

Abstract
Background and Aims:
Regional anesthesia is a recommended technique for upper and lower limb surgeries with better postoperative profile. In this, randomized, double-blind study, we evaluated the effectiveness of the addition of dexmedetomidine to varying concentration of levobupivacaine for supra clavicular brachial plexus block.
Material and Methods:
After obtaining ethical Committee approval, a double-blind, randomized prospective clinical study was conducted on 90 American Society of Anesthesiologist Grade I and II patients in the age group of 18-55 years, divided randomly into two groups: Group A received 40 ml of solution containing 30 ml 0.5% levobupivacaine and 10 ml 1% lignocaine and group B received 40 ml of solution containing 30 ml 0.25% levobupivacaine and 10 ml 1% lignocaine with dexmedetomidine 1 microg/kg for supraclavicular brachial plexus block. Besides effectiveness, other parameters observed were: duration of sensory blockade; onset and duration of motor blockade; duration of postoperative analgesia; and patient satisfaction score.
Results:
Onset of sensory and motor blockade was 7.6 ± 1.006 min and 8.3 ± 0.877 min in group A, while it was 6.96 ± 1.077 min an 7.6 ± 1.1 min in group B, respectively. The difference was statistically significant (P < 0.05). Duration of sensory block was 8.5 ± 0.77 h in group A and 8.5 ± 0.98 in group B (P > 0.05). Duration of motor block was 8.45 ± 0.75 h in group A and 5.6 ± 0.98 in group B (P < 0.05). Duration of analgesia was 8.5 ± 0.77 h in group A and 9.2 ± 1.05 in group B (P < 0.05).
Conclusion:
Addition of 1 microg/kg dexmedetomidine to 0.25% levobupivacaine for supraclaviclar plexus block shortens sensory, motor block onset time and motor block durations, extends sensory block, and analgesia durations. Reduction in total levobupivacaine dose also increases the safety margin of the block.
Keywords: Dexmedetomidine, levobupivacaine, supraclavicular brachial plexus block
Introduction
Regional anesthesia is the recommended technique for upper and lower limb surgeries with better postoperative profile. Considerable research has been conducted over years in order to determine the ideal local anesthetic (LA) drug. An ideal drug should have a fast sensory onset, differential offset, with an earlier offset of motor than sensory blockade, enabling early ambulation/movements with prolonged analgesia. Several combinations of LAs and adjuvants such as tramadol,[1,2] sufentanyl,[2] clonidine,[2] and fentanyl[3] have been employed in the search for near ideal agent, which remains elusive. Currently, levobupivacaine (S(−)-enantiomer of bupivacaine) with favorable clinical profile and lesser cardiotoxicity when compared with racemic bupivacaine[4,5] is being favored LA for regional block.
Dexmedetomidine, an α2-receptor agonist, with α2/α1 selectivity 8 times than that of clonidine has also been reported to improve the quality of intrathecal and epidural anesthesia[6,7] when used along with LA as adjuvant.
In our current prospective, randomized, double-blind study we evaluated the effectiveness of the addition of dexmedetomidine to levobupivacaine for supraclavicular brachial plexus block. It was hypothesized that addition of dexmedetomidine 1 μg/kg to levobupivacaine will help to reduce the total dose of levobupivacaine required for supraclavicular brachial plexus block. Other primary objectives were to asses: onset and duration of sensory blockade; onset and duration of motor blockade; duration of postoperative analgesia; and patient satisfaction score (PSS). Secondary objectives assessed included: intraoperative narcotic requirement; hemodynamic changes; and any side-effects or complications.
Material and Methods
With Ethical Committee approval, a double-blind, randomized prospective clinical study was planned among 90 American Society of Anesthesiologist (ASA) Grade I and II patients in the age group of 18-55 years, posted for elective upper limb orthopedic surgeries under brachial plexus block using supraclavicular approach. Patients with diabetes, peripheral neuropathy, with known allergy to LAs, coagulopathy, infection at the site of block, pregnancy, and patients on beta blockers were excluded from the study.
