

Abstract
Study Objectives:
Sleep disturbance is among the most common complaints of veterans and military personnel who deployed to the conflicts in Iraq and Afghanistan. A growing body of research has examined cross-sectional and longitudinal relationships between sleep disturbance and mental health symptoms and specific diagnoses in this population. However, prior research has not examined these relationships in terms of the presence or absence of any mental health diagnosis. The objective of the current study is to characterize the sleep complaints (sleep characteristics, sleep quality, insomnia symptoms, and distressing dreams and nightmares) of previously deployed military personnel in terms of the presence or absence of a mental health disorder, diagnosed using structured clinical diagnostic interviews.
Methods:
Participants (n = 1,238) were veterans and active duty military personnel serving in the military since September 11, 2001, and deployed at least once. Scale scores and item-level data from the Pittsburgh Sleep Quality Index (PSQI), the PSQI-Addendum, the Davidson Trauma Scale, and the Symptom Checklist-90 were used to compare sleep across mental health status (with/without mental health disorder).
Results:
As expected, self-reported sleep impairments were worse among those meeting criteria for a mental health disorder. However, findings also revealed very poor sleep among those without a mental health diagnosis as well. Mean values for both groups were suggestive of short sleep duration, low sleep efficiency, long sleep onset latencies, poor sleep quality, frequent insomnia symptoms, and nightmare frequencies that are well above norms for the general population.
Conclusions:
Given the evidence for adverse mental and physical health sequelae of untreated sleep disturbance, increased attention to sleep in this population may serve as a primary prevention strategy.
Citation:
Ulmer CS, Van Voorhees E, Germain AE, Voils CI, Beckham JC; VA Mid-Atlantic Mental Illness Research Education and Clinical Center Registry Workgroup. A comparison of sleep difficulties among Iraq/Afghanistan theater veterans with and without mental health diagnoses. J Clin Sleep Med 2015;11(9):995–1005.
Keywords: sleep, veterans, prevention, mental health disorders
Sleep disturbance is among the most common complaints of military service personnel and veterans who have served in the Iraq and Afghanistan conflicts (hereinafter IA veterans), and those who deployed to these conflicts are significantly more likely to report difficulty sleeping than those who did not deploy.1 In a post-deployment survey of IA veterans, 64% of respondents reported new onset of difficulties falling asleep and staying asleep following deployment relative to their pre-deployment sleep.2 Objective evidence (polysomnography) in IA veterans revealed high rates of sleep apnea and short sleep duration, high rates of insomnia endorsement, and frequent comorbidity with medical and mental health conditions.3
BRIEF SUMMARY
Current Knowledge/Study Rationale: Prior research has focused on relationships between sleep and mental health symptoms in previously deployed veterans and military personnel. However, little research has examined sleep in terms of the presence or absence of a mental health disorder, diagnosed using structured clinical diagnostic interviews.
Study Impact: This is the first study, to our knowledge, to reveal significantly impaired sleep among previously deployed veterans and military personnel who are known to not meet diagnostic criteria for a mental health disorder. Since prospective research suggests that sleep disturbance precedes the development of certain psychiatric disorders and health conditions, and that sleep disturbance may play a role in suicidality, improving sleep in this population may be an opportunity for primary prevention.
The majority of sleep-related research in IA veterans has focused on the relevance of trauma exposure, posttraumatic stress symptoms, and posttraumatic stress disorder (PTSD) in sleep disturbance. Approximately 21% of veterans using Veterans Affairs (VA) services meet criteria for PTSD,4 and up to 90% of these are likely to endorse insomnia symptoms as well.5,6 A range of PTSD symptoms are associated with sleep disturbance, and recent research suggests that PTSD symptoms and sleep-specific complaints may cluster in a predictable pattern.7,8 Individuals with PTSD commonly report the following sleep difficulties: difficulty initiating sleep, difficulty maintaining sleep, early morning awakenings, nonrestorative sleep, sleep paralysis, sleep talking, nightmares, violent or dangerous behaviors during sleep, hypnagogic hallucinations, and hypnopompic hallucinations.6 In fact, based on their review of the literature on polysomnographic and self-reported findings among trauma survivors, Mysliwiec and colleagues recently proposed a new parasomnia disorder, “Trauma Associated Sleep Disorder,” that is characterized by this commonly reported/observed cluster of symptoms among trauma survivors.9
Sleep disturbance is a common complaint among those suffering from both acute and chronic mood disorders as well.10 Approximately 17% of veterans using VA services are diagnosed with depression,4 and in light of the comorbidity between insomnia and mood disorders,11 a significant portion of these veterans are likely to have a comorbid insomnia as well. Insomnia is predictive of the development and recurrence of mood disorders, and is associated with the severity of psychiatric conditions.10 A growing body of prospective research suggests that sleep problems may precede the development of psychiatric disorders: a meta-analysis of longitudinal studies indicated that individuals with insomnia were more than twice as likely as those without insomnia to develop depression.12 In the Millennium Cohort, a sample of military personnel serving since 9/11, pre-deployment short sleep duration and insomnia symptoms were predictive of new-onset post-deployment PTSD, anxiety and depression.13 Sleep problems have also been found to predict suicide in several studies.14,15 In veterans, sleep disturbances explained 57% of the variance in time-to-suicide in suicide completers even after adjusting for psychiatric and substance abuse symptoms.15
The literature reviewed above reflects an awareness of the importance of addressing the sleep complaints of veterans diagnosed with certain mental health disorders, such as PTSD,16–18 but largely absent from the literature is a comparison of the sleep characteristics/complaints of veterans deployed to Iraq and Afghanistan who do not meet diagnostic criteria for a mental health disorder relative to those do. Though sleep disturbance is strongly associated with PTSD and depression diagnoses in IA veterans,1,19,20 sleep problems are also common among veterans without mental health conditions as well. In the 2009 Behavioral Risk Factor Surveillance System,21 more than 90% of veterans reported fewer than 14 days of mental health symptoms in the past month. Nevertheless, this veteran subgroup was more likely to endorse insufficient rest or sleep and short sleep duration than non-veterans. This finding remained significant after adjusting for mental health symptoms, and suggests that many IA veterans are suffering disturbed sleep even in the absence of comorbid mental health conditions. However, additional research employing mental health diagnoses, rather than symptoms, is needed to confirm this likelihood.
Recognizing and treating sleep difficulties in veterans may not only relieve the distress of the attendant sleep symptoms, but might also impede the development or progression of health-related comorbidities. In community-based research, short sleep duration and insomnia symptoms have been found to convey considerable health risks. Short sleep duration is predictive of cardiovascular disease (CVD) and stroke,22–24 increased risk of obesity,25 metabolic syndrome,26 type 2 diabetes mellitus,27 and all-cause mortality.28 The risk of hypertension in those having the combination of insomnia and short sleep duration ranges from three to five times that of normal sleepers depending on sleep duration.29 In IA military service members, combat deployment was associated with new-onset coronary heart disease following deployment,30 and deployed IA veterans were found to have significantly shorter sleep and increased odds of reporting trouble sleep relative to those who did not deploy.1,31
Given the focus on associations between sleep and symptoms of specific mental health disorders in prior research, the objective of the current study was to compare and contrast the sleep complaints of previously deployed IA veterans in terms of the presence or absence of mental health disorders diagnosed using clinician-administered structured interviews. To accomplish this objective, we compared self-reported sleep quality and sleep characteristics by mental health diagnostic status in a sample of veterans and active duty military personnel who deployed to Iraq or Afghanistan at least once, and served in the military since September 2001. Exploratory analyses were used to examine how those with and without a mental health diagnosis compared on:
Sleep characteristics;
Sleep quality;
Insomnia symptoms;
Distressing dreams and nightmares.
