

Abstract
A 50-year-old man was found to have an incidental peri-adrenal cystic lesion on CT imaging which was removed laparoscopically. Histological examination showed a cystic structure composed of respiratory and cuboidal-type epithelium with underlying smooth muscle, cartilage and seromucinous glands. The differential diagnosis for such a lesion includes bronchogenic cyst or teratoma differentiated. This case report offers an overview of both the conditions and the difficulties encountered in the histological distinction.
Background
The increasing use of CT and MR imaging has led to a rise in unexpected abnormal findings, frequently termed as ‘incidentalomas’. Four to ten per cent of adults are reported to have incidental adrenal masses on CT imaging,1 although no such data are available for peri-adrenal cystic lesions. Peri-adrenal cysts are most often benign, but warrant further investigation to distinguish them from less common malignant conditions.
Case presentation
A 50-year-old man was found to have an incidental cystic lesion in the left adrenal region following investigation for a caecal mass, subsequently found to be a tubular adenoma. The CT imaging showed a lobulated lesion adjacent to the left adrenal gland measuring 19 mm diameter. There was no evidence of metastatic disease; the liver, pancreas, spleen and kidneys were normal. Re-imaging 6 months later showed the cyst had increased in size to 23 mm. There were no endocrinological symptoms; glucocorticoid, mineralocorticoid and catecholamine levels were normal. Owing to the relative and increasing size of the lesion it was regarded as potentially neoplastic and adrenalectomy was therefore advised to allow definitive diagnosis.
The patient underwent laparoscopic adrenalectomy. The left adrenal gland was removed with an adjacent cystic lesion located superior to the adrenal. It was well defined with no evidence of communication with adjacent structures or rupture. The vascular supply could not be determined. An uneventful recovery was made from surgery.
Microscopically the adrenal gland was unremarkable. The adjacent cystic tissue was multiloculated and lined by cuboidal epithelium and ciliated pseudostratified epithelium, reminiscent of respiratory epithelium. Subepithelial stroma contained smooth muscle, cartilage, seromucinous glands and neurovascular bundles (figure 1A–C). No atypia was seen. The appearances were of a multiloculated cystic structure replicating the bronchogenic tree.
Figure 1.
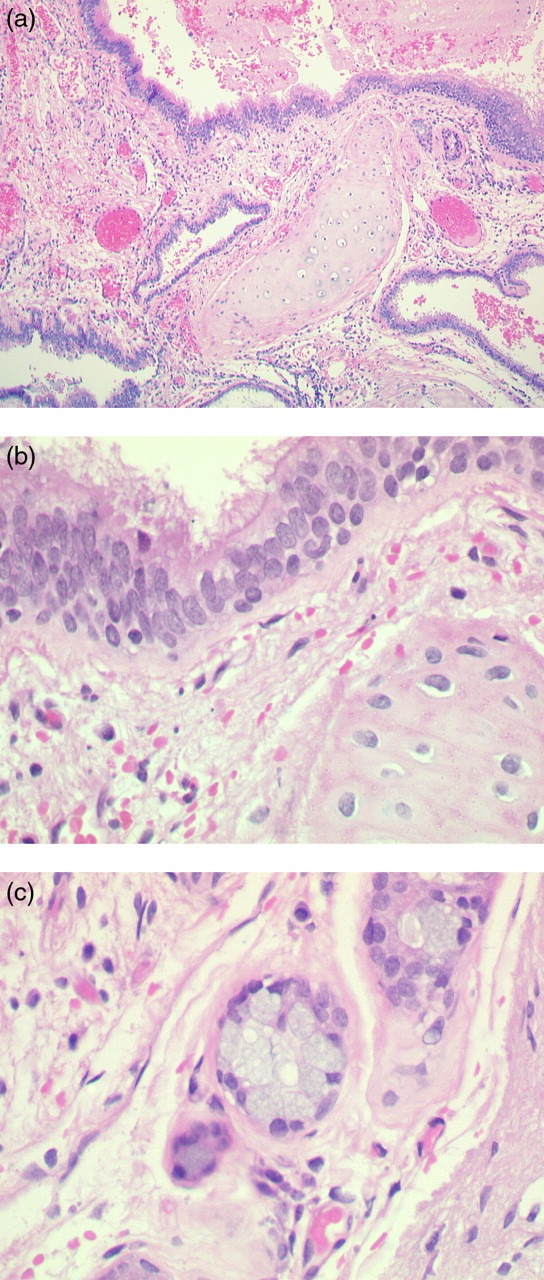
(A) Multiloculated cystic tissue lined by ciliated pseudostratified epithelium with stroma containing cartilage and seromucinous glands (stain, H&E; original magnification, ×10). (B) Respiratory epithelium overlying stroma containing cartilage (stain, H&E; original magnification, ×60). (C) Stroma containing seromucinous glands (stain, H&E; original magnification, ×60).