Preoperatively patients were counseled and familiarized with the use of Visual Analogue scale (VAS) pain score for the assessment of perioperative pain. After obtaining written informed consent, patients were randomly divided into two groups using sealed envelopes technique. A sealed envelope was randomly selected and opened by an assistant, with instructions to draw up the relevant drug. The syringe was labeled with the patient's name and handed to the investigator who performed the block. An independent observer (senior anesthesiologist posted on duty, not included in the study) then observed the onset and offset of sensory and motor blockade and analgesia. Blinding was opened at the end of the study. Group A received 40 ml of solution containing 30 ml 0.5% levobupivacaine and 10 ml 1% lignocaine and group B received 40 ml of solution containing 30 ml 0.25% levobupivacaine with dexmedetomidine 1 μg/kg body weight plus 10 ml 1% lignocaine. Standard anesthetic monitoring was established using electrocardiogram monitor, pulse oximeter, and a noninvasive blood pressure monitor.
All the patients were kept fasting 6-8 hours prior to scheduled procedure. An IV access was achieved on the nonoperative arm prior to performing supraclavicular brachial plexus block. Patients were kept in the supine position with the arm by side of the trunk and extended along the side towards the ipsilateral knee as far as possible, and the head slightly turned to the opposite side. The supraclavicular brachial plexus block was performed using subclavian perivascular technique described by Kulenkampff, modified by Winnie and Collins.[8] The brachial plexus was located using standard peripheral neurostimulator (Stimuplex®, B Braun) with 2-Hz and 1.0-mA. The site that triggered muscular response to a stimulus equal to or lower than 0.4 mA was located, and LA mixture was given in the increments of 5 ml after fixing the stimulating needle, aspirating in between to avoid inadvertent intravascular injection.
Sensory block was assessed by loss of sensation to pin prick over the C5-T1 dermatomes using a three-points scale[9] (0-Sharp pain, 1-Dull pain [analgesia], 2-No pain [anesthesia]). Similarly, motor block was assessed using Bromage Scale[10] (0-Normal motor functions with full flexion and extension of the elbow, wrist and fingers, 1-Decreased motor strength with the ability to move fingers only, 2-Complete motor blockade with inability to move fingers). Sensory and motor blocks were assessed every 2 min for first 10 min and then every 3 min until 30 min after injection, and then every 30 min after surgery, until recovery. Sensory onset time was defined as the time interval between the end of LA administration and establishment of score 2 on three-point scale on all nerve territories. Duration of sensory block was defined as the time interval between the end of LA administration and the complete resolution of anesthesia (score 0 on three-point scale) on all nerves. Complete motor block was defined as the absence of voluntary movement on hand and forearm (score 2 on Bromage Scale). Duration of motor block was defined as the time interval between the end of LA administration and the recovery of complete motor function of the hand and forearm (score 0 on Bromage Scale). Block was considered inadequate when sensory anesthesia was not achieved within 30 min. General anesthesia was given subsequently to these patients who were then excluded from the analysis. Supplemental oxygen was provided to all the patients through nasal canula throughout the surgery.
After taking a preoperative baseline value, vital parameters, that is, systolic blood pressure (SBP), diastolic blood pressure (DBP), arterial saturation (SpO2), respiratory rate (RR), and heart rate (HR) were monitored at every 5 min interval till 30 min of LA injection and then every 10 min till 1st h and thereafter every 15 min till the end of surgery and postoperatively one hourly till first 24 h. Adverse events such as hypotension (20% decrease in relation to the baseline value), bradycardia (HR <60 bpm), hypoxemia (SpO2 90%) and perioperative nausea and vomiting were recorded.
Patient's perception of pain was assessed using VAS (0-10). Rescue analgesics in the form of injection fentanyl 1 μg/kg body weight was given in case patient complained of intraoperative discomfort at any time of surgery (VAS >3). Patients were monitored for 24 h postoperatively to assess total duration of sensory and motor blockade and VAS pain score.
Postoperatively rescue analgesia in the form of nonsteroidal anti-inflammatory drugs (injection diclofenac sodium 75 mg) was given when patient complained of VAS >3. Injection fentanyl 1 μg/kg body weight was administered if patient still complained of pain. The patients were continuously monitored for any perioperative complications and adverse reactions. PSS was recorded after 24 h postoperatively as 5-Excellent, 4-Very Good, 3-Good, 2-Fair, and 1-Poor.
Analysis of data
Statistical methods (n = 43) were chosen after comparing previous studies,[11] taking time for sensory onset in minutes as one of the primary variable to ensure at least 83% power of the study. Sample size was calculated by equating standard error of the sample mean to 20% (i.e., σ/√n = 0.20 => n = σ2/(0.20)2) and power analysis was performed by taking 0.66 min as effect size at 1% level of significance (one-tailed). z = 2.33-d√n/σ. Power = 1-Φ(z) where Φ(z) is the cumulative probability density.