We expected those with a mental health disorder to endorse significantly poorer sleep across all of these measures. However, in the absence of prior research using mental health diagnostic status, we could not hypothesize about the degree of impaired sleep in IA veterans without a mental hea1th diagnosis. A detailed characterization of sleep complaints in this burgeoning population will inform our efforts to increase access to behavioral sleep medicine, and may also inform our treatment approach in this population.
METHODS
Participants and Recruitment
This study was part of a multi-site investigation conducted through the Department of Veterans Affairs VISN 6 Mid-Atlantic Mental Illness Research, Education, and Clinical Center (MIRECC). Participants were recruited from 1 of 4 VISN-6 Veterans Affairs medical centers (Durham, NC; Salisbury, NC; Richmond, VA; and Hampton, VA) through mailings, advertisements, and provider referrals. Approvals were obtained from each of the institutional review boards serving the 4 VA medical centers from which participants were enrolled. Eligible participants were individuals who served in the U.S. military after September 11, 2001. Recruitment letters used 1 of 2 wording options to invite participants to participate. Specifically, the letters stated that the study focused on “the effects of recent military deployments on the mood, emotions, and mental and physical health of military personnel” or “the effects of recent deployments on the physical and mental health of service members, especially as they transition from deployment back to civilian life.” Participants were paid $175 for completing a structured clinical interview in addition to a battery of questionnaires addressing a range of possible post-deployment adjustment problems. This ongoing project enrolled more than 3,000 veterans between June 2005 and August 2014. In the current study, data were available for 2,166 individuals participating in the study between 2005 and 2012.
Procedures
Participants underwent a full-day assessment at a research laboratory located at 1 of 4 VA hospitals. Informed consent was obtained, and participants completed a range of self-report measures on a computer examining mood, trauma exposure, mental health, and physical health ; participated in a structured clinical interview; and provided body measurements (height, weight) and blood samples for metabolomics and genetic analysis. At the end of the study day, participants were provided feedback regarding any potential diagnoses suggested by the structured clinical interview and options for further evaluation and follow-up treatment were discussed. If the clinician who conducted the interview was not a licensed clinician, the supervising licensed clinical psychologist participated in the formulation and/or presentation of the feedback. A subset of the self-report measures completed as part of this larger study was analyzed for this investigation.
Measures
Demographics Questionnaire: Participants provided demographic and military service information, including the number of tours and military status (active duty versus discharged).
Independent Variable
AXIS I Mental Health Disorder/s
The Structured Clinical Interview for DSM-IV Axis-I Disorders (SCID-I)32: The SCID-I was used to assess for the presence of all Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) Axis I psychiatric diagnoses, with the exception of childhood onset disorders, sexual disorders, sleep disorders, and dementias. Trained interviewers were licensed doctoral-level clinical psychologists, or were supervised by licensed clinical psychologists. The mean inter-rater reliability among interviewers was excellent for all for Axis I diagnoses (Fleiss κ = 0.96), including for current PTSD (Fleiss κ = 1.0). For purposes of these analyses, study participants were coded as positive for a mental health diagnosis if they met DSM-IV diagnostic criteria for any Axis I mental health condition.
Outcome Variables
Sleep Characteristics and Sleep Quality
The Pittsburgh Sleep Quality Index (PSQI)33: The PSQI was used to assess sleep quality over the past month. This self-report questionnaire is widely used in clinical sleep research, and is reliable across a range of medical and psychiatric populations (Cronbach α 0.80 and 0.83, respectively).33,34 The PSQI yields both subscale and a global score of sleep quality, ranging from 0 to 21. PSQI subscales include the following: sleep duration, sleep disturbances, sleep onset latency, daytime dysfunction due to sleepiness, habitual sleep efficiency, overall sleep quality, and need for sleep medications. A cutoff score of 5 for the total score has been found to be sensitive and specific in identifying individuals with sleep problems.33 In the current study, sleep duration, sleep onset latency, sleep efficiency percentage, and time in bed were derived from PSQI items 1–4. Sleep quality was derived from PSQI total and subscale scores.
The PSQI-Addendum (PSQI-A)7: The PSQI-A was used to assess sleep quality related to trauma exposure over the past month. The PSQI-A is a 7-item self-report measure designed to capture the unique sleep presentation of those having trauma exposure and/or symptoms of PTSD. The psychometric properties of the PSQI-A were established in a sample of women presenting for both clinical and research purposes with and without PTSD. The PSQI-A was shown to have satisfactory internal consistency (Cronbach α = 0.85), good convergence with the Clinician-Administered PTSD Scale (r = 0.51, p < 0.001) and the Perceived Stress Scale (r = 0.49, p < 0.001) after removing sleep items, and a score ≥ 4 had a positive predictive value of 93% for PTSD. The PSQI-A was also recently validated and found to have acceptable psychometric properties in a sample of sample military veterans.35
In the current study, trauma-related sleep quality was assessed using the PSQI-A total score. Respondents were asked “During the past month, how often have you had trouble sleeping because you…” Respondents were then asked to rate the frequency of 7 disruptive nocturnal behaviors, including: hot flashes, nervousness; nightmares of trauma, other nightmares, panic, night terrors, and acting out dreams. Response options for these items were: not during the past month, less than once a week, once or twice a week, or ≥ 3 times a week.
Insomnia Symptoms
The Symptom Checklist (SCL-90-R)36: The SCL-90-R was used to assess insomnia symptoms over the past week. The SCL-90-R is a commonly employed measure in medical research, and has well-established validity and reliability. It assesses a broad range of mental health symptoms including somatization, obsessions/compulsion, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism. The SCL-90-R is a self-report measure of mental health symptoms rated on a 5-point scale. On the SCL-90-R, respondents are provided with a list of mental health symptoms (e.g., feeling easily annoyed or irritated) and asked to select the response that best describes, “How much that problem has distressed or bothered you during the past 7 days, including today.” The response set is comprised of the following: not at all, a little bit, moderately, quite a bit, and extremely. In the current study, insomnia symptoms were evaluated using 3 sleep-related SCL-90-R items, as follows: trouble falling asleep, awakening early in the morning, sleep that is restless or disturbed.
Davidson Trauma Scale (DTS)37: Since the DTS insomnia item is worded to capture both sleep onset and maintenance issues, it was used as an additional measure of insomnia symptoms over the past week. The DTS is a 17-item self-report measure of the frequency and severity of symptoms of post-traumatic stress disorder (PTSD) experienced within the past week. The scale yields a total PTSD score, as well as scores for each of the 3 symptom clusters of PTSD as described in the DSM-IV-TR: re-experiencing, avoidance, and hyperarousal. This measure has demonstrated acceptable reliability and validity in samples of Operation Enduring Freedom/Operation Iraqi Freedom veterans.38 A total score cutoff value of 64 has been found to have good sensitivity (0.86) and specificity (0.70)39 for predicting a diagnosis of PTSD based on structured clinical interview.
