

Abstract
Objectives.
(a) To identify factors associated with different patterns of functional decline in a longitudinal sample of older Mexican-origin individuals, and (b) to determine the proportions of life after age 65 characterized by serious functional impairment.
Methodology.
We use the Hispanic Established Populations for Epidemiologic Studies of the Elderly to examine changes in objective Performance Oriented Mobility Assessments in a cohort of 3,050 Mexican-origin elders initially interviewed in 1993/1994 and recontacted 6 times over 17 years. This sample combined with an additional cohort of 902 individuals 75 and older added at wave 4 in 2004/2005 (combined sample = 3,952) is used in life table analyses to estimate the number of years after 65 characterized by serious functional impairment.
Results.
Three distinct patterns of functional decline emerge: (a) high initial functioning followed by decline, but not to the level of disability (48%); (b) moderate initial functioning followed by decline to the level of disability (37.5%); and (c) initial disability followed by continued poor functioning (14.5%). Life table analyses reveal that subjects spent over half of the period after 65 with serious functional limitations. Significant gender and nativity differentials emerge.
Discussion.
Protracted morbidity that accompanies increases in life expectancy has serious implications for the physical, social, and economic well-being of older individuals and their families, as well as for health and long-term care policy.
Key words: Active life expectancy, Disability trajectory, Functional capacity, H-EPESE, Hispanic, Longevity.
Increases in life expectancy during the last century reflect clear improvements in human lives (Elo, 2009; United Nations, 2011), but they also confront developed and developing nations with new and serious challenges related to the support of rapidly growing older populations, a large fraction of whom will experience serious health problems. Today, individuals over eighty make up the fastest growing segment of the elderly population (Werner, 2011). These new challenges are compounded by the fact that developing and developed nations face a period that may be characterized by protracted fiscal austerity. A long and healthy life may be everyone’s desire, but a long life is not synonymous with high-quality life or a high level of functioning. For groups with low levels of education, income, and wealth, longer life may bring prolonged periods of poor functioning, dependency, and poverty.
In this paper, we address issues related to the possibility of limitations to the potential postponement of morbidity as life spans increase in a longitudinal sample of Mexican-origin elders. Although improvements in medical care and better preventive care may postpone death, the effects of fundamental causes of impaired functioning may be more difficult to postpone, resulting in a protracted period of disability prior to death (Fries, 2003). Our analyses address two interrelated questions that require two overlapping samples and two different methodological approaches. The first question relates to patterns of change in functional capacity and their predictors in a cohort of Mexican-origin individuals 65 and over first interviewed in 1993/1994 and recontacted in six additional waves over 17 years. The long follow-up makes this analysis possible. The second question more specifically addresses the issues of the proportion of years after 65 characterized by serious functional disability. To answer this question we employ the original cohort combined with a supplemental sample consisting of 902 individuals 75 and older, that was added at wave 4 in 2004/2005 to compensate for attrition through death of members of the original cohort. This combined sample provides a large number of person-years of data and allows us to employ life table techniques to estimate the number of years after age 65 in which individuals suffer significant functional impairment.
These two sets of analyses, then, allow us (a) to identify the medical, social, and cultural predictors of different patterns of decline and (b) to compare the extent of the compression or extension of morbidity among foreign and U.S.-born men and women. The use of the two overlapping data sets permits a more detailed examination of functional capacity and its predictors than would either data set alone. These unique data comprise the largest and longest longitudinal study of older Mexican-origin adults available and provide the first comprehensive portrait of patterns and trajectories of disability in this population.
Our focus on the Mexican-origin population is motivated by certain anomalies related to this population’s favorable mortality experience despite a disadvantaged socioeconomic profile. On average, the Mexican-origin population has low levels of education and health insurance coverage, as well as low levels of income and wealth. Mexican-origin individuals experience elevated rates of diabetes, hypertension, and disability, yet their mortality profile is remarkably favorable compared to non-Hispanic whites and African Americans (Markides & Eschbach, 2005; Palloni, 2007). In 2010, life expectancy at birth for Hispanics was 81.2 compared to 78.8 for non-Hispanic whites and 74.7 for African Americans. At age 65 remaining life expectancy for Hispanic men and women was 18.8 and 22.0, while for non-Hispanic white men and women it was 17,7 and 20.3, and for African American men and women it was 15.8 and 19.1 (National Center for Health Statistics, 2014). The favorable mortality profile among Hispanics raises many important theoretical and practical questions, both with reference to the implications for the Hispanic population itself given its high rate of poverty at all ages, but also for the nation as a whole, given the high societal costs of long-term and acute care for a population with potentially high rates of serious disability.
A core objective of public health and preventive medicine is the extension of the period of life during which one is functioning at a high level. In the ideal case, an individual would experience a brief period of incapacity and decline near the end of life. Such an outcome requires that in addition to postponing death, medical science and public health postpone the onset of disability. The alternatives to a long life with a short period of disability are (a) early-onset disability accompanied by a relatively short period of incapacity before an early death; and (b) perhaps worst of all from a resource demand perspective, early-onset disability accompanied by a long period of incapacity before death.
The Public Policy Dilemma
This latter possibility, a long life with extended disability, leads to a basic dilemma that we might term a “public health or prevention paradox.” If it is the case that we can increase life expectancy through medical interventions and behavioral risk reduction, but find that we are less successful at preventing or significantly postponing the onset of disabling disease, the inevitable result may be that longer lives mean more unavoidable disability. This would happen if mortality from diseases that kill one fairly early on, such as behavior-related cancers and cardiovascular disease can be controlled, but declines associated with less controllable causes that do not kill one immediately cannot. The degenerative and incapacitating diseases of old age may simply be less amenable to prevention. They might be postponed for a brief period, but may not be preventable. Fundamental causes associated with aging may mean that if one lives long enough, one’s risk of illness and disability is very high (Link & Phelan, 1995). In which case, we may be caught in the paradox of extending lives through interventions only to inevitably increase the period of compromised functioning. If prevention is not possible, medical management and assistance may be the only option. This means that longer lives could result in greatly increased expenditures associated with increased dependency.