The data from the present study was systematically collected, compiled and statistically analyzed by Statistical Package for Social Sciences version 17.0 (SPSS) software. Unpaired t-test was applied for demographic data, hemodynamic parameters, onset and duration of sensory/motor blockade and duration of analgesia, Chi-square test was applied for age, sex and ASA grades. P value was considered as significant if <0.05 and highly significant if <0.001.
Results
A total of 92 patients were enrolled in this study. One patient in each group failed to achieve block within 30 min. General anesthesia was given subsequently to these patients who were then excluded from the analysis. The demographic data and surgical characteristics were similar in each group and were statistically insignificant (P > 0.05) [Table 1]. Sensory and motor block onset time were significantly shorter in group B as compared to the group A (P < 0.05). Sensory duration was comparable in two groups and was statistically insignificant (P > 0.05). However, the duration of motor blockade was statistically shorter in group B (P < 0.05) and duration of analgesia was statistically longer in group B (P < 0.05) when compared to group A [Table 2]. Intraoperative fentanyl was required in two patients in group A, while no patient in group B required fentanyl [Table 1]. VAS pain scores were less in group B at each interval [Figure 1].
Table 1.
The demographic data and surgical characteristics
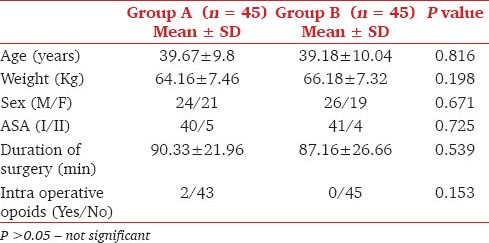
Table 2.
The characteristics of block

Figure 1.
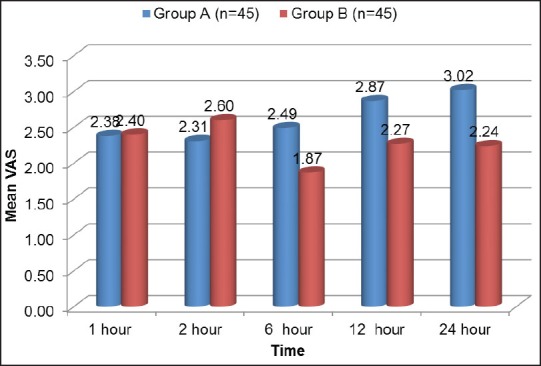
Visual analog score
We observed a statistically significant difference (P < 0.05) in HR between two groups from 10 min after the block, which extended in the postoperative period up to 24 h [Figure 2]. A statistically significant difference was observed in SBP and DBP from 10 min that extended into the postoperative period [Figure 3]. Bradycardia (HR <60) was observed in two patients in group B but none of them required treatment. Both the groups were comparable for RR and SpO2 at each interval, and the results were statistically insignificant. None of the patients in either group had technique or drug-related side effects or complications. Postoperative analgesic requirement has been depicted in Table 3. Patients in both the groups had an equally good satisfaction score [Table 4].
Figure 2.
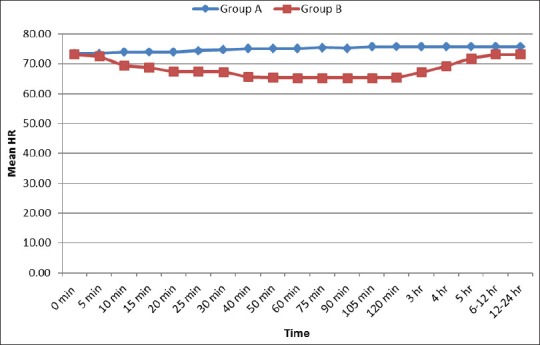
Heart rate in group A and group B
Figure 3.
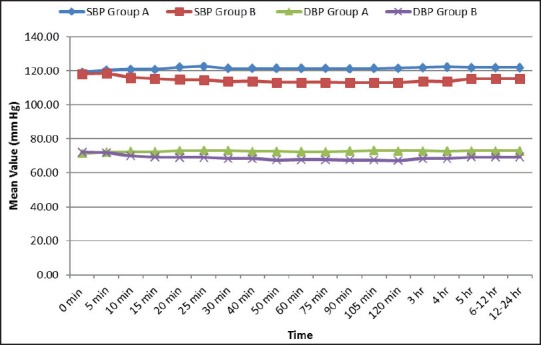
Systolic and diastolic blood pressure in group A and group B
Table 3.