On the DTS, respondents are first asked to briefly describe the traumatic experience that is most troubling to them. They are then asked, “In the past week, how much trouble you have had with the following symptoms?” In the current study, the following insomnia symptom DTS item was used in analyses: Have you had trouble falling asleep or staying asleep? The respondents used the following response sets to indicate the frequency (not at all, once only, 2–3 times, 4–6 times, and every day) and severity (not at all distressing, minimally distressing, moderately distressing, markedly distressing, and extremely distressing) of this symptom over the previous week.
Distressing Dreams and Nightmares
A single item from the DTS (described above), was used to assess the frequency and severity of distressing dreams over the past week, as follows: “Have you had distressing dreams of the event?” The respondent was offered the same frequency and severity response sets described above.
A single item from the PSQI-A was used to assess nightmare frequency: “During the past month, how often have you had trouble sleeping because you had memories or nightmares of a traumatic experience?” Response options for this item included: not during the past month, less than once a week, once or twice a week, or ≥ 3 times a week.
Analytic Approach
As noted above, data were available in these analyses for 2,166 individuals participating in the study between 2005 and 2012. Participants who did not deploy (or for whom deployment data were missing) were excluded from the dataset, leaving 1,872 participants who deployed at least once. Data from the PSQI were cleaned to exclude outliers (n = 589 cases which could be included in more than one of the following descriptions: sleep onset latency > 3 h, total sleep time > 12 h, and/or those for whom time in bed was less than total sleep time) for a final N of 1,283 available for these analyses. Outliers removed from the base file did not differ from the final sample in terms of age, gender, depression symptoms (BDI-II score), PTSD symptoms (DTS score), or general mental health symptoms (SCL score). Analysis of variance (ANOVA) was used to compare participants with (hereinafter MH+) and without (hereinafter MH−) a mental health diagnosis on continuous demographic/military variables (e.g., age, tours of duty). Those found to differ significantly were used as covariates in subsequent ANCOVA analyses. Additional analyses were conducted to answer the following specific research questions.
To examine how MH+ and MH− compared on key self-reported sleep characteristics, groups were compared using ANCOVA on the following variables which were derived from individual PSQI items: time in bed, sleep onset latency, sleep efficiency, and total sleep time.
To examine how MH+ and MH− compared on sleep quality, groups were compared using ANCOVA on PSQI total and subscale scores in addition to the PSQI-A total score.
To examine how MH+ and MH− compared on insomnia symptoms, individual items on these topics were selected from the DTS and the SCL. The following insomnia symptoms were examined: “difficulty falling asleep or staying asleep,” “trouble falling asleep,” “sleep that is restless or disturbed,” and “awaking early in the morning.” Chi-square analyses were conducted to compare groups across categorical responses, and bar graphs were used to depict differences in the frequency and severity of each insomnia symptom.
Finally, to examine how MH+ and MH− compared on distressing dreams and nightmares, individual items on these topics were selected from the DTS and PSQI-A. Chi-square analyses were conducted to compare groups across categorical responses, and bar graphs were used to depict differences in the frequency and severity of distressing dreams/nightmares and disruptive nocturnal behaviors.
RESULTS
Demographic and military service characteristics of the sample are summarized in Table 1. As shown, participants in this sample were about 37 years of age, mostly male (81.4%), about half married (49.1%), about half of minority race (49.3%), and only about 5% active duty (5.4%). The MH+ group was younger (p < 0.001), more likely to be male (p < 0.05), and less likely to be active duty (p = 0.02). Table 2 is a summary of mental health diagnosis frequencies in the MH+ group. Compared to statistics cited in a 2013 report by the Institute of Medicine40 on the demographic characteristics of military personnel serving in the Iraq and Afghanistan conflicts, our sample is about the same age, and is composed of about 25% more racial minorities, about 19% more female deployers, and about 9% fewer married individuals than the population of individuals who have served in these conflict eras.
Table 1.
Comparing demographic characteristics of those with and without a mental health diagnosis.
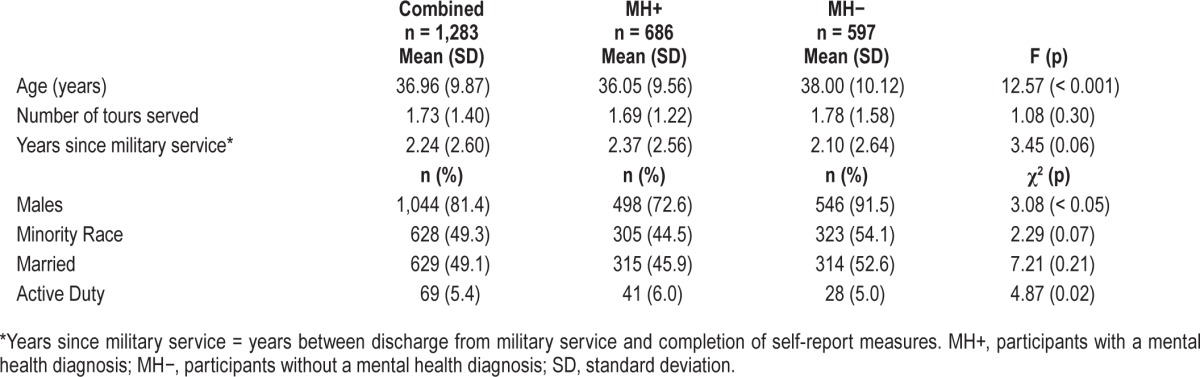
Table 2.
Mental health diagnosis frequencies for MH+ group.
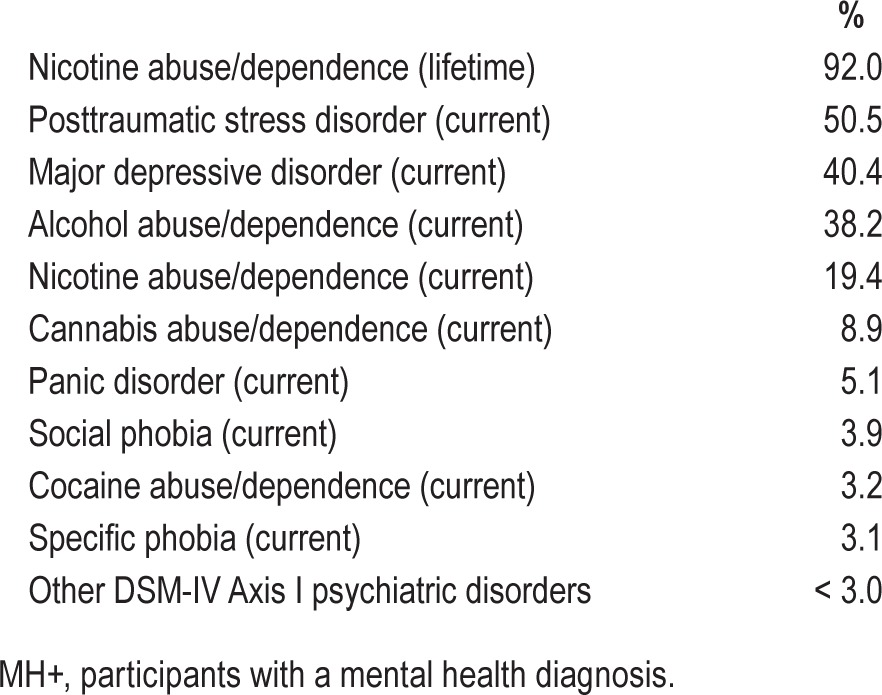
Table 3 is a comparison of MH+ and MH− on time in bed, total sleep time, sleep efficiency, and sleep onset latency. As indicated, means for these variables were adjusted for age, sex, and race. The average sleep duration, sleep efficiency and sleep onset latency of this sample was 5.40 h, 71.31%, and 36.10 min, respectively. The MH+ group reported shorter total sleep time (p < 0.001) and lower sleep efficiency (p < 0.001). Groups did not differ on sleep onset latency or time in bed.
