

Abstract
Calcific tendonitis of the quadriceps tendon is an uncommon condition. We present the first case of a quadriceps tendon tear associated with calcific tendonitis. In this case, the patient presented with symptoms mimicking a rupture of the quadriceps tendon. This case illustrates that although calcific tendonitis of the quadriceps is a rare condition it is not benign and should be considered when investigating acute symptoms associated with the extensor mechanism of the knee.
Background
Calcific tendonitis is defined as the presence of macroscopic deposits of hydroxyapatite (a crystalline calcium phosphate) in a tendon1 and is a multifocal, cell-mediated calcification process.2 It has been described associated with most joints of the body and is particularly common in the rotator cuff tendons of the shoulder.1 3 Calcific tendonitis of the quadriceps tendon is reported uncommonly.4–6
Rupture of the quadriceps tendon is usually traumatic and has been described in association with infection, gout, obesity, hyperparathyroidism, systemic lupus erythematosis and chronic renal failure.7–10
We present the case of a partial quadriceps tendon tear associated with calcific tendonitis of the quadriceps with symptoms mimicking rupture of the tendon.
Case presentation
A 43-year-old man carpenter presented to the emergency department describing an acute onset of severe right knee pain. There was no history of trauma. The patient felt otherwise well with no reported symptoms of malaise or fever. He reported that prior to the acute event he had suffered from mild knee pain for approximately 1 year and this had been managed with short courses of non-steroidal anti-inflammatory drugs. He was discharged from the emergency department with a diagnosis of suprapatellar bursitis but represented 1 week later with persistent pain in the right knee.
On review at this time, he remained systemically well. The right knee was warm to touch with localised erythema over the superior pole of the patella and a grade 1 effusion. The patient was unable to straight leg raise and passive flexion was limited to 20°.
Investigations
Blood results showed a C reactive protein level of 7.9 mg/l and white cell count of 7.2×109/l. Joint fluid aspirate was unremarkable with no organisms seen on Gram stain, no growth following extended incubation on enriched culture medium, and no crystals.
Plain radiographs of the knee showed a classical bony spur ‘whiskers’3–6 11 and erosion at the insertion of the quadriceps tendon into the patella (figure 1). There was no chondrocalcinosis.
Figure 1.
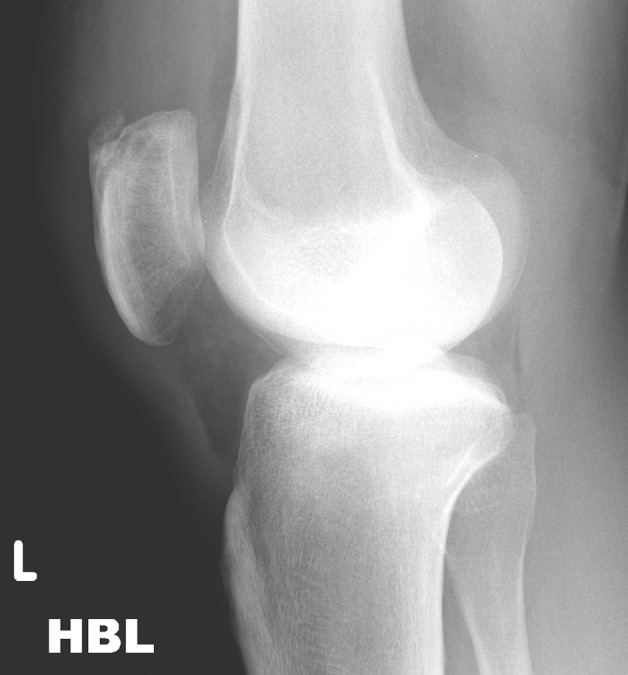
Plain radiograph of the knee showing a classical bony spur and erosion at the insertion of the quadriceps tendon into the patella.