Post operative analgesic requirement
Table 4.
Patient satisfaction score

Discussion
In this study, we demonstrated that the addition of dexmedetomidine to levobupivacaine can significantly: decrease the concentration of levobupivacaine required for surgical anesthesia; shortens the sensory and motor block onset time; reduce the offset time for motor block; prolong the duration of postoperative analgesia; reduce the total LA dose without any perioperative analgesic compromise; provides significantly lower postoperative VAS pain scores, and provided comparable overall satisfaction scores among patients.
Local anesthetic agent selection, dose, concentration, volume, and physical modifications can affect onset, spread, quality, and duration of anesthesia. Levobupivacaine, the S-enantiomer of bupivacaine, which has less cardiac and neural toxicity than bupivacaine, is currently the closest to the ideal agent for neural blockade however large volumes of drug are required for adequate block. It has been observed that 0.25% levobupivacaine and 0.25% bupivacaine have a similar motor and sensory block onset times and qualities, and provide comfortable anesthesia and analgesia for shoulder surgery.[12] A volume of 10 ml of 1% lignocaine was added to both the groups so as to hasten the onset of block. Further studies can be conducted to evaluate whether the addition of dexmedetomidine can further reduce the concentration of lignocaine also without compromising motor block. As dexmedetomidine has peripheral analgesic action,[13] so it was hypothesized that it may be helpful in reducing the total concentration of levobupivacaine from 0.5% to 0.25%, which has been validated by the findings of our study. Lesser concentration of LA correlates well with lesser duration of motor block as seen in patients allowing early painless movement of the limb and hence better postoperative comfort as well as better safety due to reduced amount of LA injected.
Alpha-2-adrenergic receptor (α2-AR) agonists have been successfully utilized in various anesthetic techniques due to the hemodynamic-stabilizing properties, sedative, analgesic, and sympatholytic effects.[14] In addition, α2-AR agonist such as dexmedetomidine have demonstrated a dose-dependent increase in the duration of thermal antinociception and analgesia in many animal studies.[15,16] Dexmedetomidine in clinically effective doses lacks respiratory depression,[17,18] but maintains its analgesic properties that may make it useful and safe adjunct in many diverse clinical applications.
No animal study has shown any evidence of neurotoxicity when administering dexmedetomidine (even at high concentrations) directly to sciatic nerves.[19] Peripheral analgesic effects of dexmedetomidine have enabled an overall improved blockade quality when added to LAs in a peripheral nerve block model and are thought to be mediated by α2-AR binding.[13]
Dexmedetomidine mixed with lidocaine has been reported to decrease tourniquet pain, improve block quality, and prolong postoperative analgesia during intravenous regional anesthesia.[20]
In a randomized, double-blind trial performed by Esmaoglu et al.,[11] dexmedetomidine added to levobupivacaine for axillary brachial plexus blockade shortened the block onset time, prolonged the duration of motor and sensory effects, and extended postoperative analgesia. However, they used 0.5% levobupivacaine with dexmedetomidine 100 μg but in this study we used dexmedetomidine 1 μg/kg with 0.25% levobupivacaine and compared it with 0.5% levobupivacaine. Mean weight of the patients was 64.16 ± 7.4 in group A and 66.18 ± 7.3 in group B. Reduced concentrations of levobupivacaine could be the reason for less duration of motor block seen in group B and reduced amount dexmedetomidine in μg/kg body weight could be the reason of less incidence of bradycardia in our study.
Recently Kaygusuz et al.[21] evaluated the addition of dexmedetomidine 1 μg/kg to 0.5% levobupivacaine in axillary brachial plexus block and observed significantly decreased sensory block onset time, an increase in the sensory and motor block duration and time to first-analgesic use, and decreased total analgesic use with no side effects. In our study by using dexmedetomidine 1 μg/kg with 0.25% levobupivacaine we could reduce the concentration of levobupivacaine and achieve early motor recovery resulting in better patient comfort and satisfaction without any perioperative analgesic compromise.
Swami et al.[22] used dexmedetomidine and clonidine as an adjuvant to bupivacaine 0.25% in supraclavicular plexus block and demonstrated that dexmedetomidine prolongs the duration of sensory and motor block and enhances the quality of block as compared with clonidine.
