

Abstract
Objectives.
Although there is extensive research on the stress-buffering effects of social support on health, there is little understanding of this effect on health behaviors such as smoking, particularly during old age. This study aimed to estimate the effect of financial strain and the stress-buffering effect of social support, on the trajectory of smoking over an extended period of time among older Japanese.
Method.
Data came from a national sample of more than 4,800 adults, aged 60 and older in Japan, with up to 7 repeated observations between 1987 and 2006 (16,669 observations). Hierarchical linear modeling was used to analyze the intrapersonal and interpersonal differences in smoking.
Results.
Higher financial strain at baseline was associated with greater amount of smoking, and a slower rate of decline, after adjusting for sociodemographic attributes. Greater instrumental support partially offset the deleterious effect of financial strain on the rate of decline in smoking.
Discussion.
Our findings add a dynamic dimension to understanding the relationship among financial strain, social support, and smoking in old age. This knowledge is significant when designing health policies and interventions regarding health behaviors in late life.
Key Words: Financial strain, Hierarchical linear modeling, Japan, Social support, Stress-buffering effect, Trajectory of smoking.
The estimated number of deaths attributable to smoking in Japan in 2005 was 163,000 for men and 33,000 for women, and the population attributable fraction of mortality associated with smoking was 27.8% for men and 6.7% for women (Katanoda et al., 2008). Moreover, the social costs of smoking (e.g., health care costs, costs for fire loss and fire fighting, and loss of labor) were estimated to be more than 4.3 trillion JPY (about 48 billion USD) in 2009 (Institute for Health Economics and Policy, 2010).
Although the rate of smoking among men in Japan has been declining in recent years, it remains relatively high (32.2% in 2010). In contrast, the rate of smoking among women is relatively low (8.4% in 2010), but it has been rising slightly in the past decade or more (Ministry of Health, Labour and Welfare, 2011). Among older adults, the rate of smoking has decreased by year but still remains high, especially in men (27.4% in men aged 60–69 and 15.6% in men aged 70 and older; 4.5% in women aged 60–69 and 2.0% in women aged 70 and older in 2010; Ministry of Health, Labour and Welfare, 2011), compared with that of American men aged 65 and older (9.7% in 2010; Centers for Disease Control and Prevention, 2011). Several studies have demonstrated the influence of smoking on adverse health outcomes such as mortality (Fujisawa et al., 2008; Liang, Bennett, Sugisawa, Kobayashi, & Fukaya, 2003), cardiovascular events and diabetes mellitus (Muratani et al., 2000), and functional decline (Tsubota-Utsugi et al., 2011) among the Japanese elderly adults. Moreover, research has found that life expectancy at age of 40 years is reduced by slightly less than 4 years in smokers compared with never smokers in both Japanese men and women and that smoking cessation at any age leads to a certain recovery of life expectancy (Ozasa et al., 2008). In a rapidly aging nation like Japan, the burden of smoking, including its economic costs at old age, will continue to grow. Therefore, tackling smoking problems in the older population must be a significant public health priority.
One barrier to reducing smoking among older Japanese is that many people are likely to use smoking as a way to cope with psychological strain. When discussing the association between psychological strain and smoking, the tension reduction hypothesis has been the predominant underlying theoretical rationale (Abbey, Smith, & Scott, 1993; Greeley & Oei, 1999). According to this hypothesis, people are inclined to increase the use of substances (e.g., tobacco and alcohol) as a means of relieving the negative emotions resulting from stress exposure. Although the associations between socioeconomic position indicators (education, occupation, and income) and smoking are well established (Businelle et al., 2010; Hiscock, Bauld, Amos, Fidler, & Munafò, 2012; van Loon, Tijhuis, Surtees, & Ormel, 2005), little attention has been paid to how psychological strain within the context of social stratification may affect smoking (Siahpush, Yong, Borland, Reid, & Hammond, 2009). Previous studies regarding the relationship between financial strain and smoking status have supported the general tenets of the tension reduction hypothesis (Falba, Teng, Sindelar, & Gallo, 2005; Kendzor et al., 2010; Nelson, Lust, Story, & Ehlinger, 2008; Shaw, Agahi, & Krause, 2011; Siahpush & Carlin, 2006; Siahpush et al., 2009). For example, studies using longitudinal data between two points demonstrated that adult smokers with more financial strain were less likely to quit smoking (Kendzor et al., 2010; Siahpush et al., 2009). College students with credit card debt tended to smoke in the past month (Nelson et al., 2008). Further, among older adults in the United States, it was revealed by multilevel models with longitudinal data that increases in levels of financial strain were directly associated with the odds of smoking over time (Shaw et al., 2011).
One factor that has been considered as a moderator of the relationship between stressor and smoking is social support. The potential moderating effects of social support are known as “stress-buffering effects,” indicating that social support could protect an individual from the potentially harmful effects of stressors (Cohen & McKay, 1984). Among older people, some research has revealed this stress-buffering effect of social support on health status. For example, older people who had more informational and emotional support and who provided support to others more often reported fewer symptoms of depression as a result of financial strain compared with those who had and provided less support (Krause, 1987). Conversely, the undesirable effects of personal financial strain on changes in self-rated health were more pronounced at progressively higher levels of negative social interaction among older adults (Krause, Newsom, & Rook, 2008).
In addition to the direct effect of social support on smoking through improving social influence, social engagement, and access to material resources (Berkman & Glass, 2000), social support may buffer the relationship between stress and smoking by affecting individual coping resources, including accessing new contacts and information and defining and solving problems (Heaney & Israel, 2008). This in turn increases the likelihood that stressors will be handled with adaptive coping (e.g., relaxation), which minimizes the negative impact of a stressor (Westmaas, Bontemps-Jones, & Bauer, 2010). Moreover, social support can help to reduce uncertainty and unpredictability, leading to a greater sense of personal control over specific situations and life domains (Heaney & Israel, 2008). According to Bandura’s (1997) work on self-efficacy, a strong sense of personal control leads to strong feelings of self-efficacy with regard to specific behaviors, which, in turn, are direct precursors of behavior modification and maintenance. Some articles have reported this stress-buffering effect of social support on smoking, particularly in workplace settings (Sapp, Kawachi, Sorensen, LaMontagne, & Subramanian, 2010), among lower educated women (Turner, Mermelstein, Hitsman, & Warnecke, 2008) and among African American women (Budescu, Taylor, & McGill, 2011). However, we still know little about the potential stress-buffering effects of social support on smoking in old age.