Table 3.
Comparison of self-reported sleep characteristics by mental health diagnostic status.
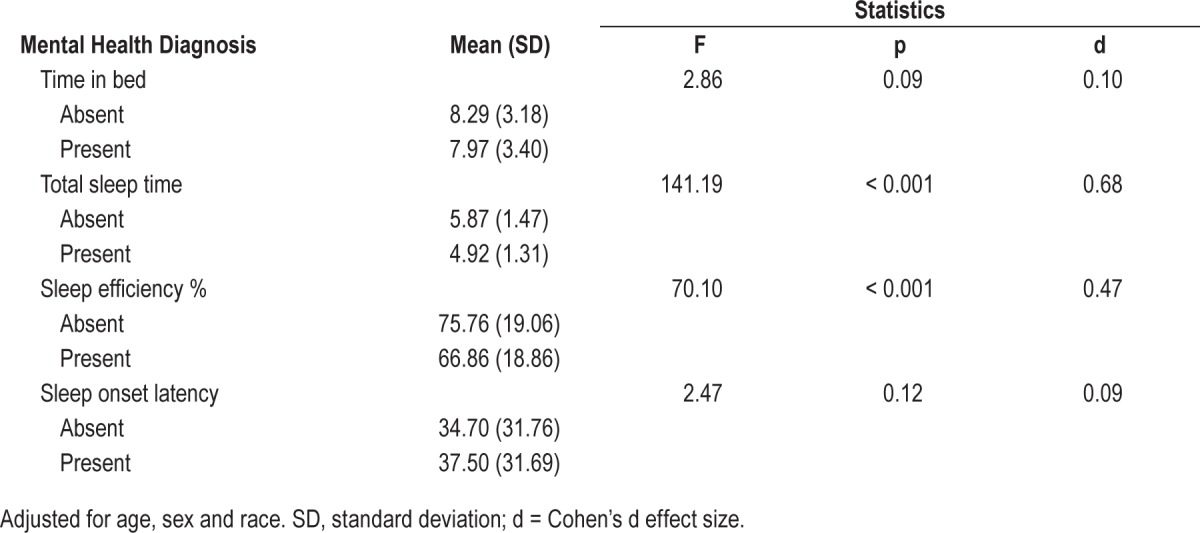
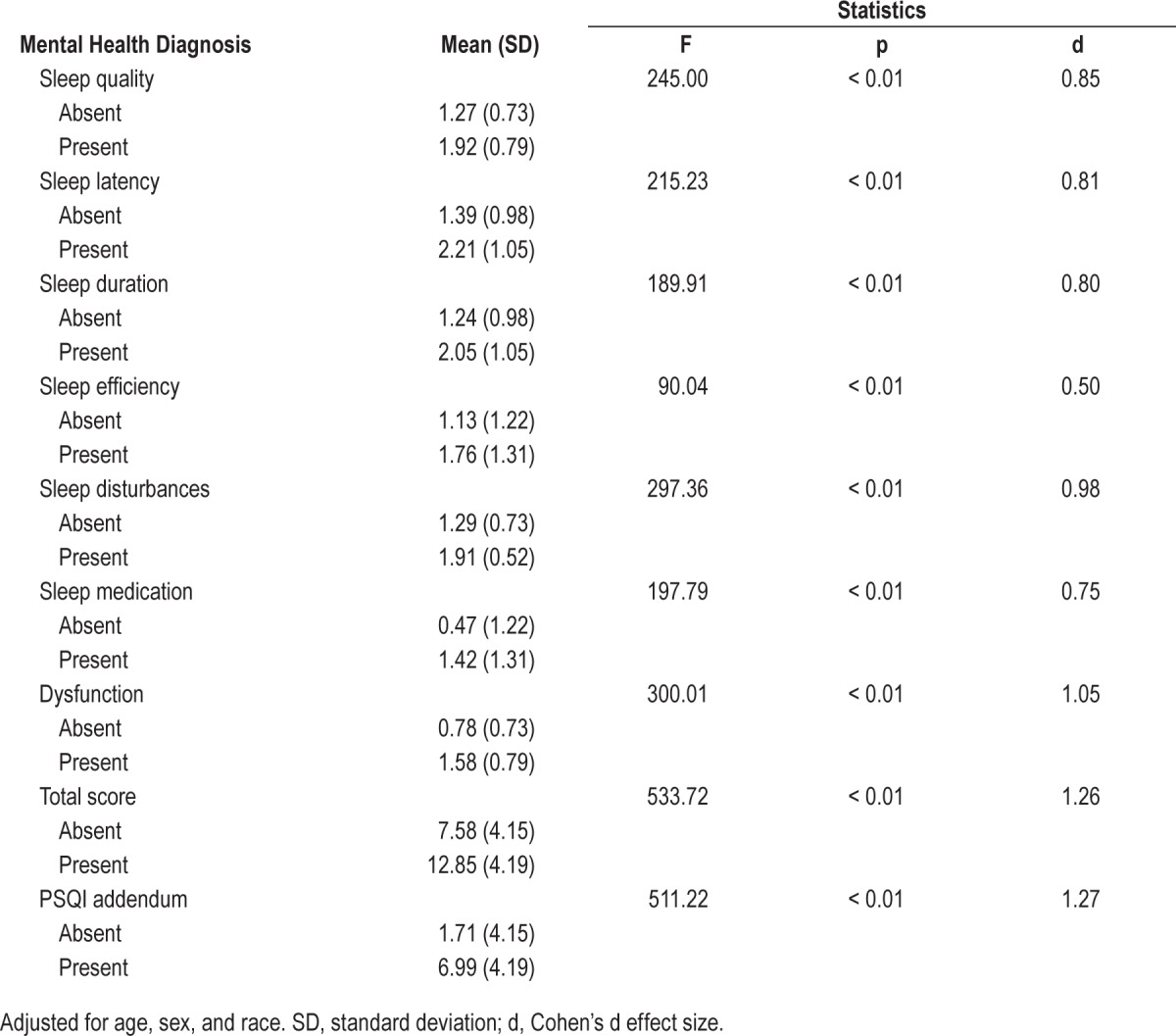
Table 4 is a comparison of MH+ and MH− on PSQI total score, PSQI subscale scores, and PSQI-A total score, adjusted for age, sex, and race. Unsurprisingly, the MH+ group reported greater pathology across all PSQI scales, with dysfunction, sleep disturbances, and sleep quality being the most disparate PSQI subscale scores between groups. Of note, the sleep onset latency subscale is calculated using both the sleep onset latency item response (Question 2 above) plus the frequency of being unable to fall asleep within 30 minutes (Question 5a). Thus, the categorization process for the sleep onset latency subscale explains the discrepancy between self-reported sleep onset latency and the sleep onset latency subscale (Table 4). Interestingly, although groups differ on PSQI total score, the mean score for the MH− group was above the PSQI cutoff score of 5, suggesting poor sleep quality. In fact, 71% of the MH− group had a PSQI total score > 5. Examination of the distribution of PSQI total scores in the MH− group revealed a bimodal distribution, with modes at scores of 4 and 10, suggesting that this group includes individuals without clinically significant sleep complaints as well as individuals with scores well above the cutoff score of 5. Also as expected, the MH+ groups endorsed considerably more disruptive nocturnal behaviors and poorer trauma-related sleep quality than the MH− group.