Ammar et al.[23] used dexmedetomidine with bupivacaine and compared it with plain bupivacaine and demonstrated enhancement of onset of sensory and motor blockade, prolonged duration of analgesia, increased duration of sensory and motor block, lower VAS pain scores, and reduction in supplemental opioid requirements.
Dexmedetomidine may lead to side effects such as hypotension and bradycardia with increased dosage, along with its effects such as sedation and anxiolysis.[24] In our study, two patients developed bradycardia, which did not require any treatment.
Major limitations of our study were that we could not biochemically analyze the blood concentration of levobupivacaine and dexmedetomidine due to nonavailability of facilities at our institution, which would have further supported our conclusions. Use of ultrasound guided nerve blocks may further help to reduce effective levobupivacaine concentration with advantage of injecting the LA mixtures in near proximity of nerve bundles. Further randomized trials need to be conducted to validate the findings of our study.
Conclusion
The results of the present study conclude that the addition of 1 microg/kg dexmedetomidine to 0.25% levobupivacaine for supraclaviclar plexus block helps in decreased onset time for sensory and motor block. It results in better patient comfort and comparable satisfaction due to early motor recovery, with lower VAS pain scores. Reduction in total levobupivacaine dose also increases the safety margin of the block.
Acknowledgments
The authors like to thanks Mr Ghansham Sharma for helping us in statistical analysis.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Robaux S, Blunt C, Viel E, Cuvillon P, Nouguier P, Dautel G, et al. Tramadol added to 1.5% mepivacaine for axillary brachial plexus block improves postoperative analgesia dose-dependently. Anesth Analg. 2004;98:1172–7. doi: 10.1213/01.ANE.0000108966.84797.72. [DOI] [PubMed] [Google Scholar]
- 2.Antonucci S. Adiuvants in the axillary brachial plexus blockade. Comparison between clonidine, sufentanil and tramadol. Minerva Anestesiol. 2001;67:23–7. [PubMed] [Google Scholar]
- 3.Geze S, Ulusoy H, Ertürk E, Cekic B, Arduc C. Comparison of local anesthetic mixtures with tramadol or fentanyl for axillary plexus block in orthopaedic upper extremity surgery. Eur J Gen Med. 2012;9:118–23. [Google Scholar]
- 4.Foster RH, Markham A. Levobupivacaine: A review of its pharmacology and use as a local anaesthetic. Drugs. 2000;59:551–79. doi: 10.2165/00003495-200059030-00013. [DOI] [PubMed] [Google Scholar]
- 5.Mazoit JX, Boïco O, Samii K. Myocardial uptake of bupivacaine: II. Pharmacokinetics and pharmacodynamics of bupivacaine enantiomers in the isolated perfused rabbit heart. Anesth Analg. 1993;77:477–82. [PubMed] [Google Scholar]
- 6.Kanazi GE, Aouad MT, Jabbour-Khoury SI, Al Jazzar MD, Alameddine MM, Al-Yaman R, et al. Effect of low-dose dexmedetomidine or clonidine on the characteristics of bupivacaine spinal block. Acta Anaesthesiol Scand. 2006;50:222–7. doi: 10.1111/j.1399-6576.2006.00919.x. [DOI] [PubMed] [Google Scholar]
- 7.Congedo E, Sgreccia M, De Cosmo G. New drugs for epidural analgesia. Curr Drug Targets. 2009;10:696–706. doi: 10.2174/138945009788982441. [DOI] [PubMed] [Google Scholar]
- 8.Winnie AP, Collins VJ. The subclavian perivascular technique of brachial plexus anesthesia. Anesthesiology. 1964;25:353–63. doi: 10.1097/00000542-196405000-00014. [DOI] [PubMed] [Google Scholar]
- 9.Crews JC, Weller RS, Moss J, James RL. Levobupivacaine for axillary brachial plexus block: A pharmacokinetic and clinical comparison in patients with normal renal function or renal disease. Anesth Analg. 2002;95:219–23. doi: 10.1097/00000539-200207000-00039. [DOI] [PubMed] [Google Scholar]
- 10.Sarkar DJ, Khurana G, Chaudhary A, Sharma JP. A comparative study on the effects of adding fentanyl and buprenorphine to local anaesthetics in brachial plexus block. J Clin Diagn Res. 2010;4:3337–43. [Google Scholar]