Taken together, although there is extensive research on the effects of financial strain on smoking and the stress-buffering effect of social support, there are several important gaps that remain to be addressed. First, most previous studies on these topics have focused on young and middle-aged populations, including college students and employees, rather than the older population. Smoking behavior and its relationship with financial strain and social support among young people or current workers may differ from those among older adults, as individual social and economic circumstances, as well as health status, change substantially across the life course. Second, almost all studies in this area have assessed smoking behavior using cross-sectional data or, at most, longitudinal data between two points in time. Understanding the trajectory of smoking, involving the level of tobacco use and its rate of change over time, and its risk factors might contribute to the development and improvement of interventions to reduce tobacco use in late life. Analyzing multiwave longitudinal data of a national sample of older Americans for 10 years, Shaw and coworkers (2011) focused on the linkage between within-person changes in financial strain and within-person changes in smoking, that is, whether time-varying financial strain was associated with smoking. However, they did not consider the between-person association of financial strain with the levels of tobacco use and its rate of change over time. Third, most of the studies on smoking among older people are from Western countries. Considering the difference in backgrounds between Japan and Western countries, it is important to explore the relationships of financial strain and social support with smoking in Japan. Data from non-Western societies present many conditions not observable in Western countries and could offer useful insights concerning the underlying mechanisms.
In this study, to address these gaps, we analyzed data from a national sample of older Japanese, followed for 19 years. The purpose of this study was to estimate the effects of financial strain on the trajectories of smoking and to examine how social support buffers the effects of financial strain on the trajectories of smoking over an extended period of time among older Japanese.
As mentioned earlier, several previous studies supported the tension reduction hypothesis by examining the linkage between financial strain and smoking status, though most of these were not studies of older generations (Falba et al., 2005; Kendzor et al., 2010; Nelson et al., 2008; Shaw et al., 2011; Siahpush & Carlin, 2006; Siahpush et al., 2009). Going beyond these conventional observations, in order to add a dynamic dimension to understanding how financial strain influences smoking in old age, we hypothesize that older people who feel more financial strain smoke more and have a slower rate of decline in smoking over time compared with older people who feel less financial strain (H1). The second hypothesis is that social support buffers the effects of financial strain on levels of smoking and its rate of changes over time (H2).
Method
Sample and Procedures
Data came from the National Survey of the Japanese Elderly (NSJE), a seven-wave (1987, 1990, 1993, 1996, 1999, 2002, and 2006) longitudinal data set based on a sample of 4,869 Japanese, 60 years of age and older, with 16,669 observations over a period of 19 years (1987–2006). NSJE began with 2,200 people aged 60 and older in 1987. The sample was subsequently supplemented in 1990 (N = 580) and 1996 (N = 1,210). An additional sample of those aged 70 and older (N = 2,000) was added in 1999. In NSJE, face-to-face interviews were used to collect data. Trained investigators visited the respondents’ homes, and the interviews were performed with a structured questionnaire. Response rates for the seven waves of surveys ranged from 69% to 93%. Responses obtained from proxy interviews were excluded. This study was approved by the Institutional Review Board of the Tokyo Metropolitan Institute of Gerontology.
Measures
Smoking.—
We asked current smoking status to all respondents with the statement of “Do you smoke currently?” The respondents were dichotomized: smoking (1) and nonsmoking (0). For the respondents who reported current smoking, an additional question about the amount of cigarettes was asked with the statement of “How many cigarettes do you smoke daily on average?” In the analysis, we used this average number of cigarettes smoked per day by each respondent as the dependent variable. Responses of nonsmoking in the first question were coded as “zero cigarettes per day.”
Financial strain.—
Financial strain was measured by a three-item composite, including (a) satisfaction with finances (completely satisfied [1], very satisfied [2], cannot say either way [3], not very satisfied [4], and not at all satisfied [5]); (b) financial situation compared with others (better [1], about the same [2], and worse [3], which was transformed into a 5-point scale); and (c) whether they have enough pocket money (yes [1] and no [2], which was also transformed into a 5-point scale). Scores for financial strain had a possible range from 5 to 15 (Cronbach’s alpha = .67), with higher scores reflecting more strain.
Social support.—
We measured two types of received social support: Emotional support and instrumental support. Emotional and instrumental supports were each measured by a two-item composite. Emotional support received consisted of “How often someone listens to you” and “How often someone shows you love and understanding.” Instrumental support comprised “How often someone cares for you when you are sick” and “How often someone provides financial assistance.” All items described earlier were coded from never (1) to always (5). The emotional and instrumental support composites ranged from 2 to 10 (Cronbach’s alpha = .87 for emotional support and .61 for instrumental support), with a higher score reflecting greater support received.
Covariates
Baseline measures of age, gender, marital status, socioeconomic status (SES), and health status were also incorporated in this study. Marital status (not married [0] and married [1]) was indexed as a binary indicator. SES measures included education, which was indexed by the number of years of schooling, and household annual income, which was assessed by using five categories, ranging from less than 1.2 million yen per year (1) to more than 10 million yen per year (5).