Table 4.
Comparison of PSQI subscale and total scores by mental health diagnostic status.
Figures 1A through 1E display the categorical responses to questions about the frequency and severity of insomnia symptoms. As seen in Figure 1A, more than 80% (81.5%) of the MH+ group had difficulty falling asleep or staying asleep ≥ 2–3 times per week, as compared to almost 40% (39.7%) of those in the MH− group. About three-quarters (75.6%) of the MH+ group rated their distress about difficulties with sleep onset or maintenance as “moderate” or greater, as compared to about one-quarter (27.8%) of the MH− group (Figure 1B). About three-quarters (73.3%) of the MH+ group rated their distress level about trouble falling asleep over the past 7 days as “moderate” or greater, as compared to about one-quarter (26.8%) of the MH− group (Figure 1C). As seen in Figure 1D, about three-quarters (75.9%) of the MH+ group rated their distress about sleep that is restless or disturbed as “moderate” or greater, as compared to 28.8% of the MH− group. As seen in Figure 1E, 60.30% of the MH+ group rated their distress about awaking early in the morning as “moderate” or greater, as compared with 22.7% of the MH− group. Chi-square analysis findings are shown on each figure and indicate significantly greater frequency and severity across all of these items in the MH+ group.
Figure 1.

(A) DTS Item: Trouble Falling Asleep or Staying Asleep (Frequency). (B) DTS Item: Trouble Falling Asleep or Staying Asleep (Severity). (C) SCL Item: Trouble Falling Asleep. (D) SCL Item: Sleep that is Restless or Disturbed. (E) SCL Item: Awaking Early in the Morning.
Figures 2A through 2C display categorical responses about the frequency and severity of distressing dreams and frequency of nightmares. As seen in Figure 2A, about 66% of the MH+ group endorsed “distressing dreams of a traumatic event” at a frequency of at least once per week, as compared to 26% of the MH− group. More than half (58.4%) of the MH+ group rated distressing dreams to be “moderately distressing” or greater, as compared to 16.6% of the MH− group (Figure 2B). About 54% of the MH+ group endorsed trouble sleeping because of “memories or nightmares of a traumatic experience” at a frequency of at least once per week, as compared to about 10% of the MH− group (Figure 2C). Chi-square analysis findings are shown on each figure and indicate significantly greater frequency and severity across all of these items in the MH+ group.
Figure 2.

(A) DTS Item: Distressing Dreams of a Traumatic Event (Frequency). (B) DTS Item: Distressing Dreams of a Traumatic Event (Severity). (C) PSQI Addendum Item: During the past month, how often have you had trouble sleeping because you had memories or nightmares of a traumatic experience?
DISCUSSION
In the current study, we examined the self-reported sleep characteristics, sleep quality, disturbing dreams and nightmares, and insomnia complaints in a sample of previously deployed IA veterans and military personnel with and without a mental health diagnosis. Our finding of poor sleep in IA veterans with a mental health disorder is unsurprising and is consistent with the literature reviewed above. To our knowledge, however, our study is the first to reveal significantly impaired sleep among IA veterans known to not meet diagnostic criteria for a mental health disorder.
Sleep Characteristics
As expected, MH+ IA veterans reported shorter sleep duration and lower sleep efficiency than MH− IA veterans. However, groups did not differ on self-reported minutes to fall asleep or time in bed over the past month. The average sleep onset latency in both groups exceeded 30 minutes; a frequently cited guideline for “normal” sleep onset latency.41,42 In light of the higher rates of insomnia symptoms in MH+ individuals, the failure to find a difference in sleep onset latency between groups is unexpected. Although there was a trend towards MH− individuals spending more time in bed, groups did not differ significantly on typical time in bed over the past month.
When examining groups separately, we found that MH− IA veterans had considerably poorer sleep characteristics than a comparable young adult sample used to validate the PSQI.43 Whereas the PSQI validation sample reported a sleep latency of 16.20 minutes (diary), a sleep efficiency of 94.32% (diary), and a total sleep time of 7.22 hours; MH− IA veterans in the current research reported a sleep latency of 34.70 minutes; sleep efficiency of 75.76%; and total sleep time of 5.87 hours. Another noteworthy finding is that self-reported sleep onset latency and sleep efficiency percentage in MH− IA veterans exceeded the frequently cited guidelines for “normal” sleep of 30 minutes and 85%, respectively.41
The finding of 5.87 hours of self-reported sleep duration in the MH− group is in line with the 5.8 hours reported for a sample of IA veterans who had recently returned from deployment,44 but is considerably lower than the 6.5 hours reported for the Millennium Cohort sample.1,13 This discrepancy could be explained by the fact that the Millennium Cohort findings were adjusted for baseline mental health symptoms, whereas the findings of Luxton and colleagues were not. The discrepancy might also be explained by differences in sample characteristics, such as military service branch or demographic characteristics. On the whole, however, the collective findings of these studies suggest that sleep duration among veterans and military personnel are shorter than the US general population,45,46 regardless of mental health diagnostic status.
Sleep Quality
As expected and consistent with prior research,17,47,48 we found that MH+ veterans had higher PSQI and PSQI-A scores (including both total and subscale scores) than MH− IA veterans. However, we also found poor sleep quality in MH− IA veterans on average. Not only was the average global PSQI score in the MH− group (7.58) above the cutoff of 5 for normal sleep quality,33 but more than two-thirds of MH− IA veterans exceeded this cutoff. This finding is not consistent with the global PSQI score for the young adult validation sample (4.07) discussed above,43 suggesting that IA veterans without a mental health diagnosis have poorer sleep quality than community-dwelling young adults. Although scores for trauma-related sleep quality were similarly disparate across groups (Cohen's d = 1.27) as overall sleep quality, MH− IA veterans scored (M = 1.71, SD = 4.15) well below the cutoff of 4, whereas MH+ IA veterans scored considerably higher than the cutoff score (M = 6.99, SD = 4.19).
Insomnia Symptoms
As expected, the MH+ group endorsed significantly more difficulties falling asleep, staying asleep, and waking too early. About two-thirds (65.0%) of MH+ IA veterans endorsed “trouble falling asleep or staying asleep” ≥ 4 days per week, and three-quarters (75.6%) endorsed “moderate” or greater distress about these difficulties. These findings are consistent with those of the Millennium Cohort,1 wherein deployers endorsing mental health symptoms (above defined criterion values) had increased odds of “trouble falling asleep or staying asleep” over the past month. Insomnia symptoms in our MH− group were elevated as well. About 20% (21.10%) of MH− IA veterans endorsed “trouble falling asleep or staying asleep” ≥ 4 days per week, and 27.80% endorsed “moderate” or greater distress about these difficulties.