These two scenarios, the late and early onset of morbidity, have clear and profoundly different implications for public policy at the federal and state levels, as well as for individual and family finances and welfare. A long and healthy life gives one the opportunity to remain engaged and active and to avoid becoming a burden on one’s family or on society. A long but unhealthy life implies the opposite, a potentially long period of dependency and medical care use and potentially onerous financial and care giving burdens for families and the state. A large fraction of the medical care that individuals consume in their lives occurs during the last few years of life (Cohen & Yu, 2012). In the absence of significant rationing, the extension of morbidity would almost inevitably increase the aggregate consumption of expensive medical services.
Disability rates by age have decreased over the last 30 years as life expectancy has increased (Freedman, Schoeni, Martin, & Cornman, 2007). Self-reported disability rates, though, differ significantly by race and Hispanic ethnicity (Brown, O’Rand, & Adkins, 2012; Cantu, Hayward, Hummer, & Chiu, 2013; Haan, Zeki Al-Hazzouri, & Aiello, 2011; Haas & Rohlfsen, 2010; Haas, Krueger, & Rohlfsen, 2012; Hayward, Hummer, Chiu, González-González, & Wong, 2014; Hayward, Warner, & Crimmins, 2007; Quiñones, Liang, Bennett, Xu, & Ye, 2011; Taylor & Lynch, 2004). This variation raises the possibility that among disadvantaged groups longer lives may be accompanied by significant morbidity. The present study builds upon previous work by employing an objective measure of functional capacity, the performance-oriented mobility assessment (POMA), to examine the proportion of years after age 65 that are characterized by serious disability. The POMA instrument is widely used in clinical settings to provide an objective evaluation of such physical performance abilities as balance, the ability to stand and to walk, the ability to get out of a chair, and grip strength. It is used to assess changes in these abilities over time (Faber, Boscher, & van Wieringen, 2006).
One recent study employed physical performance assessments to investigate differences among respondents by race and Hispanic ethnicity. Using data from the Health and Retirement Study (HRS) 2004, 2006, and 2008 cohorts Hass and colleagues found that Hispanic immigrants had poorer performance outcomes in terms of lung function, longer walk times, and grip strength than non-Hispanic whites and U.S.-born Hispanics (Haas et al., 2012). However, consistent with the Hispanic paradox, both U.S.-born and foreign-born Hispanics in the HRS were more likely to have better lung function than non-Hispanic whites after adjusting for a range of relevant covariates. These findings based on a small sample of Hispanics reveal great heterogeneity in late life physical performance based on nativity, race, and Hispanic ethnicity and point to the need to further investigate the social distribution of decline.
Data
Our objective in what follows is to identify major functional profiles of decline in POMAs as a function of age among older Mexican-origin individuals and to identify major correlates of different patterns employing a unique and important longitudinal data set, the Hispanic Established Population for Epidemiologic Studies of the Elderly or H-EPESE (Markides, Rudkin, Angel, & Espino, 1997). These data provide detailed information on risk factors for mental and physical illness and mortality for a sample of 3,050 individuals of Mexican-origin in the United States living in the five southwestern states of Arizona, California, Colorado, New Mexico, and Texas who were 65 and older when they were first interviewed in 1993–1994. This panel was re-contacted in 1995–1996, 1998–1999, 2000–2001, 2004–2005, 2007, and 2010–2011. This sample is used in our first analysis of patterns of decline in functional capacity. Due to sample attrition either from non-response or loss to follow up over the seven waves, our final analytic sample for this analysis is 2,455 respondents. Sensitivity analyses (available upon request) were conducted in order to assess the extent to which loss to follow-up might affect interpretation of findings. No significant differences between groups emerged from the results.
A second objective of our analysis is to estimate the proportion of life spent in a highly disabled state prior to death for U.S.-born and foreign-born men and women. Because of attrition in the original cohort, in 2004 a new cohort of 902 individuals who were the same age as the original cohort (75 or older at the time) was added to increase sample size and statistical power. This new panel was recontacted in 2007 and 2010–2011. This enhanced sample is used for our second analysis of the proportion of the life course characterized by significant impairment. This second analysis is based on 3,952 individuals and 35,674 person-years of data. Of the initial sample, 434, or 14.2%, were lost to follow up by 2010–2011. In the baseline sample, 1,957, or 64.2% of the sample, died by the end of the study. Among the survivors of the original cohort 659, or 21.6% were reinterviewed in 2010–2011. Of these 115, or 11.1% were proxies. In the combined cohort, which includes the original cohort and the additional cohorts of 902 individuals 75 and older added at wave 5 in 2004–2005, 2,356, or 59.6% of the sample had died by wave 7. Among the survivors, 1,076 were reinterviewed at wave 7 and 520 or 13.2% were lost to follow up.
Measures
Physical Mobility
In the following analyses we employ three of the POMA tasks (a) standing balance (semi-tandem and side by side), (b) a timed 8-ft walk at a normal pace (gait speed), and (c) a timed test of five repetitions of rising from a chair and sitting down (Guralnik, Ferrucci, Simonsick, Salive, & Wallace, 1995). Following the work of Markides and colleagues (Markides et al., 2001), each assessment was coded (0) unable to complete task, (1) poor, (2) fair, (3) good, and (4) best. Respondents who received a score of (0) included those who tried but were unable to complete the task and those who did not attempt the task for safety reasons. A total POMA score ranged from 0 to 12, with higher scores indicating better physical functioning. The POMAs were assessed at each wave and form the basis for both the pattern analysis and the life table analyses of the proportion of life characterized by serious functional limitation.
Independent variables included in the multivariate regressions for the POMA change analyses include the following predictor variables measured at time one (1993–1994).
Mental and Physical Health
To assess depressive affect we used the center for epidemiologic studies depression scale (CES-D) from the first wave. The CES-D consists of 20 items (Radloff, 1977). Respondents were asked to indicate the frequency of depressive symptoms experienced in the past week. We coded the original response categories for these items as (1) rarely or none of the time, (2) some of the time, (3) occasionally, and (4) most or all of the time. The final CES-D score ranges from 0 to 54 with a mean of 14.9.