Ultrasound examination revealed no evidence of a quadriceps or patella tendon rupture but did delineate a focal area of tissue or collection around the quadriceps tendon. An MRI demonstrated similar findings but demonstrated a likely tear of the central portion of the distal quadriceps tendon (figure 2a,b).
Figure 2.
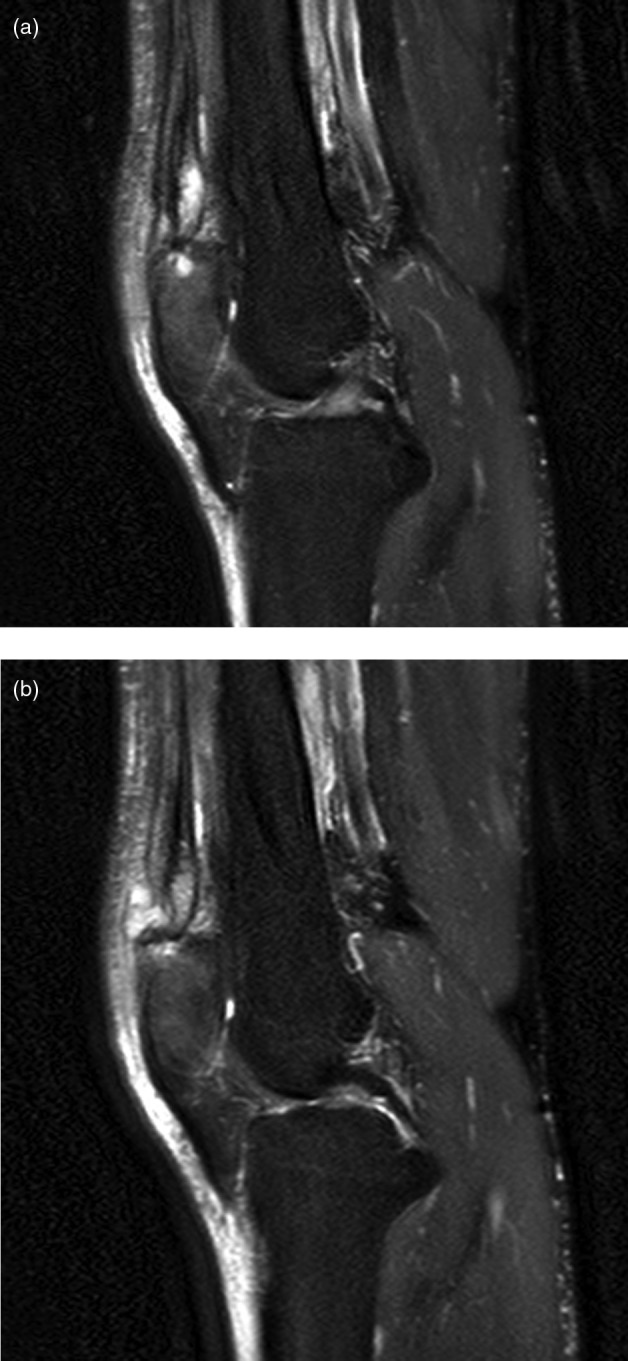
(a and b) MRI demonstrating tear of the central portion of the distal quadriceps tendon.
Treatment
A diagnosis of a quadriceps tendon tear was made and the patient was booked for operative intervention. Intraoperatively, a central quadriceps tendon tear was confirmed in association with white, chalky material embedded in the central portion of the tendon and inflammatory tissue over the superior pole of the patella. The abnormal material was removed by curette and histology excluded gout.
The defect in the quadriceps tendon was repaired and the patient did well postoperatively and had an uneventful discharge.
Outcome and follow-up
At 6-week follow-up, the patient had a fully active straight leg raise and was capable of both passive and active flexion to 90°. At 12-month follow-up the patient reported no impairment to his active lifestyle and no knee pain. His range of movement at 12 months was 0–130° flexion.