Although groups did not differ in terms of sleep onset latency, as discussed above, they differed significantly on the severity of “trouble falling asleep,” as depicted in Figure 1B. Perhaps this discrepancy is explained by differences in perceptions about “trouble falling asleep.” Whereas the sleep onset latency item of the PSQI elicits the typical number of minutes it takes to fall asleep, the “trouble falling asleep” item elicits the respondent's perception of sleep onset difficulties. Indeed, prior research has demonstrated differences between insomniacs and normal sleepers on their perceptions of sleep onset and awakenings.49
The endorsement ratios (MH+/MH−) for “trouble falling asleep” (Figure 1C) and “sleep that is restless and disturbed” (Figure 1D) is roughly 75/25 for both items. As would be expected, the endorsement rates were slightly higher when participants were asked about “trouble falling asleep or staying asleep” within a single item, since participants could endorse this item if they had only one of these issues, or both. Interestingly, the endorsement rate for “awakening too early” was about 14% lower (than 75%) in the MH+ group, but only about 4% lower (than 25%) in the MH− group. It may be that “awakening too early” implies that one has slept without disruption until early in the morning, whereas the highly fragmented sleep of IA veterans is better reflected by the “sleep that is restless or disturbed” item.
Distressing Dreams and Nightmares
As expected, the MH+ group endorsed considerably higher nightmare frequency. We found that 54.1% of MH+ participants and 10.1% of MH− participants endorsed memories or nightmares of a traumatic event at a frequency of at least “once or twice” per week. These findings are generally consistent with those of Pigeon and colleagues50 wherein 61% of IA veterans endorsed being at least “moderately bothered” by nightmares in the past month. In contrast, the prevalence of nightmares in US adults is estimated between 2% to 8%.42 In a recent study of the Finnish general adult population (n = 69,813) respondents were asked, “During the past 30 days, have you had nightmares…often, sometimes, or never?” After removing the war generation, they found a 30-day prevalence of frequent (“often”) nightmares in 2.9% of men and in 4.4% of women.51 Thus, when considered in light of the prevalence in civilian samples, nightmare prevalence in MH− IA veterans appears to be considerably higher than the general population. Respondents were also asked about distressing dreams in the current study, and rates of endorsement for this item were comparable to rates for nightmares. More than half (52.4%) of MH+ veterans endorsed distressing dreams at a frequency of at least 2 to 3 per week, as compared to 13.2% of MH− veterans. Thus, the endorsement rate for distressing dreams appears to be somewhat less than nightmares in the MH+ group, and somewhat more than nightmares in the MH− group.
Summary
Our findings are consistent with other studies of impaired sleep in veterans and military personnel of the Iraq and Afghanistan conflicts. We found high levels of impaired sleep in the group as a whole, and even greater sleep impairment among those with a mental health diagnosis. A novel finding emerging from this research is that IA veterans and military personnel who do not meet criteria for a mental health disorder appear to have subjectively shorter sleep duration, poorer sleep quality, and more frequent/more severe insomnia, distressing dreams and nightmares than the general population. This is the first study, to our knowledge, designed to characterize the sleep complaints of veterans in terms of the presence or absence of mental health diagnoses. Whereas prior studies used mental health symptom questionnaire cutoff scores to establish mental health diagnoses, a particular strength of this research is the use of structured clinical diagnostic interviews to identify those with and without mental health disorders.
In recent years, awareness has grown about the importance of treating sleep disturbance in IA veterans. The findings of our study highlight the breadth of the problem, and the need to address the sleep complaints of all veterans, regardless of mental health diagnostic status. Failing to do so may hasten the onset of a range of comorbid mental and physical health conditions, since sleep complaints and problems are known to precede the onset of psychiatric disorders, independently contribute to functional impairments, and increase the risk of cardiovascular disease. Many questions remain with regards to the trajectory of untreated sleep disturbance. Among these questions; we do not know if sleep interventions which convey improved sleep prevent the development of psychiatric illness or accelerate recovery in those with psychiatric disorders. Given the longitudinal findings of Baglioni and colleagues12 showing that insomnia is predictive of future depression, and Gehrman and colleagues13 showing that sleep characteristics and insomnia symptoms are predictive of future mental health disorders in IA veterans, it is reasonable to hypothesize that an effective sleep intervention might not only decrease sleep disturbance but could prevent the development of a mental health disorder among those not currently meeting diagnostic criteria. We also do not know if improving sleep could reduce the risk of future cardiovascular disease. In light of the findings of Haack and colleagues,52 wherein reduced blood pressure was a consequence of increased sleep duration in adults with early stage hypertension, it is reasonable to hypothesize that effective sleep interventions could, in fact, reduce cardiovascular disease risk as well. Given the personal and economic costs associated with the presence of a mental health disorder, and the fact that cardiovascular disease is the leading cause of death in US adults,53 future research testing these hypotheses is warranted.
Our findings should be considered in light of several limitations, namely, the use of cross-sectional data which cannot imply causation, the uncertainty about occult sleep disorders in our sample, and the inability to generalize from a sample of individuals volunteering for a research study to the larger population. As discussed above, our sample is not necessarily representative of all IA veterans and military personnel in that it was comprised of deployers only and contained more minorities, more female deployers, and fewer married individuals than the population of military personnel who have served in these conflicts. In addition, study participants were volunteers recruited from several VA hospitals in the southeast, and thus, may be more reflective of the demographic and/or military service characteristics of previously deployed military personnel living in the southeastern US. Despite these limitations, our findings underscore the prominence of sleep disturbance in IA veterans. When considered in light of prior research, our findings suggest that sleep disorders screening in previously deployed military personnel, both with and without mental health diagnoses, may serve as a primary prevention strategy for a multitude of physical and mental health conditions in this population.
DISCLOSURE STATEMENT
This was not an industry supported study. Christi S. Ulmer (CDA 09-218) and Elizabeth Van Voorhees (1K2RX001298) were supported by Veterans Affairs Research Career Development Awards while preparing this manuscript. This project was supported by the Mid-Atlantic Mental Illness Research, Education and Clinical Center (VISN 6 MIRECC) of the Department of Veterans Affairs Office of Mental Health Services, the VA Mid-Atlantic Healthcare Network (VISN 6), the Durham, NC Veterans Affairs Medical Center, and the Department of Veterans Affairs Office of Research and Development. The views expressed are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs or any of the institutions with which the authors are affiliated. The Mid-Atlantic Mental Illness Research, Education, and Clinical Center Workgroup for this manuscript includes: Patrick S. Calhoun, Eric B. Elbogen, John A. Fairbank, Jeffrey M. Hoerle, Christine E. Marx, Scott D. Moore, Rajendra A. Morey, Kristy A. Straits-Tröster, Larry A. Tupler, Richard D. Weiner, and H. Ryan Wagner from the Durham (NC) VA Medical Center; Marinell Miller-Mumford from the Hampton (VA) VA Medical Center; Antony Fernandez, Scott D. McDonald, and Treven C. Pickett from the Richmond (VA) VA Medical Center; Robin A. Hurley, Katherine H. Taber, and Ruth E. Yoash-Gantz from the Salisbury (NC) VA Medical Center; and Gregory McCarthy, from Yale University. The research described in this manuscript was conducted at VA facilities within the VISN 6 region.