To control for cognitive capacity we used the mini-mental state examination (MMSE), measured at wave 1. The MMSE is one of the most commonly used brief cognitive screening devices in studies of older adults (Folstein, Folstein, & McHugh, 1974). It is based on a standard battery of memory and reasoning items and assesses orientation, attention, immediate and short-term recall, language, and the ability to follow simple verbal and written commands. Following recent research we employ the continuous specification of MMSE (Hill, Angel, & Balistreri, 2012).
We control for a number of chronic conditions at baseline, including diabetes, hypertension, stroke, and heart attack. Respondents were asked to indicate whether they had ever been told by a doctor that they had any of these conditions. We coded responses as (1) for yes and as (0) otherwise. Blood pressure was directly measured with a standard mercury sphygmomanometer. Two readings were taken for each respondent, and an average systolic and diastolic blood pressure was recorded. We coded respondents as positive for hypertension if their average systolic reading was 140 mmHg or higher or their average diastolic reading was 90 mmHg or higher.
Health Behavior and Body Mass
Our measurement of health behaviors is based on responses to questions concerning smoking and drinking at baseline. Respondents were asked whether they were current smokers. They were also asked whether they had any alcohol during the past month. We coded response categories for these items as (1) for yes and (0) otherwise. Anthropometric measurements of height and weight were collected in the respondent’s home. Using the standard formula and documented thresholds provided by the Centers for Disease Control, we coded respondents as (1) obese (BMI ≥ 35) and (0) otherwise.
Nativity and Age at Migration
Following previous research (Angel, Angel, & Hill, 2009; Hill, Angel, Balistreri, & Herrera, 2012), we created four nativity status and life course stage at migration categories. Category 1 consists of those who were born in the United States; Category 2 consists of those who were born in Mexico and migrated to the United States before the age of 20; Category 3 consists of those who were born in Mexico and migrated to the United States between the ages of 20 and 49 years; and Category 4 consists of those who were born in Mexico and migrated to the United States after the age of 50. In our multivariate analyses, Group 1, U.S.-born, serve as the reference category.
Background Factors
Our multivariate analyses include controls for age, gender, education, financial strain, marital status, living arrangements, monthly contact with family and friends, and perceived social support derived from the baseline survey. Age is entered as a continuous variable. Financial strain was measured with two items. Respondents were asked, “[h]ow much difficulty do you have in meeting monthly payments on your bills?” Response categories for this item were coded (1) none, (2) a little, (3) some, and (4) a great deal. Respondents were also asked, “[a]t the end of the month, do you usually end up with some money left over, just enough to make ends meet, or not enough to make ends meet?” Response categories for this item were coded (1) some money left over, (2) just enough to make ends meet, and (3) not enough money to make ends meet. We measured financial strain as the mean response to these two items. These items were standardized to account for metric differences. Our measure of social support is the mean response to two items. Respondents were asked, “In times of trouble, can you count on at least some of your family or friends?” Respondents were also asked, “Can you talk about your deepest problems with at least some of your family or friends?” Response categories for these items were coded (0) hardly ever, (1) some of the time, or (2) most of the time. Marital status (married), living arrangement (live with others), education (having less than a high school education), and gender (male) were dichotomized in the analyses with the reference category in parentheses.
Statistical Procedures
Our analyses are based on two samples and two statistical techniques. The first set of analyses is based on the original sample of 3,050 respondents, 1,957 of whom had died and 659 of whom were reinterviewed in 2010–2011. In this analysis we identify patterns of decline over the seven waves of data using growth mixture modeling (GMM) from Mplus 6.12 (Figure 1). Although the identification of categories (classes) of change in functional capacity requires some judgment, GMM provides a systematic and structured method of identifying substantively meaningful subgroups in a sample based on patterns of longitudinal change (Jung & Wickrama, 2008; Ram & Grimm, 2009).
Figure 1.
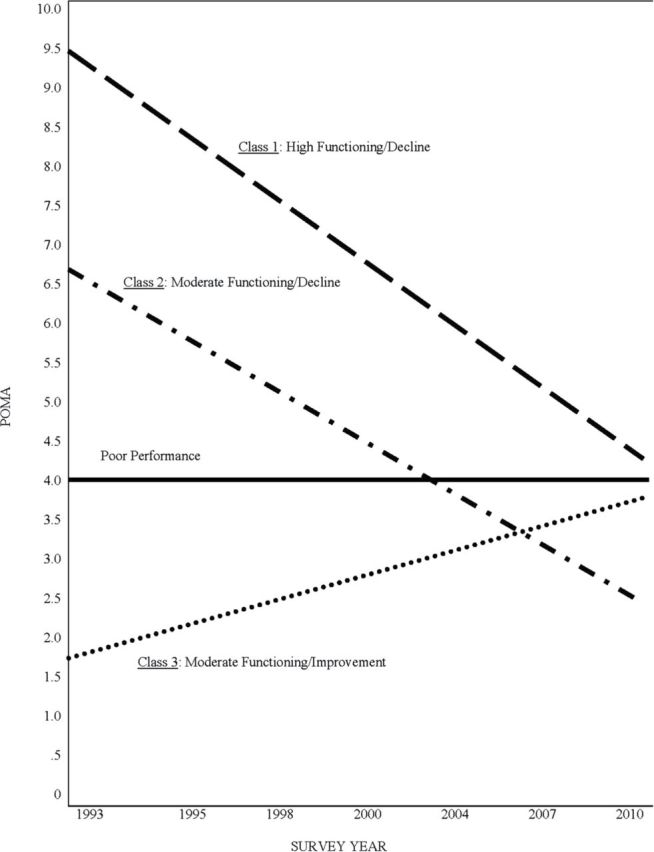
Performance oriented mobility assessment (POMA) classes, 1993–2011.
Once we identify the number of meaningful latent subpopulations in the data we determine the predictors of each pattern in greater detail. In order to accomplish this, we employ a series of pair-wise t-tests to assess unadjusted mean differences in our focal variables across the identified POMA pattern groupings (Table 1). We then estimate a series of multinomial logistic regression models to predict the odds of membership in the various POMA decline groups.
Table 1.