Regarding health status, multiple measures were included. First, disease burden was measured as a count of 16 health conditions (i.e., cancer, high blood pressure, heart conditions, diabetes, stroke, arthritis, eye disease, lung disease, chronic back pain, liver disease, trouble with circulation, stomach disease, kidney disease, anemia, Parkinson’s, skin disease). Scores on the total conditions composite ranged from 0 to 16. Second, self-rated health was measured by a three-item composite including a rating of overall present health, satisfaction with one’s health, and comparison of one’s health with others of the same age. Scores on the self-rated health composite ranged from 3 to 15 (Cronbach’s alpha = .85), with a higher score indicating poorer health. Finally, functional status entailed a sum of difficulties with six activities of daily living (i.e., dressing, walking, bathing or showering, eating, getting in or out of bed, and using the toilet) and five instrumental activities of daily living (i.e., grocery shopping, phone calls, climbing stairs, walking a few blocks, and traveling by bus or train). All items except climbing stairs and walking a few blocks described earlier were coded from no difficulty (1) to unable to do (5). Climbing stairs and walking a few blocks were coded on a 5-point scale in Waves 1 and 2 but coded on a 4-point scale in Waves 3 through 7. Therefore, a 4-point scale in Waves 3 through 7 was transformed into a 5-point scale. Scores for this composite ranged from 11.5 to 55 (Cronbach’s alpha = .92), with a higher score reflecting more difficulty.
Data Analysis
Hierarchical linear models (HLMs) were used to chart the trajectory of smoking as a function of financial strain. With a mean of 4.14 cigarettes a day at the baseline, the count for the dependent variable, number of cigarettes smoked per day, was positively skewed (skewness = 2.209; kurtosis = 4.927) and contained many zeros partially due to the substantial proportion of individuals who did not smoke. Statistically, it might be better to treat number of cigarettes smoked per day with several categories (including nonsmoking, moderate smoking [1–19 cigarettes per day], and heavy smoking [20+ cigarettes per day]). We undertook our analyses both with a multilevel linear regression model, which treated the number of cigarettes as a continuous variable, and with a multinomial logistic regression model, which treated smoking as categorical variable (with nonsmoking as the reference category), and obtained similar results. For the ease of presentation, we focus on the results from the analyses that treated smoking as a continuous variable.
The intraindividual differences in the average number of cigarettes smoked per day were modeled as follows in the Level 1 equation:
| (1) |
where Y iT is the number of cigarettes smoked by individual i at time T. π0i is the intercept (i.e., level) and π1i is the slope (i.e., rate of change) over time. Time is the distance (in years) of assessment from the baseline when the respondent was first interviewed, and εiT is a random error. Time was centered on its grand mean (5.43 years).
Interpersonal variations in the trajectory of smoking (i.e., intercept and slope) were specified in the Level 2 equation:
| (2) |
where X qi is the qth covariate (e.g., financial strain, age at baseline, gender, and education) associated with individual i, and βpq represents the effect of variable X q on the pth growth parameter (πp; i.e., intercept and slope). r pi is a random effect with a mean of 0. All covariates (Level 2) were centered on their grand mean. All models were fitted by using HLM version 6.08
To minimize the loss of participants due to item nonresponse, multiple imputation was undertaken. In particular, three complete data sets were imputed with the NORM software developed by Schafer (1997), and analyses were run on each of these three data sets with parameter estimates derived by averaging across three imputations and by adjusting for their variance. As a major advantage, multilevel models can include every participant in the estimation, regardless of how many observations one contributed to the data set. With reference to attrition, multilevel models are predicated on the assumption of missing at random (MAR), which means that the probability of missing depends upon only the observed data for either the covariates or the outcome variables, hence permitting valid inference (Raudenbush & Bryk, 2002). In addition to MAR, to adjust for the selection bias, we included binary variables in the Level 2 equation to indicate attrition due to nonresponse and attrition due to death. These variables were viewed as confounding variables instead of predictors of daily amount of smoking.
The modeling was performed in four models. At first, age, gender, marital status, SES, financial strain, and social support at baseline were included in the model (Model 1). Next, to assess the interaction between financial strain and social support on amount of smoking, we added these interactions to Model 1 (Model 2). In Model 3, health status at baseline was added to Model 2. Finally, in Model 4, attrition due to nonresponse and death was added to Model 3.
Results
Table 1 presents the descriptive statistics of the respondents (N = 4,869) at the baseline. Mean age was 69.85 (SD = 7.20), and 55.31% of respondents were women. Mean educational years was 9.15 (SD = 2.76), and the mode of household annual income was 3–5 million yen.
Table 1.
Baseline Descriptive Statistics (N = 4,869)
| M | SD | % | |
|---|---|---|---|
| Age (years) | 69.85 | 7.20 | |
| Female | 55.31 | ||
| Education (years) | 9.15 | 2.76 | |
| Household income | 2.88 | 1.10 | |
| Less than 1.2 million yen | 10.45 | ||
| 1.2–3 million yen | 29.14 | ||
| 3–5 million yen | 30.58 | ||
| 5–10 million yen | 22.30 | ||
| More than 10 million yen | 7.52 | ||
| Total conditions (range: 0–16) | 1.23 | 1.37 | |
| Self-rated poor health (range: 3–15) | 7.69 | 2.81 | |
| Functional status (range: 11.5–55) | 17.26 | 5.38 | |
| Average number of cigarettes smoked per day | 4.14 | 8.43 | |
| 0 cigarettes per day | 75.46 | ||
| 1–19 cigarettes per day | 12.43 | ||
| 20+ cigarettes per day | 12.12 | ||
| Financial strain (range: 5–15) | 8.39 | 2.22 | |
| Emotional support received (range: 2–10) | 8.26 | 1.66 | |
| Instrumental support received (range: 2–10) | 7.93 | 1.49 | |
| Dead | 36.74 | ||
| Attrition | 20.99 |
Table 2 shows the results of the multilevel linear regression model. To depict the trajectory of smoking, we evaluated linear, quadratic, and cubic models and chose the most appropriate one on the basis of the statistical significance of higher order fixed effects estimates. As quadric and cubic models were not statistically significant, the change in smoking can be best described by a linear function. In Model 1, the intercept of the linear slope was significant (b = −0.185, p < .001), meaning that the number of cigarettes smoked per day declined within individuals over time. After adjusting for sociodemographic attributes, baseline financial strain was associated with higher levels of smoking (b = 0.123, p = .006) and with relatively slow declines in smoking over time (b = 0.009, p = .031). These findings lend support to the first hypothesis (H1). Regarding social support, instrumental support at baseline was associated with lower levels of smoking (b = −0.134, p = .041). The rate of decline in smoking was slower among people with greater emotional support at baseline (b = 0.016, p = .007).