ABBREVIATIONS
- CVD
cardiovascular disease
- DTS
Davidson Trauma Scale
- IA
Iraq-Afghanistan
- MH
mental health
- PSQI
Pittsburg Sleep Quality Index
- PSTD
posttraumatic stress disorder
REFERENCES
- 1.Seelig AD, Jacobson IG, Smith B, et al. Sleep patterns before, during, and after deployment to Iraq and Afghanistan. Sleep. 2010;33:1615–22. doi: 10.1093/sleep/33.12.1615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Amin M, Parisi JA, Gold MS, Gold AR. War-related illness symptoms among Operation Iraqi Freedom/Operation Enduring Freedom Returnees. Mil Med. 2010;175:155–7. doi: 10.7205/milmed-d-90-00153. [DOI] [PubMed] [Google Scholar]
- 3.Mysliwiec V, McGraw L, Pierce R, Smith P, Trapp B, et al. Sleep disorders and associated medical comorbidities in active duty military personnel. Sleep. 2013;36:167–74. doi: 10.5665/sleep.2364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Seal KH, Metzler TJ, Gima KS, et al. Trends and risk factors for mental health diagnoses among Iraq and Afghanistan Veterans using Department of Veterans Affairs Health Care, 2002–2008. Am J Public Health. 2009;99:1651–8. doi: 10.2105/AJPH.2008.150284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Roszell DK, McFall ME, Malas KL. Frequency of symptoms and concurrent psychiatric disorder in Vietnam veterans with chronic PTSD. Hosp Community Psychiatry. 1991;42:293–6. doi: 10.1176/ps.42.3.293. [DOI] [PubMed] [Google Scholar]
- 6.Ohayon MM, Shapiro CM. Sleep disturbances and psychiatric disorders associated with\ posttraumatic stress disorder in the general population. Compr Psychiatry. 2000;41:469–78. doi: 10.1053/comp.2000.16568. [DOI] [PubMed] [Google Scholar]
- 7.Germain A, Halla M, Krakow B, Sheara MK, Buysse DJ. A brief sleep scale for posttraumatic stress disorder: Pittsburgh Sleep Quality Index Addendum for PTSD. Anxiety Disord. 2005;19:233–44. doi: 10.1016/j.janxdis.2004.02.001. [DOI] [PubMed] [Google Scholar]
- 8.Babson K, Feldner M, Badourb C, et al. Posttraumatic stress and sleep: differential relations across types of symptoms, and sleep problems. J Anxiety Disord. 2011;25:706–13. doi: 10.1016/j.janxdis.2011.03.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mysliwiec V, O'Reilly B, Polchinski J, et al. Trauma associated sleep disorder: a proposed parasomnia encompassing disruptive nocturnal behaviors, nightmares, and REM without atonia in trauma survivors. J Clin Sleep Med. 2014;109:1143–8. doi: 10.5664/jcsm.4120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Benca R. Psychiatric Disorders. In: Meir H, Kryger TR, Dement WC, editors. Principles and practice of sleep medicine. 5th ed. St. Louis, MO: Elsevier Saunders; 2011. [Google Scholar]
- 11.Riemann D, Berger M, Voderholzer U. Sleep and depression—results from psychobiological studies: an overview. Biol Psychiatry. 2001;57:67–103. doi: 10.1016/s0301-0511(01)00090-4. [DOI] [PubMed] [Google Scholar]
- 12.Baglioni C, Battagliese G, Feige B, et al. Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies. J Affect Disord. 2011;135:10–9. doi: 10.1016/j.jad.2011.01.011. [DOI] [PubMed] [Google Scholar]
- 13.Gehrman P, Seelig AD, Jacobson IG, et al. Predeployment sleep duration and insomnia symptoms as risk factors for new-onset mental health disorders following military deployment. Sleep. 2013;36:1009–18. doi: 10.5665/sleep.2798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Pigeon WR, Britton PC, Ilgen MA, Chapman B, Conner KR. Sleep disturbance preceding suicide among veterans. Am J Public Health. 2012;102(Suppl 1):S93–7. doi: 10.2105/AJPH.2011.300470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Pigeon WR, Pinquart M, Conner K. Meta-analysis of sleep disturbance and suicidal thoughts and behaviors. J Clin Psychiatry. 2012;73:e1160–7. doi: 10.4088/JCP.11r07586. [DOI] [PubMed] [Google Scholar]
- 16.Schoenfeld FB, Deviva JC, Manber R. Treatment of sleep disturbances in posttraumatic stress disorder: a review. J Rehabil Res Dev. 2012;49:729–52. doi: 10.1682/jrrd.2011.09.0164. [DOI] [PubMed] [Google Scholar]
- 17.Ulmer CS, Edinger JD, Calhoun PS. A multi-component cognitive-behavioral intervention for sleep disturbance in veterans with PTSD: a pilot study. J Clin Sleep Med. 2011;7:57–68. [PMC free article] [PubMed] [Google Scholar]
- 18.Talbot LS, Maguen S, Metzler TJ, et al. Cognitive behavioral therapy for insomnia in posttraumatic stress disorder: a randomized controlled trial. Sleep. 2014;37:327–41. doi: 10.5665/sleep.3408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hoge CW, Terhakopian A, Castro CA, Messer SC, Engel CC. Association of posttraumatic stress disorder with somatic symptoms, health care visits, and absenteeism among Iraq war veterans. Am J Psychiatry. 2007;164:150–3. doi: 10.1176/ajp.2007.164.1.150. [DOI] [PubMed] [Google Scholar]
- 20.Lew HL, Pogoda TK, Hsu PT, et al. Impact of the “polytrauma clinical triad” on sleep disturbance in a department of veterans affairs outpatient rehabilitation setting. Am J Phys Med Rehabil. 2010;89:437–45. doi: 10.1097/PHM.0b013e3181ddd301. [DOI] [PubMed] [Google Scholar]
- 21.Faestel P, Littell CT, Vitiello MV, Forsberg CW, Littman AJ. Perceived insufficient rest or sleep among veterans: Behavioral Risk Factor Surveillance System 2009. J Clin Sleep Med. 2013;9:577–84. doi: 10.5664/jcsm.2754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ikehara S, Iso H, Date C, et al. Association of sleep duration with mortality from cardiovascular disease and other causes for Japanese men and women: the JACC Study. Sleep. 2009;32:259–301. doi: 10.1093/sleep/32.3.295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Chien K, Chen P, Hsu H, et al. Habitual sleep duration and insomnia and the risk of cardiovascular events and all-cause death: report from a community-based cohort. Sleep. 2010;33:177–84. doi: 10.1093/sleep/33.2.177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Cappuccio F, Miller MA. Sleep and mortality: cause, consequence, or symptom? Sleep Med. 2013;14:587–8. doi: 10.1016/j.sleep.2013.04.001. [DOI] [PubMed] [Google Scholar]