Baseline Sample Means by POMA Trajectory Classes (H-EPESE)
| Class 1 remained non-disabled (n = 1,178) | Class 2 became disableda (n = 911) | Class 3 remained disabledb (n = 356) | |
|---|---|---|---|
| Age | 71.34a,b | 71.89b | 75.24 |
| Female | .46a | .54 | .53 |
| Education (≥ HS) | .16a,b | .06 | .09 |
| Financial strain | –.11a,b | .11 | .08 |
| Unmarried | .37b | .40 | .48 |
| Lives alone | .21 | .23 | .28 |
| No contact w/family and friends | .15 | .13 | .19 |
| Social support | 1.62 | 1.63 | 1.56 |
| U.S.-born | .57a | .63 | .59 |
| Immigrant (1–19) | .08a,b | .15 | .18 |
| Immigrant (20–49) | .25a,b | .17 | .17 |
| Immigrant (50+) | .09a | .05 | .06 |
| CES-D | 14.43b | 14.16b | 17.53 |
| MMSE | 26.18a,b | 25.36b | 24.11 |
| Smoker | .17a,b | .12 | .10 |
| Drinker | .25a,b | .14 | .07 |
| Obese | .23a,b | .35 | .37 |
| Diabetic | .24b | .28b | .37 |
| Hypertensive | .39a | .50 | .43 |
| History of heart attack | .09 | .10 | .12 |
| History of stroke | .04b | .05b | .10 |
| POMA | 9.51a,b | 6.36b | 1.09 |
Notes. CES-D = center for epidemiologic-depression scale; H-EPESE = Hispanic established populations for the epidemiologic study of the elderly, n = 2,455; HS = high school; MMSE = mini-mental state exam. POMA = performance oriented mobility assessment. BIC = 50119.55 and LMR-LRT = 88.137 (p < .05).
a,bIdentifies significant mean differences between designated classes (two-tailed t-tests, p < .05).
The second set of analysis is based on the original sample and the new cohort that was added at wave 5 in 2004–2005 to increase the total sample size. The addition of the new cohort increased the sample size to 3,952. Of this sample, 2,356 had died by wave 7 and 1,076 survivors were recontacted. This sample allows us to compute person-years of life with and without disability. We employ age-specific mortality rates with age-specific prevalence of POMA limitations to calculate Sullivan-based multistate life table models of the number of years of life free of POMA limitations relative to life expectancy with POMA limitations for each group of interest (Sullivan, 1971). This method allows us to calculate the ratio of the number of healthy, POMA-free years to the number of unhealthy, POMA-limited years. For the three POMAs we employ in this analysis a score of 0 means the test cannot be performed and a score of 1 reflects extremely low functioning. Scores greater than 1 indicate moderate to high functioning. In the following analysis we define impaired as a score of 0 or 1 on any of the three POMAs employed. Deaths are determined via mortality link and proxy reports.
To estimate mortality rates, Gompertz models of the following form stratified by sex and nativity are used.
| (1) |
where, x is age. To estimate prevalence probability, the logistic regressions of the following form stratified by sex and nativity are fit.
| (2) |
where, π is the prevalence probability. Equation 1 allows us to estimate age-specific mortality rates and total life expectancy for the sample. Equation 2 allows us to estimate the age-specific prevalence of POMA limitations for each group of interest. The estimated prevalence is used to divide total life expectancy into the number of years lived in different functional status states based on the age-specific prevalence of healthy (POMA limitations free) relative to unhealthy (with POMA limitations) person years. For a more detailed explanation refer to Jagger, Cox, Le Roy, and EHEMU (2006). The unhealthy life expectancies are estimated using logistic regression to predict the age specific prevalence rates for POMA disability. A bootstrapping technique is used to obtain standard errors for the total life expectancy, healthy life expectancy, and unhealthy life expectancy estimates.
Results
Growth Mixture Modeling Analysis
The GMM analysis is based on the original cohort that was followed for all seven waves. To determine the appropriate number of POMA pattern classes, we fit three consecutive GMM models that included adjustments for age, gender, education, financial strain, marital status, nativity and age at migration, body mass, and chronic conditions. These models include the dead and produce full information estimates of class patterns based on the existing data for all individuals in the sample.
Our first model specified two POMA pattern classes and resulted in a Bayesian information criterion (BIC) of 50143.54 and a Lo-Mendell-Rubin adjusted likelihood ratio test test (LMR-LRT) of 481.886 (p < .001). The statistically significant LMR-LRT suggested that the two-pattern model fit the data better than the one-pattern model. Our second model specified three POMA pattern classes and resulted in a BIC of 50119.55 and a LMR-LRT of 88.137 (p < .05). Again, the statistically significant LMR-LRT suggested that the three-pattern model fit the data better than the initial two-pattern model. Our final model specified four POMA pattern classes and resulted in a BIC of 50360.98 and a LMR-LRT of 85.532 (p < .10). In the end, we selected the three-pattern model because it resulted in the lowest BIC, and the LMR-LRT for the four-pattern model was not statistically significant at conventional levels, suggesting no improvement in model fit over the three-pattern model.
Figure 1 presents a graphical illustration of the three POMA patterns. The threshold for poor performance on the POMAs is indicated by the horizontal dark line in the middle of the figure. The first pattern, class 1 (remained non-disabled), is characterized by initially high functioning followed by decline and includes 48% of the sample. Even though most declined somewhat given their age at baseline, over the study period (approximately 17 years), respondents in this group remained above the threshold for poor functioning. The second pattern, class 2 (became non-disabled) includes initial fair functioning followed by significant decline and includes 37.5% of the sample. These individuals were above the threshold at baseline, but dropped below the threshold by the final interview. On average, they remained above the threshold for poor functioning over the first five waves (approximately 11 years), but dropped below the threshold by the time of the final two waves. The third pattern, class 3 (remained disabled) reflects initial poor functioning, followed by little change or even slight improvement and includes 14.5% of the sample. These individuals remained below the functional impairment threshold throughout the study. Despite some moderate improvement they stayed below the threshold for poor functioning over the seven waves.