Table 2.
Hierarchical Linear Model for Average Number of Cigarettes Smoked per Day
| Model 1 | Model 2 | Model 3 | Model 4 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| b | SE | p | b | SE | p | b | SE | p | b | SE | p | |
| Fixed effecta | ||||||||||||
| Intercept (π0) | ||||||||||||
| Intercept | 3.159 | 0.089 | .000 | 3.151 | 0.090 | .000 | 3.138 | 0.090 | .000 | 3.169 | 0.091 | .000 |
| Age | −0.130 | 0.013 | .000 | −0.131 | 0.013 | .000 | −0.124 | 0.013 | .000 | −0.142 | 0.013 | .000 |
| Female | −5.469 | 0.182 | .000 | −5.468 | 0.196 | .000 | −5.402 | 0.195 | .000 | −5.194 | 0.196 | .000 |
| Education | −0.148 | 0.034 | .000 | −0.148 | 0.038 | .000 | −0.148 | 0.038 | .000 | −0.129 | 0.038 | .001 |
| Household income | −0.255 | 0.090 | .005 | −0.253 | 0.086 | .004 | −0.272 | 0.086 | .002 | −0.230 | 0.087 | .008 |
| Financial strain | 0.123 | 0.044 | .006 | 0.117 | 0.046 | .010 | 0.157 | 0.046 | .001 | 0.170 | 0.046 | .000 |
| Emotional support | 0.038 | 0.058 | .516 | 0.037 | 0.060 | .538 | 0.026 | 0.060 | .660 | −0.013 | 0.060 | .828 |
| Instrumental support | −0.134 | 0.066 | .041 | −0.129 | 0.066 | .049 | −0.142 | 0.066 | .030 | −0.105 | 0.066 | .110 |
| Emotional support × Financial strain | 0.010 | 0.026 | .696 | 0.008 | 0.026 | .750 | 0.012 | 0.026 | .643 | |||
| Instrumental support × Financial strain | −0.020 | 0.028 | .459 | −0.019 | 0.028 | .499 | −0.021 | 0.028 | .455 | |||
| Total condition | −0.141 | 0.064 | .029 | −0.118 | 0.064 | .065 | ||||||
| Self-rated health | -0.109 | 0.037 | .003 | -0.127 | 0.037 | .001 | ||||||
| Functional status | 0.008 | 0.028 | .776 | −0.005 | 0.027 | .855 | ||||||
| Dead | 1.272 | 0.223 | .000 | |||||||||
| Attrition | 0.304 | 0.217 | .162 | |||||||||
| Linear slope (π1) | ||||||||||||
| Intercept | −0.185 | 0.010 | .000 | −0.188 | 0.010 | .000 | −0.190 | 0.010 | .000 | −0.185 | 0.010 | .000 |
| Age | 0.004 | 0.001 | .004 | 0.004 | 0.001 | .002 | 0.005 | 0.001 | .001 | 0.005 | 0.001 | .002 |
| Female | 0.309 | 0.018 | .000 | 0.309 | 0.020 | .000 | 0.307 | 0.020 | .000 | 0.302 | 0.020 | .000 |
| Education | 0.000 | 0.003 | .896 | 0.000 | 0.004 | .935 | 0.001 | 0.004 | .868 | 0.000 | 0.004 | .932 |
| Household income | 0.001 | 0.009 | .912 | 0.001 | 0.009 | .873 | 0.002 | 0.009 | .802 | 0.001 | 0.009 | .882 |
| Financial strain | 0.009 | 0.004 | .031 | 0.007 | 0.004 | .083 | 0.006 | 0.004 | .189 | 0.005 | 0.004 | .201 |
| Emotional support | 0.016 | 0.006 | .007 | 0.016 | 0.006 | .012 | 0.017 | 0.006 | .007 | 0.017 | 0.006 | .006 |
| Instrumental support | −0.008 | 0.006 | .223 | −0.006 | 0.007 | .392 | −0.005 | 0.007 | .414 | −0.006 | 0.007 | .359 |
| Emotional support × Financial strain | 0.003 | 0.003 | .203 | 0.003 | 0.003 | .203 | 0.003 | 0.003 | .211 | |||
| Instrumental support × Financial strain | −0.007 | 0.003 | .011 | −0.007 | 0.003 | .011 | −0.007 | 0.003 | .010 | |||
| Total condition | −0.012 | 0.007 | .099 | −0.012 | 0.007 | .101 | ||||||
| Self-rated health | 0.009 | 0.004 | .017 | 0.009 | 0.004 | .013 | ||||||
| Functional status | −0.003 | 0.004 | .395 | −0.003 | 0.004 | .411 | ||||||
| Dead | −0.009 | 0.025 | .704 | |||||||||
| Attrition | 0.009 | 0.023 | .704 | |||||||||
| Random effect (variance) | ||||||||||||
| Intercept | 32.224 | .000 | 32.232 | .000 | 32.108 | .000 | 31.825 | .000 | ||||
| Linear slope | 0.137 | .000 | 0.137 | .000 | 0.137 | .000 | 0.137 | .000 | ||||
| Level 1 εb | 10.808 | 10.804 | 10.801 | 10.808 | ||||||||
Notes. aAll variables in the analysis were measured at baseline (time-constant variables).
bLevel 1 ε is the random effect in the level 1 equation.