Differential diagnosis
The differential diagnosis of a peri-adrenal cystic lesion composed of respiratory structures includes bronchogenic cyst or cystic teratoma.1 2 The typical features of intestinal duplication cyst with replication of the normal alimentary tract layers (submucosa and muscularis propria) are not present in this case.3
Bronchogenic cysts are a rare developmental abnormality of the primitive foregut that arise during early embryogenesis from abnormal budding of the developing tracheobronchial tree. They most commonly occur in the thoracic cavity but can occur elsewhere, including the retroperitoneum.4 They are usually asymptomatic unless complicated by perforation, become secondarily infected, compress adjacent structures or show neoplastic transformation.5
Teratomas can be composed of a variety of different parenchymal cell types which represent one or more germ cell layers.6 They are usually encountered in the gonads; however, they may occur in sequestered rests of cells in midline locations and may rarely be seen in the peri-adrenal region.7 Teratomas may be benign or malignant. A peri-adrenal teratoma could therefore represent a primary tumour or metastatic spread.
Discussion
Histologically, bronchogenic cysts are composed of elements found in the tracheobronchial tree including respiratory-type epithelium, smooth muscle, seromucinous glands and cartilage. Squamous metaplasia has been reported.5 Teratomas can comprise a host of tissues including squamous, ciliated and glandular epithelia. In similarity with bronchogenic cysts; respiratory epithelium, cartilage and smooth muscle can be seen.2
Differentiation is usually straightforward, for example, the presence of skin structures, neural crest or elements not seen in bronchogenic cyst would be in keeping with teratoma. However, shared histological features may make differentiation difficult or potentially impossible.8
The case report, as described, includes respiratory and cuboidal epithelium, smooth muscle, nerves, cartilage and seromucinous glands. These were arranged in a manner resembling that of the tracheobronchial tree. This suggested that bronchogenic cyst was more likely than teratoma. The patient was followed up with examination of the gonads and germ cell tumour markers, all of which were normal. The clinical findings in conjunction with histology were in keeping with bronchogenic cyst.
The three previous peri-adrenal cyst case reports where the same differential diagnosis was encountered draw differing conclusions. In one, the lack of all three germ cell layers was interpreted as in keeping with a diagnosis of bronchogenic cyst, in another the diagnosis of bronchogenic cyst was determined more by the organisation of tissue resembling that of the normal bronchus and in the third, differentiation could not be reached.5 8 9
Specialist techniques, such as cytogenetic or fluorescence in situ hybridisation testing for the isochromosome 12p (a specific chromosomal abnormality in some teratomas), may help achieve a diagnosis but this is not performed routinely in most histology departments.2
In summary, peri-adrenal cysts may be seen increasingly as ‘incidentalomas’ with the rise in CT and MR imaging. This is the fourth such reported case of a peri-adrenal cystic lesion where the differential diagnosis included bronchogenic cyst or teratoma. In all cases the cysts arose on the left side. Histology still remains the routine method of diagnosis and this case serves to highlight the difficulties encountered in differentiation.
Learning points.
Peri-adrenal cysts composed of mixed tissue types can give rise to the histological differential diagnosis of bronchogenic cyst or teratoma differentiated.
The continuing rise in CT and MR imaging may lead to more such lesions being discovered as ‘incidentalomas’.
Differentiation may not always be possible, owing to histological similarities.
Footnotes
Competing interests: None.
Patient consent: Obtained.
References
- 1.Dunnick N, Korobkin M. Imaging of adrenal incidentalomas: current status. Am J Roentgenol 2002;179:559–68. [DOI] [PubMed] [Google Scholar]
- 2.Roma A, Varsegi M, Magi-Galluzzi C, et al. The distinction of bronchogenic cyst from metastatic testicular teratoma. Am J Clin Pathol 2008;130:265–73. [DOI] [PubMed] [Google Scholar]
- 3.Otter M, Marks C, Cook M. An unusual presentation of intestinal duplication with a literature review. Digest Dis Sci 1996;41:627–9. [DOI] [PubMed] [Google Scholar]
- 4.Petrina A, Boselli C, Cirocchi R, et al. Bronchogenic cyst of the ileal mesentery: a case report and a review of literature. J Med Case Reports 2010;4:313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Chung J, Jung M, Lee W, et al. Retroperitoneal bronchogenic cyst presenting as adrenal tumour in adult successfully treated with retroperitoneal laparoscopic surgery. Urology 2009;73:13–15. [DOI] [PubMed] [Google Scholar]
- 6.Gatcombe H, Assikis V, Kooby D, et al. Primary retroperitoneal teratomas: a review of the literature. J Surg Oncol 2004;86:107–13. [DOI] [PubMed] [Google Scholar]
- 7.Kalyanasundaram K, Beacock C, Otter M. Teratoma differentiated with predominant cartilaginous differentiation. Diagn Histopathol 2010;16:306–8. [Google Scholar]
- 8.Onol F, Baytekin F, Dikbas O, et al. A retroperitoneal bronchogenic cyst mimicking adrenal tumour in an adult: is differential diagnosis truly possible? J Clin Pathol 2009;62:187–9. [DOI] [PubMed] [Google Scholar]
- 9.Yang S, Linton J, Ryu S, et al. Retroperitoneal multilocular bronchogenic cyst adjacent to adrenal gland. Yonsei Med J 1999;40:523–6. [DOI] [PubMed] [Google Scholar]