Bivariate Analysis
Table 1 presents sample means for all study variables across the GMM POMA pattern classes. On average, respondents in class 1 are younger, more highly educated, and more financially stable than respondents in class 2 and class 3. Respondents in class 1 are more likely to have immigrated during middle-life than respondents in class 2 and class 3. They are also more likely to have immigrated during late-life than respondents in class 2. With respect to health behavior and body mass, respondents in the first class are more likely to smoke and drink, but less likely to be obese, than respondents in class 2 and class 3. In terms of mental and physical health, respondents in class 1 have higher cognitive and physical functioning than respondents in class 2 and class 3. Respondents in class 1 also have lower rates of hypertension than respondents in class 2 and lower rates of stroke and diabetes than respondents in class 3.
Multivariate Analysis
Table 2 provides multinomial logistic regression results predicting the odds of POMA class membership. Three contrasts, each with two analyses are presented. The first two columns compare those who remained non-disabled (class 1) to those who remained disabled (class 3). In model 1, the odds of remaining non-disabled versus remaining disabled are lower for older adults, women, and respondents with higher levels of financial strain. This model also indicates that the odds of remaining non-disabled as opposed to remaining disabled are higher for respondents who immigrated during middle- and late-life than for the U.S.-born or those who immigrated early in life.
Table 2.
Multinomial Logistic Regression Predicting the Odds of POMA Class Membership
| Class 1 vs Class 3, remained non-disabled vs remained disabled | Class 2 vs Class 3, became disabled vs remained disabled | Class 1 vs Class 2, remained non-disabled vs became disabled | ||||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | |
| Age | .90*** (.88, .92) | 1.01 (.92, 1.1) | .92*** (.90, .94) | 0.97 (.90, 1.1) | .97** (.96, .99) | 1.03 (.99, 1.1) |
| Female | .65** (.50, .86) | 6.92** (2.1, 22.2) | 1.02 (.77, 1.3) | 4.00* (1.4, 11.7) | .64*** (.53, .78) | 1.73* (1.1, 2.7) |
| Education (≥ HS) | 1.54 (.99, 2.4) | 1.02 (.18, 5.7) | .54* (.33, .88) | .21 (.04, 1.0) | 2.87*** (2.0, 4.0) | 4.76*** (2.3, 9.9) |
| Financial strain | .43*** (.34, .56) | .24** (.09, .65) | .96 (.76, 1.2) | .63 (.25, 1.6) | .45*** (.38, .54) | .38*** (.26, .56) |
| Unmarried | .97 (.69, 1.4) | 1.18 (.33, 4.3) | .98 (.69, 1.4) | .73 (.22, 2.4) | .99 (.78, 1.27) | 1.61 (.97, 2.7) |
| Lives alone | .95 (.66, 1.3) | 1.54 (.37, 6.3) | .95 (.66, 1.3) | 1.76 (.48, 6.4) | 1.00 (.76, 1.31) | .88 (.49, 1.6) |
| No contact w/family and friends | .89 (.63, 1.3) | .79 (.18, 3.4) | .70 (.48, 1.0) | .67 (.18, 2.6) | 1.28 (.97, 1.70) | 1.18 (.67, 2.1) |
| Social support | .98 (.79, 1.2) | .52 (.22, 1.2) | .98 (.79, 1.2) | .48 (.22, 1.0) | 1.00 (.86, 1.17) | 1.07 (.78, 1.5) |
| Immigrant (1–19) | .88 (.60, 1.3) | .44 (.09, 2.2) | 1.05 (.72, 1.5) | .82 (.19, 3.6) | .84 (.62, 1.13) | .54* (.29, .98) |
| Immigrant (20–49) | 1.76** (1.3, 2.4) | 3.05 (.71, 13.2) | 1.03 (.73, 1.4) | 1.53 (.39, 6.1) | 1.70*** (1.4, 2.1) | 1.99* (1.2, 3.3) |
| Immigrant (50+) | 2.67*** (1.6, 4.4) | 77.26*** (12.4, 481) | 1.01 (.59, 1.7) | 7.26* (1.4, 38.6) | 2.64*** (1.8, 3.7) | 10.64*** (5.1, 22.3) |
| CES-D | .94 (.88, 1.0) | .96 (.91, 1.0) | .98 (.96, 1.0) | |||
| Class 1 vs Class 3, remained non-disabled vs remain disabled | Class 2 vs Class 3, became disabled vs remain disabled | Class 1 vs Class 2, remained non-disabled vs became disabled | ||||
| Model 2 | Model 2 | Model 2 | ||||
| MMSE | 1.00 (.87, 1.1) | .96 (.84, 1.1) | 1.04 (.99, 1.1) | |||
| Smoker | .34 (.07, 1.7) | .43 (.09, 2.0) | .78 (.45, 1.4) | |||
| Drinker | 2.61 (.48, 14.1) | 2.18 (.45, 10.1) | 1.19 (.68, 2.1) | |||
| Obese | .07*** (.02, .20) | .36* (.14, .97) | .19*** (.12, .29) | |||
| Diabetic | 2.01 (.62, 6.5) | 1.18 (.40, 3.5) | 1.70* (1.1, 2.6) | |||
| Hypertensive | .98 (.35, 2.8) | .71 (.27, 1.9) | 1.38 (.92, 2.1) | |||
| History of heart attack | 6.24 (.84, 46.2) | 3.16 (.47, 21.2) | 1.97* (1.05, 3.7) | |||
| History of stroke | 1.35 (.21, 8.5) | 0.91 (.18, 4.5) | 1.48 (.61, 3.6) | |||
| POMA | 159.8*** (90.3, 282) | 11.78*** (7.16, 19.4) | 13.65*** (10.3, 18) | |||
Notes. CES-D = center for epidemiologic studies depression scale ; H-EPESE = Hispanic established populations for the epidemiologic study of the elderly, n = 2,455; HS = high school; MMSE = mini-mental state exam; POMA = performance oriented mobility assessment. The model fit statistics for the three-class solution were as follows: BIC = 50119.55 and LMR-LRT = 88.137 (p < .05).
Shown are odds ratios and 96% confidence intervals (CIs). *p < .05, **p < .01, ***p < .001.
The second model (row 2) adjusts for health behavior, body mass, and health. With these controls the odds of remaining non-disabled versus remaining disabled are lower for obese respondents, but higher for respondents with better physical functioning at baseline. The age effect in model 1 is explained away by differences in baseline physical functioning. With the addition of the health-related covariates in model 2, the odds of becoming disabled versus remaining disabled are now higher for women, indicating a strong distortion pattern or a form of suppression. This means that a third variable, that is, health, changes the direction of the effect of gender on performance.