In Model 2, the interactions between the two types of social support and financial strain were added. We found a significant interaction between instrumental support and financial strain at baseline on the rate of change in smoking (b = −0.007, p = .011). This indicates that greater instrumental support partially offsets the deleterious effect of financial strain on the rate of decline in smoking (Figure 1), supporting our second hypothesis (H2).
Figure 1.
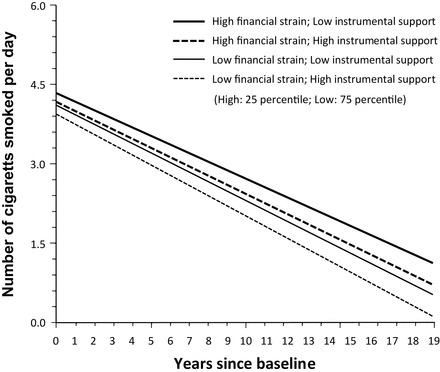
Linear trajectory of average number of cigarettes smoked per day by financial strain and instrumental support (Based on Model 2 in Table 2).
Finally, even with the baseline health status (total conditions, self-rated health, and functional status) and mortality and attrition controlled (Model 3 and 4, respectively), the observed associations, including the interaction between instrumental support and financial strain, remained robust.
Discussion
The findings from this study provide two new insights. First, among older Japanese, experiences of financial strain were associated with elevated levels of smoking. Second, greater instrumental support partially offset the deleterious effect of financial strain on smoking, suggesting a stress-buffering role of instrumental support. Population aging is a worldwide phenomenon and is a particularly pressing matter in Japan. Although rates of smoking among older people are lower than those among younger age groups, smoking rates among older Japanese men remain high (Ministry of Health, Labour and Welfare, 2011). Thus, understanding the major influences on smoking in later life can provide important clues to develop health promotion strategies in an aging society like Japan and also in other future aging countries.
This study focused on the trajectory of smoking in later life and showed that the amount of smoking in later life tends to decline over time. In contrast, most prior studies on smoking trajectories have focused on adolescents and young adults, and in these age groups, the use of tobacco tends to be stable or increase over time (Bernat, Erickson, Widome, Perry, & Forster, 2008; Karp, O’loughlin, Paradis, Hanley, & Difranza, 2005). Therefore, the trajectories of smoking are clearly different between older people and adolescents or younger generations, suggesting the importance of treating older adults as a unique subgroup of the population when studying smoking and its determinants.
Baseline financial strain was associated with higher levels of smoking during the follow-up period. As previous research suggests that members of disadvantaged social status groups experience more exposure to stress (Brunner, 1997), we adjusted for SES, but the association between financial strain and smoking remained (Model 1–4). Moreover, the rate of decline in smoking was slower among people with greater financial strain at baseline (Model 1). These findings support our hypothesis (H1) based on the tension reduction hypothesis.
Research on the association between financial strain and trajectories of smoking among older adults is sparse. In this study, we focused on the between-persons effect that reflects a fundamental difference in the trajectory between the people who feel lots of financial strain and those who feel little. Our study could add a dynamic dimension to understanding the relationship between financial strain and smoking in old age. In later life, many people experience the retirement from their long-term job. In Japan, where a lifetime employment system has long been the norm, retirement often results in substantial loss of income in spite of the pension system (Yashiro & Oshio, 1999). Older Americans also experience financial losses following job loss (Couch, 1998), and a direct association between job loss and smoking intensity and relapse has been observed among them (Falba et al., 2005). Our study provides further evidence that financial hardships during later life may encourage smoking behavior, or inhibit smoking cessation, among older Japanese.
Greater instrumental support partially offset the deleterious effect of financial strain on the rate of decline in smoking (Model 2–4), which supported our second hypothesis (H2). Previous research suggests that members of disadvantaged social status groups have weaker psychological and social resources than their more well-off counterparts (Krause & Borawski-Clark, 1995; Shaw & Krause, 2001). In a U.S. study, smokers of higher SES were more likely than those of lower SES to quit smoking by using effective resources for smoking cessation (Honjo, Tsutsumi, Kawachi, & Kawakami, 2005). Moreover, it was reported that middle-aged and older people with a new diagnosis of a chronic illness tended to quit smoking (Newson et al., 2012). Therefore, we adjusted for variables related to social stratification (age, gender, and SES) and health status in the analysis, but the significant interaction between instrumental support and financial strain on smoking persisted.
Why did instrumental support buffer the effect of financial strain on smoking? By definition, financial strain is a lack of material resources (i.e., money as well as the things that money can buy), and instrumental support is the provision of material resources. Instrumental support could address the needs that are created by the stressor in a more direct way. This is consistent with the basic tenets of the matching hypothesis (Cutrona, 1990). Moreover, Cutrona and Russell (1990) differentiate between controllable and uncontrollable stressors and the life domain in which the stressor occurs. Uncontrollable events, such as the loss of relationships (e.g., death of spouse), require emotional support, particularly comforting, acceptance, and evidence that one is loved. Controllable events, such as the loss of assets, require instrumental support to aid and encourage the individual’s efforts at problem solving. Financial strain can be regarded as a kind of lack of assets (This may be sometimes influenced by economic recessions or depressions that individuals cannot control, but people can predict and prepare it.). Therefore, it stands to reason that instrumental support, not emotional support, was found to buffer the effects of financial strain on smoking.
Older adults might enhance their stress-coping resources through receiving more instrumental support. Such support could aid in coping by providing individuals with access to new contacts and information and could improve an individual’s ability to solve problems. A previous study has reported that received instrumental support increased with advancing age, whereas received emotional support was relatively stable in late life (Shaw, Krause, Liang, & Bennett, 2007). Our study suggests that such increases in instrumental support may help in promoting healthy behaviors in old age.
