driving.
This approach could have positive health effects, but we have little evidence of how and why these types of tradeoffs might occur and even less information on their potential health impact. Another explanation may simply be that the variables for alcohol policy are picking up the effect of federal actions that took place in 1988 raising the legal minimum drinking age to 21 years. In any case, our findings suggest that assessing policy adoption patterns both within and across domains can illuminate how policy action in related arenas may accelerate or inhibit state policy adoption.
These results are consistent with those from studies suggesting that beginning in the 1980s, during the so-called era of new federalism, states increased the pace of policy adoption dramatically—across numerous economic and social realms—and that some of the major determinants were state population size, policy appetite, and neighboring state’s adoption.23 Although several studies have found that ideology, the political party in power, and the professionalism of the state government were predictors of whether new policies were adopted,24 we did not. This finding supports our hypothesis that drivers of ideologically noncontentious public health issues would be different from contentious ones. Our finding that the general measure of the state’s history of policy innovativeness did not predict policy adoption in impaired driving lends further support to this insight.
Limitations
This study has several limitations. The number of impaired driving laws is small, limiting the amount of policy adoption we could model. Our data set was limited to policies related to general deterrence (discouraging first-time impaired driving offenses) and did not include new technologies (e.g., ignition interlock for repeat offenders) introduced into a few states at the end of our study period. We did not include measures of local policies, and localities can and do impose additional fines and other sanctions for impaired driving.
To date, there are no comprehensive databases listing such local policies, and although there may be some evidence of bottom-up federalism the mechanisms identified are likely to be important beyond learning from influential localities to state governments. Finally, there is no guarantee that states with a greater number of laws on the books actually enforce these laws. Because enforcement data were lacking for most states, the relationship between enforcement and policy diffusion has not been well explored and is an area for further research.
Conclusions
The Institute of Medicine recently highlighted the potential of public policies to substantively improve the health of populations, saying they are among the most powerful tools available.25 The American Public Health Association, leading philanthropies in the field, and many national and state public health organizations have argued that strengthening the state public health environment means applying lessons learned in policymaking from one health arena to another. Our evidence suggests that there is still much work to do to overcome existing silos. Additional research testing these hypotheses in other policy domains may further our understanding of the drivers of public health policy adoption and contribute to moving evidence into policy across multiple health issues.
Acknowledgments
This work was supported by the National Institute of Alcohol Abuse and Alcoholism, National Institutes of Health (grants 1R01AA021436-0 and 1R21AA021523-01A1).
A previous version of this article was presented at the 2013 Association for Public Policy Analysis and Management conference.
Human Participant Protection
No protocol approval was necessary because no human participants were involved.
References
- 1.Evans L. Traffic fatality reductions: United States compared with 25 other countries. Am J Public Health. 2014;104(8):1501–1507. doi: 10.2105/AJPH.2014.301922. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Silver D, Macinko J, Bae JY, Jimenez G, Paul M. Variation in US traffic safety policy environments and motor vehicle fatalities 1980–2010. Public Health. 2013;127(12):1117–1125. doi: 10.1016/j.puhe.2013.10.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.National Highway Traffic Safety Administration. Countermeasures That Work: A Highway Safety Countermeasure Guide for State Highway Safety Offices. 7th ed. Washington, DC: 2013. [Google Scholar]
- 4. New State Ice Co. v. Liebmann, 285 US 262 (1932).
- 5.Mooney CZ, Lee M. Legislating morality in the American states: the case of pre-Roe abortion regulation reform. Am J Polit Sci. 1995;39(3):599–627. [Google Scholar]
- 6.Mintrom M, Vergari S. Policy networks and innovation diffusion: the case of state education reforms. J Polit. 1998;60(1):126–148. [Google Scholar]
- 7.Haider-Markel DP. Policy diffusion as a geographical expansion of the scope of political conflict: same-sex marriage bans in the 1990s. State Polit Policy Q. 2001;1(1):5–26. [Google Scholar]
- 8.Mooney CZ, Lee M. Morality policy reinvention: state death penalties. Ann Am Acad Polit Soc Sci. 1999;566:80–92. [Google Scholar]
- 9.Bae JY, Anderson ED, Silver D, Macinko J. Child passenger safety laws in the United States, 1978–2010: policy diffusion in the absence of strong federal intervention. Soc Sci Med. 2014;100:30–37. doi: 10.1016/j.socscimed.2013.10.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Macinko J, Silver D. Improving state health policy assessment: an agenda for measurement and analysis. Am J Public Health. 2012;102(9):1697–1705. doi: 10.2105/AJPH.2012.300716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.National Highway Traffic Safety Administration. Traffic Safety Facts 2009: A Compilation of Motor Vehicle Crash Data From the Fatality Analysis Reporting System and the General Estimates System. Washington, DC: US Department of Transportation; 2011. [Google Scholar]
- 12.Baumgartner FR, Jones BD. Agendas and Instability in American Politics. Chicago, IL: University of Chicago Press; 1993. [Google Scholar]
- 13.Schram SF, Soss J. Making something out of nothing: welfare reform and a new race to the bottom. Publius. 1998;28(3):67–88. [Google Scholar]
- 14.Pomeranz JL. Sugary beverage tax policy: lessons learned from tobacco. Am J Public Health. 2014;104(3):e13–e15. doi: 10.2105/AJPH.2013.301800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Wilsford D. Path dependency, or why history makes it difficult but not impossible to reform health care systems in a big way. J Public Policy. 1994;14(3):251–283. [Google Scholar]
- 16.Berry FS, Berry W. Innovation and diffusion models in policy research. In: Sabatier P, editor. Theories of the Policy Process. 2nd ed. Boulder, CO: Westview Press; 2007. pp. 169–200. [Google Scholar]
- 17.Box-Steffensmeier JM, Zorn CJW. Duration models and proportional hazards in political science. Am J Polit Sci. 2001;45(4):972–988. [Google Scholar]
- 18.Box-Steffensmeier JM, Zorn C. Duration models from repeated events. J Polit. 2002;64(4):1069–1094. [Google Scholar]
- 19.Volden C. States as policy laboratories: emulating success in the children’s health insurance program. Am J Polit Sci. 2006;50(2):294–312. [Google Scholar]
- 20.Silver D, Macinko J. State Health Policy Research Dataset (SHEPRD): 1980–2010. Ann Arbor, MI: Inter-University Consortium for Political and Social Research; 2013. [Google Scholar]
- 21.Berry WD, Fording RC, Ringquist EJ, Hanson RL, Klarner CE. Measuring citizen and government ideology in the US states: a re-appraisal. State Polit Policy Q. 2010;10(2):117–135. [Google Scholar]
- 22.Squire P. Measuring state legislative professionalism: the Squire index revisited. State Polit Policy Q. 2007;7(2):211–227. [Google Scholar]
- 23.Boehmke FJ, Skinner P. State policy innovativeness revisited. State Polit Policy Q. 2012;12(3):303–329. [Google Scholar]
- 24.Tung GJ, Vernick JS, Stuart EA, Webster DW. Political factors affecting the enactment of state-level clean indoor air laws. Am J Public Health. 2014;104(6):e92–e97. doi: 10.2105/AJPH.2013.301689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Institute of Medicine, Committee on Public Health Strategies to Improve Health. For the Public’s Health: Revitalizing Law and Policy to Meet New Challenges. Washington, DC: National Academies Press; 2011. [Google Scholar]