The second two models (columns 3 and 4) contrast became disabled (class 2) and remained disabled (class 3). In these contrasts the first model reveals that the odds of becoming disabled as opposed to remaining disabled are lower for older adults and respondents with at least a high school education than for younger adults and those with less education. With the addition of health-related covariates in model 2, the odds of becoming disabled versus remaining disabled are higher for women, respondents who immigrated in late-life, and those with higher baseline physical functioning. Significant differences in age and education revealed in the previous model are explained away with the introduction of the health covariates. Gender differences that were suppressed in model 1 reemerge in model 2, suggesting a suppressor effect associated with health.
Columns 5 and 6 contrast remained non-disabled (class 1) and became disabled (class 2). In the first model, the odds of remaining non-disabled versus becoming disabled are lower for older adults, women, and those respondents with higher levels of financial strain. The odds of remaining non-disabled versus becoming disabled are also higher for those with at least a high school education and for those respondents who immigrated in middle- and late-life. Model 2 reveals that the odds of remaining non-disabled versus becoming disabled are lower for obese respondents, but higher for those respondents with a history of heart attack and higher baseline physical functioning. Once again, age differences are explained away and distorted gender differences are revealed.
To summarize, the results reveal three general patterns of decline (a) high initial functioning followed by decline but remaining above our disability cutoff (48% of the sample); (b) moderate initial functioning followed by decline into the range of disability (37.5% of the sample); and (c) poor initial functioning followed by continuing poor functioning (14.5% of the sample). Individuals with the most seriously impaired physical functioning tended to be older, poorly educated, and less financially stable than respondents with better functioning or less decline. Interestingly, most of the health variables are not associated with changes in functioning. The exception is obesity which is known to have important effects on physical functioning, and especially lower body mobility. We suspect that obesity, which is highly significant and correlated with both life style and chronic conditions, overwhelms the impact of the other health predictors. Moreover, the non-statistically significant health behaviors and hypertension are likely to be confounded with certain demographic variables such as age, late-life migration, and initial functioning (Angel, Angel, Díaz-Venegas, & Bonazzo, 2010).
Life Table Analysis
We also estimate of the proportion of life spent with a significant functional limitation relative to the total number of years lived after age 65. These analyses are based on our larger sample that includes the new sample added in 2004 and consists of 3,952 individuals that provide 35,674 person-years of observation. Table 3 presents estimates of life expectancy for women and men at age 65 as well as the average number of years spent with and without significant functional impairment. The first panel refers to women and the second to men. The analysis is stratified by nativity to determine if any detectable immigrant advantages emerge. The first row of Table 3 shows that among women, total life expectancy at age 65 is slightly higher (18.30 years) for the foreign-born than for the U.S.-born (17.76 years), although the difference is not statistically significant. No statistically significant difference in healthy life expectancy (second row) emerge. On the other hand, the foreign born experience a significantly greater number of years with significant functional incapacity than the U.S.-born (11.82 years vs 10.71, respectively). The fourth row presents the ratio of the number of years lived without significant functional incapacity to the total number of years lived, .40 for U.S.-born vs. .35 for the foreign-born.
Table 3.
POMA Life Expectancy at Age 65 by Nativity and Gender 1993–2011
| U.S.-born | Foreign-born | |||
|---|---|---|---|---|
| Years (SE) | 95% CI | Years (SE) | 95% CI | |
| Female | ||||
| Total life expectancy | 17.76 (.35) | 17.10, 18.40 | 18.30 (.40) | 17.56, 19.05 |
| Health life expectancy | 7.04 (.26) | 6.55, 7.56 | 6.48 (.26) | 5.98, 6.99 |
| Unhealthy life expectancy | 10.71 (.25) | 10.25, 11.18 | 11.82 (.36)* | 11.14, 12.53 |
| Ratio of healthy to total | .40 (.01) | .38, .42 | .35 (.01)** | .33, .38 |
| Male | ||||
| Total life expectancy | 14.93 (.32) | 14.28, 15.56 | 16.15 (.49)* | 15.22, 17.07 |
| Health life expectancy | 6.96 (.26) | 6.44, 7.49 | 7.71 (.31) | 7.12, 8.34 |
| Unhealthy life expectancy | 7.96 (.25) | 7.46, 8.45 | 8.44 (.37) | 7.74, 9.19 |
| Ratio of healthy to total | .47 (.01) | .44, .49 | .48 (.01) | .45, .51 |
Notes. CI = confidence interval; POMA = performance-oriented mobility assessment.
*p ≤ .05; **p ≤ .001 significance calculated using z = x 1−x 2/√(se1 2+se2 2)
The patterns for men are similar, although they reflect shorter life spans. The foreign-born have a significant advantage in total life expectancy over the U.S.-born. At age 65, foreign-born men can expect to live an additional 16.15 years compared to 14.93 for the U.S.-born (p < .05). Foreign-born men also have significantly longer lives without functional incapacity. However, when we examine unhealthy life expectancy, there are no statistically significant differences between the foreign born and U.S.-born in terms of time spent with limited physical mobility. Regardless of nativity, men can expect to live over half of their life with limited or no mobility.
Discussion
The objectives of this analysis were (a) to characterize general patterns of decline in functional capacity, and (b) to estimate the proportion of life after 65 in which individuals experience serious incapacity in a longitudinal sample of Mexican-origin adults. In addition to the long follow-up period, a unique aspect of this analysis is the use of an objective, performance-based measure of functional capacity. The analyses suggest great variation in the pace and pattern of decline in objectively measured physical functioning, and they suggest that on average older Mexican-origin individuals spend a large fraction of their lives after 65 with serious impairments. Using growth curve modeling we identified three typical patterns of initial functioning and subsequent decline: (a) high initial functioning followed by stability or moderate decline; (b) moderate initial functioning followed by serious decline; and (c) low initial functioning followed by no change or slight improvement. Clearly, age is a major predictor of low initial functioning and declines over the study period. Results not reported here reveal that older individuals and those with initially low levels of functioning were at elevated risk of death. We were particularly interested in the association of nativity and age at migration on class membership. As in previous research our findings reveal that those who immigrated in mid- or late-life were more likely to be members of the highest functioning category than the U.S.-born or early-life migrants, suggesting that late-life migrants are likely selected for better health.