In addition to the findings described earlier, we did find some direct effects of baseline social support on smoking trajectories. First, instrumental support at baseline was associated with lower levels of smoking at the mean time of follow-up (Model 1–3), but emotional support was not associated with levels of smoking. Unlike emotional support, instrumental support may influence health because this type of support improves access to resources and material goods (Berkman & Glass, 2000). Older people with higher instrumental support have more opportunity to access to resources (e.g., health care services, health-related information) than those with lower support, and then this would influence the lower levels of tobacco use.
Second, people with higher emotional support at baseline had slower rates of decline in smoking over time compared with those with lower levels of support (Model 1–4). The association between time-constant emotional support and smoking trajectories indicates a between-persons effect of social support on smoking and may reflect the greater baseline needs or problems of those who receive an abundance of emotional support. Indeed, a correlation between higher emotional support and poorer health status has been reported in some cross-sectional studies (Finch & Vega, 2003; Stephens, Alpass, Towers, & Stevenson, 2011). Although receiving high emotional support might be a reflection of poorer health conditions, in Model 3 we adjusted for health condition (total conditions, self-rated health, and functional status) and found that the significance of the association between higher emotional support and slower rates of decline in smoking remained. This means that higher emotional support may reflect some other unmeasured health conditions, such as mental illness. Further examination of this issue is needed in future work.
Our findings could have several clinical and policy implications. Independent variables in the model were measured at baseline, and results indicated that the baseline predictors such as financial strain and social support had an impact on smoking trajectories over a long period of time. This implies that even if interventions are short term, interventions aiming to lessen financial strain and to improve social supports could possibly have a long-term effect on preventing or decreasing smoking in older people.
Because the distribution of cigarettes smoked per day was highly skewed, we evaluated our hypotheses by not only treating the amount of smoking as a continuous variable but also treating it as discrete variable consisting of three categories, using a multinomial logistic regression model (see Supplementary Material). The results by multinomial logistic regression model, setting nonsmoking as the reference category, were mostly similar to those from the multilevel linear regression model, except the following three points. First, the interaction between instrumental support and financial strain was significant only for heavy smokers compared with nonsmokers in multinomial logistic regression model. This means that the stress-buffering effect of instrumental support on smoking is likely to be most relevant for heavy smokers. Second, in the multinomial logistic regression models, greater instrumental support at baseline was significantly associated with lower probability of being a moderate smoker during follow-up. The association between baseline instrumental support and the probability of being heavy smoker was also found, but it was marginally significant. Instrumental support that improves people’s access to resources might be more effective on smoking cessation for moderate smokers than heavy smokers because heavy smokers tend to have more difficulty in quitting smoking than moderate smokers (Killen, Fortmann, Telch, & Newman, 1988). Third, although emotional support at baseline was significantly associated with changes in smoking in the multilevel linear regression model, it was not in the multinomial logistic regression model. It is necessary to assess the relationship between emotional support and smoking status further. Thus, although we focus on the result based on the multilevel linear regression models for ease of presentation, the results generated from the multinomial logistic regression models might also provide us further insights on the understanding of smoking in late life.
Moreover, we additionally performed multilevel linear regression models after accounting for the time-varying nature of financial strain and two kinds of social supports (adding both time-constant variables and time-varying variables in the model; data not shown). The associations between the time-constant variables and smoking were same as those generated from models without time-varying variables. This indicates a robustness of evidence supporting our hypothesis, even after adjusting for the time-varying nature of financial strain and social supports.
There are several limitations in this study. First, we relied on self-reported measures of smoking instead of measured level of nicotine. Hence, the level of smoking may be underestimated. Second, because data on smoking before baseline was not available, a proper examination of whether one’s life history of smoking moderates the effects of financial strain on current smoking behavior was not possible. In fact, as some articles hypothesized that smoking status influenced financial strain (Siahpush, Borland, & Scollo, 2003; Siahpush, Spittal, & Singh, 2007), smoking status and financial strain may influence each other. Lifelong evaluation of both smoking behavior and financial strain would be necessary to fully evaluate these possibilities. Third, period effects may influence the results of this study. For example, in Japan, the Health Promotion Act to curb passive smoking in public spaces was not enacted until 2003. Treatment for smoking cessation was not covered by health insurance until 2006. The trajectory of smoking behavior might be influenced by these health policies related to smoking. Moreover, financial strain may be also affected by economic trends. Year of baseline survey and follow-up duration are different by each participant. Therefore, we must carefully interpret the findings in this study, taking into consideration the data collection period.
In conclusion, this study, using longitudinal data of Japanese elderly adults spread over 19 years , revealed that regardless of social support, people who are financially strained are likely to smoke more than those who are not strained. However, those financially strained individuals with greater instrumental support are likely to decline their smoking, suggesting a stress-buffering role of instrumental support with reference to financial strain. Our findings can contribute to a greater understanding of the relationship between financial strain and smoking and the stress-buffering effect of social support. These findings can also provide new insights into the design of health policies and interventions regarding health behaviors in order to promote and maintain health in late life.
Supplementary Material
Supplementary material can be found at: http://psychsocgerontology.oxfordjournals.org/.
Funding
This work was supported by the National Institute on Aging (R01 AG031109, P60 AG024824) at the National Institutes of Health.