- 25.Patel S, Hu FB. Short sleep duration and weight gain: a systematic review. Obesity. 2008;16:643–53. doi: 10.1038/oby.2007.118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hall M, Muldoon MF, Jennings JR, et al. Self-reported sleep duration is associated with the metabolic syndrome in midlife adults. Sleep. 2008;31:635–43. doi: 10.1093/sleep/31.5.635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Yaggi H, Araujo AB, McKinlay JB. Sleep duration as a risk factor for the development of type 2 diabetes. Diabetes Care. 2006;29:657–61. doi: 10.2337/diacare.29.03.06.dc05-0879. [DOI] [PubMed] [Google Scholar]
- 28.Kripke D, Langer RD, Elliott JA, Klauber MR, Rex KM. Mortality related to actigraphic long and short sleep. Sleep Med. 2011;12:28–33. doi: 10.1016/j.sleep.2010.04.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Gangwisch J, Heymsfield SB, Boden-Albala B, et al. Short sleep duration as a risk factor for hypertension: analyses of the First National Health and Nutrition Examination Survey. Hypertension. 2006;47:833–9. doi: 10.1161/01.HYP.0000217362.34748.e0. [DOI] [PubMed] [Google Scholar]
- 30.Crum-Cianflone N, Bagnell ME, Schaller E, et al. Impact of combat deployment and posttraumatic stress disorder on newly reported coronary heart disease among US active duty and reserve forces. Circulation. 2014;129:1813–20. doi: 10.1161/CIRCULATIONAHA.113.005407. [DOI] [PubMed] [Google Scholar]
- 31.Gangwisch J, Feskanich D, Malaspina D, Shen S, Forman JP. Sleep duration and risk for hypertension in women: results from the nurses' health study. Am J Hypertension. 2013;26:903–11. doi: 10.1093/ajh/hpt044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.First MB, Spitzer RL, Gibbon M, Williams JBW. New York: Biometrics Research, New York State Psychiatric Institute; 1996. Structured Clinical Interview for the DSM-IV Axis I Disorders. [Google Scholar]
- 33.Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213. doi: 10.1016/0165-1781(89)90047-4. [DOI] [PubMed] [Google Scholar]
- 34.Carpenter JS, Andrykowski MA. Psychometric evaluation of the Pittsburgh Sleep Quality Index. J Psychosom Res. 1998;45:5–13. doi: 10.1016/s0022-3999(97)00298-5. [DOI] [PubMed] [Google Scholar]
- 35.Insana SP, Hall M, Buysse DJ, Germain A. Validation of the Pittsburgh Sleep Quality Index Addendum for posttraumatic stress disorder (PSQI-A) in U.S. male military veterans. J Trauma Stress. 2013;26:192–200. doi: 10.1002/jts.21793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Derogatis LR, Savitz KL. The SCL-90-R and the Brief Symptom Inventory (BSI) in Primary Care. In: Maruish ME, editor. Handbook of psychological assessment in primary care settings. Mahwah, NJ: Lawrence Erlbaum; 2000. pp. 297–334. [Google Scholar]
- 37.Davidson JR, Book SW, Colket JT, et al. Assessment of a new self-rating scale for post-traumatic stress disorder. Psychol Med. 1997;27:153–60. doi: 10.1017/s0033291796004229. [DOI] [PubMed] [Google Scholar]
- 38.McDonald SD, Beckham JC, Morey RA, Calhoun PS. The validity and diagnostic efficacy of the Davidson Trauma Scale in military veterans who have served since September 11, 2001. J Anxiety Disord. 2009;23:247–55. doi: 10.1016/j.janxdis.2008.07.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Sijbrandij M, Olff M, Opmeer BC, Carlier IV, Gersons BP. Early prognostic screening for posttraumatic stress disorder with the Davidson Trauma Scale and the SPAN. Depress Anxiety. 2008;25:1038–45. doi: 10.1002/da.20441. [DOI] [PubMed] [Google Scholar]
- 40.Institute of Medicine. Returning home from Iraq and Afghanistan: assessment of readjustment needs of veterans, service members, and their families. National Academies Press; 2013. Deployment Characteristics. [PubMed] [Google Scholar]
- 41.Lichstein K, Durrence HH, Taylor DJ, Bush AJ, Riedel BW. Quantitative criteria for insomnia. Behav Res Ther. 2003;41:427–45. doi: 10.1016/s0005-7967(02)00023-2. [DOI] [PubMed] [Google Scholar]
- 42.American Academy of Sleep Medicine. Darien, IL: American Academy of Sleep Medicine; 2014. International classification of sleep disorders, 3rd ed. [Google Scholar]
- 43.Grandner M, Kripke DF, Yoon I, Youngstedt SD. Criterion validity of the Pittsburgh Sleep Quality Index: investigation in a non-clinical sample. Sleep Biol Rhythms. 2006;4:129–39. doi: 10.1111/j.1479-8425.2006.00207.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Luxton D, Greenburg D, Ryan J, et al. Prevalence and impact of short sleep duration in redeployed OIF soldiers. Sleep. 2011;34:1189–95. doi: 10.5665/SLEEP.1236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Centers for Disease Control. Perceived insufficient rest or sleep among adults--United States, 2008. Morb Mortal Wkly Rep Surveill Summ. 2009;58:1175–9. [PubMed] [Google Scholar]
- 46.Steptoe A, Peacey V, Wardle J. Sleep duration and health in young adults. Arch Intern Med. 2006;166:1689–92. doi: 10.1001/archinte.166.16.1689. [DOI] [PubMed] [Google Scholar]
- 47.Pietrzak R, Morgan CA, Southwick SM. Sleep quality in treatment-seeking veterans of Operations Enduring Freedom and Iraqi Freedom: the role of cognitive coping strategies and unit cohesion. J Psychosom Res. 2010;69:441–8. doi: 10.1016/j.jpsychores.2010.07.002. [DOI] [PubMed] [Google Scholar]
- 48.Babson KA, Blonigen DM, Boden MT, Drescher KD, Bonn-Miller MO. Sleep quality among U.S. Military veterans with PTSD: a factor analysis and structural model of symptoms. J Trauma Stress. 2012;25:665–74. doi: 10.1002/jts.21757. [DOI] [PubMed] [Google Scholar]
- 49.Edinger J, Fins AI. The distribution and clinical significance of sleep time misperceptions among insomniacs. Sleep. 1995;18:232–9. doi: 10.1093/sleep/18.4.232. [DOI] [PubMed] [Google Scholar]
- 50.Pigeon WR, Campbell CE, Possemato K, Ouimette P. Longitudinal relationships of insomnia, nightmares, and PTSD severity in recent combat veterans. J Psychosom Res. 2013;75:546–50. doi: 10.1016/j.jpsychores.2013.09.004. [DOI] [PubMed] [Google Scholar]
- 51.Sandman N, Valli K, Kronholm E, et al. Nightmares: prevalence among the Finnish general adult population and war veterans during 1972-2007. Sleep. 2013;36:1041–50. doi: 10.5665/sleep.2806. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Haack M, Serrador J, Cohen D, et al. Increasing sleep duration to lower beat-to-beat blood pressure: a pilot study. J Sleep Res. 2013;22:295–304. doi: 10.1111/jsr.12011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Centers for Disease Control. Heart Disease Facts. Updated February 19, 2015. Retrieved from http://www.cdc.gov/heartdisease/facts.htm.