These data indicate that many older Mexican-origin individuals remain highly functional for a long period, but a large fraction decline seriously or are in poor health from a relatively early age. Those respondents who were 65 at baseline were over 80 by the time of the final follow-up. Those who were older at baseline were even older by the end. Those who were older at baseline were at elevated risk of serious functional decline, dependency, and death. Other factors were also predictive of the extent of functional decline. In bivariate analyses, respondents with less education and lower financial stability were more likely to experience functional decline than those with higher levels of education and financial stability. They also had higher rates of hypertension, stroke, and diabetes at baseline. By definition, those in the highest functioning category had higher physical and cognitive scores than those in the lower functioning categories at baseline.
In the multiple decrement life table analyses we directly estimated the ratio of disability-free years to those with functional impairment by nativity. Those detailed analyses show that the differences in life expectancies between U.S.-born and foreign-born populations are consistent with previous research (Arias, Eschbach, Schauman, Backlund, & Sorlie, 2010; Eschbach, Al-Snih, Markides, & Goodwin, 2007). In this sample, though, Mexican origin elders on average live more than half of their lives after age 65 with significant functional limitations. The data also reveal that gender and nativity interact, such that life expectancy at 65 is highest for foreign-born Mexican-origin women and lowest for U.S.-born males. Regardless of nativity, men spend approximately half of the years after age 65 in an impaired state; foreign-born women live nearly two-thirds of the additional years in a seriously impaired state.
In terms of our motivating question concerning the extent of life past age 65 characterized by significant functional impairment, these data suggest that in this Mexican-origin sample increased longevity is accompanied by the relatively early onset of functional impairment. The data suggest, then, that the postponement of death may occur even in the presence of significant declines in functional capacity. Of course we are dealing with aggregates and a more detailed analysis of individual trajectories of decline would be necessary to more clearly understand intra-group differences in the timing and severity of functional decline.
Our findings have clear policy and practical implications. Individuals who are functionally incapacitated according to the criteria we used are unlikely to be able to care for themselves without some assistance. Most will almost inevitably become entirely dependent on family or the state. For these individuals, Medicaid financed long-term or community care will become a necessity. As states struggle with the burgeoning costs of Medicaid, the growth in the aging population presents local, state, and federal authorities with major challenges. Although the present analysis identifies various factors associated with different patterns of decline in functioning, further research will be required to better understand those at highest risk and to determine how different sources of assistance affect subsequent health and longevity.
Supplementary Material
Supplementary material can be found at: http://psychsocgerontology.oxfordjournals.org/
Funding
This research was supported by the National Institutes of Health , National Institute on Minority Health and Health Disparities (grant 5R01MD-005894-02) and the National Institute of Aging (grant R01-AG10939).
Supplementary Material
Acknowledgments
R. Angel developed the conceptual framework. J. Angel supervised the study and analyses. T. Hill completed the analyses. All authors contributed to the writing and revision of the paper. We would like to thank Marc Garcia and Chi-Tsun Chui for their valuable research assistance.
References
- Angel R. J., Angel J. L., Hill T. D. (2009). Subjective control and health among Mexican-origin elders in Mexico and the United States: structural considerations in comparative research. Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 64B, 390–401. :10.1093/geronb/gbn029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Angel R. J., Angel J. L., Díaz-Venegas C., Bonazzo C. (2010). Shorter stay, longer life: age at migration and mortality among the older Mexican-origin population. Journal of Aging and Health, 22, 914–931. :10.1177/0898264310376540 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arias E., Eschbach K.E., Schauman W. S., Backlund E. L., Sorlie P. D. (2010). The Hispanic mortality advantage and ethnic misclassification on US death certificates. American Journal of Public Health, 100(Suppl 1), S171–S177. :10.2105/AJPH.2008.135863 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown T. H., O’Rand A. M., Adkins D. E. (2012). Race-ethnicity and health trajectories: tests of three hypotheses across multiple groups and health outcomes. Journal of Health and Social Behavior, 53, 359–377. :10.1177/0022146512455333 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cantu P. A., Hayward M. D., Hummer R. A., Chiu C. T. (2013). New estimates of racial/ethnic differences in life expectancy with chronic morbidity and functional loss: evidence from the National Health Interview Survey. Journal of Cross-Cultural Gerontology, 28, 283–297. :10.1007/s10823-013-9206-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen S. B., Yu W. (2012). The concentration and persistence in the level of health expenditures over time: estimates for the U.S. population, 2008–2009 MEPS Statistical Brief (Vol. No. 392.). Rockville, MD: Agency for Healthcare Research and Quality. [Google Scholar]
- Elo I. T. (2009). Social class differentials in health and mortality: Patterns and explanations in comparative perspective Annual Review of Sociology, 35, 553–572. :10.1146/annurev-soc-070308-115929 [Google Scholar]
- Eschbach K., Al-Snih S., Markides K. S., Goodwin J. S. (2007). Disability and Active Life Expectancy of Older U.S.-and Foreign-Born Mexican Americans. In Angel J. L., Whitfield K. E. (Eds.), The health of aging Hispanics: the Mexican-origin population (pp. 40–49). New York, NY: Springer Science. [Google Scholar]
- Faber M. J., Bosscher R. J., van Wieringen P. C. (2006). Clinimetric properties of the performance-oriented mobility assessment. Physical Therapy, 86, 944–954. [PubMed] [Google Scholar]