Supplementary Material
References
- Abbey A., Smith M. J., Scott R. O. (1993). The relationship between reasons for drinking alcohol and alcohol consumption: An interactional approach. Addictive Behaviors, 18, 659–670. 10.1016/0306-4603(93)90019-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bandura A. (1997). Self-efficacy: The exercise of control. New York, NY: W.H. Freeman. [Google Scholar]
- Berkman L. F., Glass T. (2000). Social integration, social networks, and social support, and health. In Berkman L. F., Kawachi I. (Eds.), Social epidemiology (pp. 137–173). New York, NY: Oxford University Press. [Google Scholar]
- Bernat D. H., Erickson D. J., Widome R., Perry C. L., Forster J. L. (2008). Adolescent smoking trajectories: Results from a population-based cohort study. Journal of Adolescent Health, 43, 334–340. 10.1016/j.jadohealth.2008.02.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brunner E. (1997). Socioeconomic determinants of health: Stress and the biology of inequality. British Medical Journal, 314, 1472–1476. 10.1136/bmj.314.7092.1472 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Budescu M., Taylor R. D., McGill R. K. (2011). Stress and African American women’s smoking/drinking to cope: Moderating effects of kin social support. Journal of Black Psychology, 37, 452–484. 10.1177/0095798410396087 [Google Scholar]
- Businelle M. S., Kendzor D. E., Reitzel L. R., Costello T. J., Cofta-Woerpel L., Li Y, … Wetter D. W. (2010). Mechanisms linking socioeconomic status to smoking cessation: A structural equation modeling approach. Health Psychology, 29, 262–273. 10.1037/a0019285 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. (2011). Vital signs: Current cigarette smoking among adults aged ≥18 years: United States 2005–2010. Morbidity and Mortality Weekly Report, 60, 1207–1212. [PubMed] [Google Scholar]
- Cohen S., McKay G. (1984). Social support, stress and the buffering hypothesis: A theoretical analysis. In Baum A., Taylor S. E., Singer J. E. (Eds.), Handbook of psychology and health (pp. 253–267). Mahwah, NJ: Hillsdale. [Google Scholar]
- Couch K. A. (1998). Late life job displacement. The Gerontologist, 38, 7–17. 10.1093/geront/38.1.7 [DOI] [PubMed] [Google Scholar]
- Cutrona C. E. (1990). Stress and social support: In search of optimal matching. Journal of Social and Clinical Psychology, 9, 3–14. 10.1521/jscp.1990.9.1.3 [Google Scholar]
- Cutrona C. E., Russell D. W. (1990). Type of social support and specific stress: Towards a theory of optimal matching. In Sarason B. R., Sarason I. G., Pierce G. R. (Eds.), Social support: An interactional view (pp. 319–366). New York, NY: John Wiley. [Google Scholar]
- Falba T., Teng H. M., Sindelar J. L., Gallo W. T. (2005). The effect of involuntary job loss on smoking intensity and relapse. Addiction, 100, 1330–1339. 10.1111/j.1360-0443.2005.01150.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Finch B. K., Vega W. A. (2003). Acculturation stress, social support, and self-rated health among Latinos in California. Journal of Immigrant Health, 5, 109–117. 10.1023/A:1023987717921 [DOI] [PubMed] [Google Scholar]
- Fujisawa K., Takata Y., Matsumoto T., Esaki M., Ansai T., Iida M. (2008). Impact of smoking on mortality in 80-year-old Japanese from the general population. Gerontology, 54, 210–216. 10.1159/000138336 [DOI] [PubMed] [Google Scholar]
- Greeley J., Oei T. (1999). Alcohol and tension reduction. In Leonard K. E., Blane H. T. (Eds.), Psychological theories of drinking and alcoholism (pp. 14–53). New York, NY: Guilford Press. [Google Scholar]
- Heaney C. A., Israel B. A. (2008). Social networks and social support. In Glanz K., Rimer B. K., Viswanath K. (Eds.), Health behavior and health education: Theory, research, and practice (pp.189–210). San Francisco, CA: Jossey-Bass. [Google Scholar]
- Hiscock R., Bauld L., Amos A., Fidler J. A., Munafò M. (2012). Socioeconomic status and smoking: A review. Annals of the New York Academy of Sciences, 1248, 107–123. 10.1111/j.1749-6632.2011.06202.x [DOI] [PubMed] [Google Scholar]
- Honjo K., Tsutsumi A., Kawachi I., Kawakami N. (2005). What accounts for the relationship between social class and smoking cessation? Results of a path analysis. Social Science & Medicine, 62, 317–328. 10.1016/j.socscimed.2005.06.011 [DOI] [PubMed] [Google Scholar]
- Institute for Health Economics and Policy. (2010). Study for anti-smoking measures [Kinen sesaku no arikata ni kansuru kenkyu]. Tokyo, Japan: Author. [Google Scholar]
- Karp I., O’loughlin J., Paradis G., Hanley J., Difranza J. (2005). Smoking trajectories of adolescent novice smokers in a longitudinal study of tobacco use. Annals of Epidemiology, 16, 445–452. 10.1016/j.annepidem.2004.10.002 [DOI] [PubMed] [Google Scholar]
- Katanoda K., Marugame T., Saika K., Satoh H., Tajima K., Suzuki T, … Sobue T. (2008). Population attributable fraction of mortality associated with tobacco smoking in Japan: A pooled analysis of three large-scale cohort studies. Journal of Epidemiology, 18, 251–264. 10.2188/jea.JE2007429 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Killen J. D., Fortmann S. P., Telch M. J., Newman B. (1988). Are heavy smokers different from light smokers? A comparison after 48 hours without cigarettes. Journal of American Medical Association, 260, 1581–1588. 10.1001/jama.1988.03410110089033 [PubMed] [Google Scholar]
- Krause N. (1987). Chronic strain, locus of control, and distress in older adults. Psychology and Aging, 2, 375–382. 10.1037/0882-7974.2.4.375 [DOI] [PubMed] [Google Scholar]
- Krause N., Borawski-Clark E. (1995). Social class differences in social support among older adults. The Gerontologist, 35, 498–508. 10.1093/geront/35.4.498 [DOI] [PubMed] [Google Scholar]
- Krause N., Newsom J. T., Rook K. S. (2008). Financial strain, negative social interaction, and self-rated health: Evidence from two nationwide longitudinal surveys. Aging & Society, 28, 1001–1023. 10.1017/S0144686X0800740X [Google Scholar]