- 11.Esmaoglu A, Yegenoglu F, Akin A, Turk CY. Dexmedetomidine added to levobupivacaine prolongs axillary brachial plexus block. Anesth Analg. 2010;111:1548–51. doi: 10.1213/ANE.0b013e3181fa3095. [DOI] [PubMed] [Google Scholar]
- 12.Baskan S, Taspinar V, Ozdogan L, Gulsoy KY, Erk G, Dikmen B, et al. Comparison of 0.25% levobupivacaine and 0.25% bupivacaine for posterior approach interscalene brachial plexus block. J Anesth. 2010;24:38–42. doi: 10.1007/s00540-009-0846-0. [DOI] [PubMed] [Google Scholar]
- 13.Yoshitomi T, Kohjitani A, Maeda S, Higuchi H, Shimada M, Miyawaki T. Dexmedetomidine enhances the local anesthetic action of lidocaine via an alpha-2A adrenoceptor. Anesth Analg. 2008;107:96–101. doi: 10.1213/ane.0b013e318176be73. [DOI] [PubMed] [Google Scholar]
- 14.Khan ZP, Ferguson CN, Jones RM. alpha-2 and imidazoline receptor agonists. Their pharmacology and therapeutic role. Anaesthesia. 1999;54:146–65. doi: 10.1046/j.1365-2044.1999.00659.x. [DOI] [PubMed] [Google Scholar]
- 15.Brummett CM, Padda AK, Amodeo FS, Welch KB, Lydic R. Perineural dexmedetomidine added to ropivacaine causes a dose-dependent increase in the duration of thermal antinociception in sciatic nerve block in rat. Anesthesiology. 2009;111:1111–9. doi: 10.1097/ALN.0b013e3181bbcc26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Brummett CM, Amodeo FS, Janda AM, Padda AK, Lydic R. Perineural dexmedetomidine provides an increased duration of analgesia to a thermal stimulus when compared with a systemic control in a rat sciatic nerve block. Reg Anesth Pain Med. 2010;35:427–31. doi: 10.1097/AAP.0b013e3181ef4cf0. [DOI] [PubMed] [Google Scholar]
- 17.Belleville JP, Ward DS, Bloor BC, Maze M. Effects of intravenous dexmedetomidine in humans. I. Sedation, ventilation, and metabolic rate. Anesthesiology. 1992;77:1125–33. doi: 10.1097/00000542-199212000-00013. [DOI] [PubMed] [Google Scholar]
- 18.Hall JE, Uhrich TD, Barney JA, Arain SR, Ebert TJ. Sedative, amnestic, and analgesic properties of small-dose dexmedetomidine infusions. Anesth Analg. 2000;90:699–705. doi: 10.1097/00000539-200003000-00035. [DOI] [PubMed] [Google Scholar]
- 19.Brummett CM, Norat MA, Palmisano JM, Lydic R. Perineural administration of dexmedetomidine in combination with bupivacaine enhances sensory and motor blockade in sciatic nerve block without inducing neurotoxicity in rat. Anesthesiology. 2008;109:502–11. doi: 10.1097/ALN.0b013e318182c26b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ramadhyani U, Park JL, Carollo DS, Waterman RS, Nossaman BD. Dexmedetomidine: Clinical application as an adjunct for intravenous regional anesthesia. Anesthesiol Clin. 2010;28:709–22. doi: 10.1016/j.anclin.2010.08.008. [DOI] [PubMed] [Google Scholar]
- 21.Kaygusuz K, Kol IO, Duger C, Gursoy S, Ozturk H, Kayacan U, et al. Effects of adding dexmedetomidine to levobupivacaine in axillary brachial plexus block. Curr Ther Res Clin Exp. 2012;73:103–11. doi: 10.1016/j.curtheres.2012.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Swami SS, Keniya VM, Ladi SD, Rao R. Comparison of dexmedetomidine and clonidine (a2 agonist drugs) as an adjuvant to local anaesthesia in supraclavicular brachial plexus block: A randomised double-blind prospective study. Indian J Anaesth. 2012;56:243–9. doi: 10.4103/0019-5049.98767. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Ammar AS, Mahmoud KM. Ultrasound-guided single injection infraclavicular brachial plexus block using bupivacaine alone or combined with dexmedetomidine for pain control in upper limb surgery: A prospective randomized controlled trial. Saudi J Anaesth. 2012;6:109–14. doi: 10.4103/1658-354X.97021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Talke P, Lobo E, Brown R. Systemically administered alpha2-agonist-induced peripheral vasoconstriction in humans. Anesthesiology. 2003;99:65–70. doi: 10.1097/00000542-200307000-00014. [DOI] [PubMed] [Google Scholar]