- Folstein M., Folstein S., McHugh P. (1974). “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research, 12, 189–198. :10.1016/0022-3956(75)90026-6 [DOI] [PubMed] [Google Scholar]
- Freedman V. A., Schoeni R. F., Martin L. G., Cornman J. C. (2007). Chronic conditions and the decline in late-life disability. Demography, 44, 459–477. :10.1007/s13524-012-0167-z [DOI] [PubMed] [Google Scholar]
- Fries J. F. (2003). Measuring and monitoring success in compressing morbidity. Annals of Internal Medicine, 139, 455–459. :10.4061/2011/261702 [DOI] [PubMed] [Google Scholar]
- Guralnik J., Ferrucci L., Simonsick E., Salive M., Wallace R. (1995). Lower-extremity function in persons over the age of 70 years as a predictor of subsequent disability. New England Journal of Medicine, 332, 556–562. :10.1056/NEJM199503023320902 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haan M. N., Zeki Al-Hazzouri A., Aiello A. E. (2011). Life-span socioeconomic trajectory, nativity, and cognitive aging in Mexican Americans: the Sacramento Area Latino Study on Aging. Journals of Gerontology. Series B, Psychological sciences and social sciences, 66B(Suppl 1),i102–i110. :10.1093/geronb/gbq071 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haas S., Rohlfsen L. (2010). Life course determinants of racial and ethnic disparities in functional health trajectories. Social Science & Medicine (1982), 70, 240–250. :10.1016/j.socscimed [DOI] [PubMed] [Google Scholar]
- Haas S. A., Krueger P. M., Rohlfsen L. (2012). Race/Ethnic and Nativity Disparities in Later Life Physical Performance: The Role of Health and Socioeconomic Status Over the Life Course. Journal of Gerontology: Psychological and Social Sciences, 66B, i102–i110. :10.1093/geronb/gbr155 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayward M. D., Hummer R. A., Chiu C.-T., González-González C., Wong R. (2014). Does the Hispanic Paradox in U.S. Adult Mortality Extend to Disability? Population Research and Policy Review, 33, 81–96. do1:10.1007/s11113-013-9312-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayward M. D., Warner D. F., Crimmins E. M. (2007). Does Longer Life Mean Better Health? Not for Native-born Mexican Americans in the Health and Retirement Study. In Whitfield J. L. A. a. K. E. (Ed.), The health of aging Hispanics: the Mexican-origin population (pp. 85–95). New York, NY: Springer Sciences. [Google Scholar]
- Hill T., Angel J., Balistreri K. (2012). Does the Healthy Immigrant Effect Extend to Cognitive Aging?. In Angel J. L., Torres-Gil F., Markides K. (Eds.), Aging, health, and longevity in the Mexican-origin population (pp. 19−–33). New York, NY: Springer Publishing Company. [Google Scholar]
- Hill T., Angel J., Balistreri K., Herrera A. (2012). Immigrant status and cognitive functioning in late-life: an examination of gender variations in the healthy immigrant effect. Social Science & Medicine (1982), 75, 2076–2084. :10.1016/j.socscimed.2012.04.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jagger C, Cox, B, Le Roy S, EHEMU. (2006). Health Expectancy Calculation by the Sullivan Method. Third Edition. EHEMU Technical Report. pp. 5–37. France: EHEMU. [Google Scholar]
- Jung T., Wickrama A. (2008). An introduction to latent class growth analysis and growth mixture modeling. Social and Personality Psychology Compass, 2, 302–317. :10.1111/j.1751-9004.2007.00054.x [Google Scholar]
- Link B. G., Phelan J. (1995). Social conditions as fundamental causes of disease. Journal of Health and Social Behavior, 35, 80–94. :10.1177/0022146510383498 [PubMed] [Google Scholar]
- Markides K. S., Black S. A., Ostir G. V., Angel R. J., Guralnik J. M., Lichtenstein M. (2001). Lower body function and mortality in Mexican American elderly people. Journals of Gerontology. Series A, Biological sciences and Medical Sciences, 56, M243–M247. :10.1093/gerona/56.4.M243 [DOI] [PubMed] [Google Scholar]
- Markides K. S., Eschbach K. (2005). Aging, migration, and mortality: current status of research on the Hispanic paradox. Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 60, S68–S75. :10.1093/geronb/60.Special_Issue_2.S68 [DOI] [PubMed] [Google Scholar]
- Markides K. S., Rudkin L., Angel R. J., Espino D. (1997). Health Status of Hispanic Elderly. In Martin L. G., Soldo B. J. (Eds.), Racial and ethnic differences in the health of older Americans (pp. 285–300) Washington, DC: National Academy Press. [Google Scholar]
- National Center for Health Statistics. (2014). Life expectancy at birth, at age 65, and at age 75, by sex, race, and Hispanic origin: United States, selected years 1900–2010. Health, United States, 2013: With special feature on prescription drugs. Hyattsville, MD: National Center for Health Statistics. [PubMed] [Google Scholar]
- Palloni A. (2007). Health Status of Elderly Hispanics in the United States. In Angel J. L., Whitfield K. E. (Eds.), The health of aging Hispanics: The Mexican-origin population (pp. 1–14). New York, NY: Springer. [Google Scholar]
- Quiñones A. R., Liang J., Bennett J. M., Xu X., Ye W. (2011). How does the trajectory of multimorbidity vary across Black, White, and Mexican Americans in middle and old age? Journals of Gerontology. Series B, Psychological sciences and social sciences, 66B, 739–749. :10.1093/geronb/gbr106 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Radloff L. S. (1977). The CES-D scale: a self-report depression scale for research in the general population. Journal of Applied Psychological Measurement, 1, 385–401. :10.1177/014662167700100306 [Google Scholar]
- Ram N., Grimm K. (2009). Growth Mixture Modeling: a method for identifying differences in longitudinal change among unobserved groups. International Journal of Behavioral Development, 33, 565–576. :10.1177/0165025409343765 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sullivan D. F. (1971). A single index of mortality and morbidity. HSMHA Health Reports, 86, 347–354. [PMC free article] [PubMed] [Google Scholar]
- Taylor M. G., Lynch S. M. (2004). Trajectories of impairment, social support, and depressive symptoms in later life. Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 59, S238–S246. :10.1093/geronb/59.4.S238 [DOI] [PubMed] [Google Scholar]
- United Nations. (2011). World mortality report 2007. New York, NY: United Nations, Department of Economic and Social Affairs, Population Division; Retrived February 5, 2010, from http://www.un.org/esa/population/publications/worldmortalityreport2007/WORLD%20MORTALITY%20REPORT.PDF. [Google Scholar]
- Werner C. A. (2011). The older population: 2010. 2010 census briefs C2010BR-09 (pp. 1–19), Washington, DC: Census Bureau. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.