- Kendzor D. E., Businelle M. S., Costello T. J., Castro Y., Reitzel L. R., Cofta-Woerpel L. M, … Wetter D. W. (2010). Financial strain and smoking cessation among racially/ethnically diverse smokers. American Journal of Public Health, 100, 702–706. 10.2105/AJPH.2009.172676 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liang J., Bennett J. M., Sugisawa H., Kobayashi E., Fukaya T. (2003). Gender differences in old age mortality: Roles of health behavior and baseline health status. Journal of Clinical Epidemiology, 56, 572–582. 10.1016/S0895-4356(03)00060-X [DOI] [PubMed] [Google Scholar]
- Ministry of Health, Labour and Welfare. (2011). National Health Nutrition Survey 2010. Tokyo, Japan: Author. [Google Scholar]
- Muratani H., Kimura Y., Fukiyama K., Kawano Y., Fujii J., Abe K, … Omae T. (2000). Control of blood pressure and lifestyle-related risk factors in elderly Japanese hypertensive subjects. Hypertension Research, 23, 411–449. 10.1291/hypres.23.441 [DOI] [PubMed] [Google Scholar]
- Nelson M. C., Lust K., Story M., Ehlinger E. (2008). Credit card debt, stress and key health risk behaviors among college students. American Journal of Health Promotion, 22, 400–407. 10.4278/ajhp.22.6.400 [DOI] [PubMed] [Google Scholar]
- Newson J. T., Huguet N., McCarthy M. J., Ramage-Morin P., Kaplan M. S., Bernier J, … Oderkirk J. (2012). Health behavior change following chronic illness in middle and later life. Journals of Gerontology: Psychological Sciences and Social Sciences, 67, 279–288. 10.1093/geronb/gbr103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ozasa K., Katanoda K., Tamakoshi A., Sato H., Tajima K., Suzuki T, … Sobue T. (2008). Reduced life expectancy due to smoking in large-scale cohort studies in Japan. Journal of Epidemiology, 18, 111–118. 10.2188/jea.JE2007416 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raudenbush S. W., Bryk A. S. (2002). Hierarchical linear models: Applications and data analysis methods (2nd ed). Thousand Oaks, CA: Sage. [Google Scholar]
- Sapp A. L., Kawachi I., Sorensen G., LaMontagne A. D., Subramanian S. V. (2010). Does workplace social capital buffer the effects of job stress? A cross-sectional, multilevel analysis of cigarette smoking among U.S. manufacturing workers. Journal of Occupational and Environmental Medicine, 52, 740–750. 10.1097/JOM.0b013e3181e80842 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schafer J. L. (1997). Analysis of incomplete multivariate data. London: Chapman & Hall. [Google Scholar]
- Shaw B. A., Agahi N., Krause N. (2011). Are changes in financial strain associated with changes in alcohol use and smoking among older adults? Journal of Studies on Alcohol and Drugs, 72, 917–925. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shaw B. A., Krause N. (2001). Exploring race variations in aging and personal control. Journals of Gerontology: Psychological Sciences and Social Sciences, 56, 119–124. 10.1093/geronb/56.2.S119 [DOI] [PubMed] [Google Scholar]
- Shaw B. A., Krause N., Liang J., Bennett J. (2007). Tracking changes in social relations throughout late life. Journal of Gerontology: Psychological Sciences and Social Sciences, 62, 90–99. [DOI] [PubMed] [Google Scholar]
- Siahpush M., Borland R., Scollo M. (2003). Smoking and financial stress. Tobacco Control, 12, 60–66. 10.1136/tc.12.1.60 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Siahpush M., Carlin J. B. (2006). Financial stress, smoking cessation and relapse: Results from a prospective study of an Australian national sample. Addiction, 101, 121–127. 10.1111/j.1360-0443.2005.01292.x [DOI] [PubMed] [Google Scholar]
- Siahpush M., Spittal M. M., Singh G. K. (2007). Association of smoking cessation with financial stress and material well-being: Results from a prospective study of a population-based national survey. American Journal of Public Health, 97, 2281–2287. 10.2105/AJPH.2006.103580 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Siahpush M., Yong H. H., Borland R., Reid J. L., Hammond D. (2009). Smokers with financial stress are more likely to want to quit but less likely to try or succeed: findings from the International Tobacco Control (ITC) Four Country Survey. Addiction, 104, 1382–1390. 10.1111/j.1360-0443.2009.02599.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stephens C., Alpass F., Towers A., Stevenson B. (2011). The effects of types of social networks, perceived social support, and loneliness on the health of older people: Accounting for the social context. Journal of Aging and Health, 23, 887–911. 10.1177/0898264311400189 [DOI] [PubMed] [Google Scholar]
- Tsubota-Utsugi M., Ito-Sato R., Ohkubo T., Kikuya M., Asayama K., Metoki H, … Imai Y. (2011). Health behaviors as predictors for declines in higher-level functional capacity in older adults: The Ohasama study. Journal of American Geriatric Society, 59, 1933–2000. 10.1111/j.1532-5415.2011.03633.x [DOI] [PubMed] [Google Scholar]
- Turner L. R., Mermelstein R., Hitsman B., Warnecke R. B. (2008). Social support as a moderator of the relationship between recent history of depression and smoking cessation among lower-educated women. Nicotine & Tobacco Research, 10, 201–212. 10.1080/14622200701767738 [DOI] [PubMed] [Google Scholar]
- van Loon A. J. M., Tijhuis M., Surtees P. G., Ormel J. (2005). Determinants of smoking status: Cross-sectional data on smoking initiation and cessation. European Journal of Public Health, 15, 256–261. 10.1093/eurpub/cki077 [DOI] [PubMed] [Google Scholar]
- Westmaas J. L., Bontemps-Jones J., Bauer J. E. (2010). Social support in smoking cessation: Reconciling theory and evidence. Nicotine & Tobacco Research, 12, 695–707. 10.1093/ntr/ntq077 [DOI] [PubMed] [Google Scholar]
- Yashiro N., Oshio T. (1999). Social security and retirement in Japan. In Gruber J., Wise D. A. (Eds.), Social security and retirement around the world (pp. 239–267). Chicago, IL: Chicago University Press. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.