Discussion
Calcific tendonitis is a cell-mediated process2 which uncommonly affects the quadriceps tendon.4–6 Although a degree of calcification may occur as part of the ageing process, our patient was young and otherwise fit and well. Operative findings demonstrated a significant chalky deposit in the body of the tendon and calcific tendonitis has not previously been reported in association with an atraumatic tear of the quadriceps tendon. In this case, the patient's symptoms mimicked quadriceps tendon rupture as has been reported previously with calcific tendonitis of the patella tendon.12 The diagnosis was made only after multimodality imaging had been performed, followed by surgical exploration.
The majority of the research on calcific tendonitis relates to its presence in the shoulder. This is because it is a relatively common condition in the shoulder, being present in approximately 7% of patients with shoulder pain.13 Here, calcific tendonitis may be managed in a number of ways including conservative medical management, extracorporeal shockwave therapy and arthroscopic or open surgery.1 Conservative management is effective in greater than 60% of cases of calcific tendonitis in the shoulder and surgery is only advocated for severe or refractive symptoms13 14 Ultrasound and extracorporal shockwave therapy is more effective than sham therapy but further research is required into this treatment modality14 15 A similar response and natural history might be expected in the quadriceps tendon in the absence of an acute tear or rupture. In the shoulder, a rotator cuff tear associated with dystrophic calcification at the site of the tear is thought to be associated with a poor prognosis.1 Furthermore, calcific tendonitis may increase the risk of a rotator cuff tear.16 Given the comparative rarity of calcific tendonitis of the quadriceps tendon, similar data has not been published for this condition, but it is probable that similar associations would be found in this group of patients.
Partial tears of the quadriceps tendon are generally managed conservatively in a full extension brace for 6 weeks followed by protected range of motion exercises with good outcomes and regain of function.7 In the case of complete quadriceps tendon rupture or where diagnosis is uncertain, repair is advocated as outcomes of conservative management in terms of disability and weakness are poor.7 Our patient was managed by open, operative treatment due to the severity of the symptoms and imaging findings suggesting tendon damage but some remaining diagnostic uncertainty. There was an excellent recovery to baseline level of function. Given that calcific tendonitis may be associated with worse outcomes in rotator cuff tears of the shoulder, a lower threshold for surgical exploration and debridement in cases of quadriceps tendon tears in association with calcific tendonitis may be appropriate.
Our case demonstrates that calcific tendonitis is not a benign condition and an awareness of the condition and the potential complication of quadriceps tendon damage is important when investigating acute symptoms associated with the extensor mechanism of the knee.
Learning points.
Calcific tendonitis is not a benign condition.
Calcific tendonitis should be considered when investigating acute symptoms associated with extensor mechanism of the knee.
Footnotes
Competing interests: None.
Patient consent: Obtained.
References
- 1.Speed CA, Hazleman BL. Calcific tendinitis of the shoulder. N Engl J Med 1999;340:1582–4. [DOI] [PubMed] [Google Scholar]
- 2.Uhthoff HK, Loehr JW. Calcific tendinopathy of the rotator cuff: pathogenesis, diagnosis, and management. J Am Acad Orthop Surg 1997;5:183–91. [DOI] [PubMed] [Google Scholar]
- 3.Holt PD, Keats TE. Calcific tendinitis: a review of the usual and unusual. Skeletal Radiol 1993;22:1–9. [DOI] [PubMed] [Google Scholar]
- 4.Varghese B, Radcliffe GS, Groves C. Calcific tendonitis of the quadriceps. Br J Sports Med 2006;40:652–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Macurak RB, Goldman JA, Hirsh E, et al. Acute calcific quadriceps tendinitis. South Med J 1980;73:322–5. [DOI] [PubMed] [Google Scholar]
- 6.Trujeque L, Spohn P, Bankhurst AD, et al. Patellar whiskers and acute calcific quadriceps tendinitis in a general hospital population. Arthritis Rheum 1977;20:1409–12. [DOI] [PubMed] [Google Scholar]
- 7.Ilan DI, Tejwani N, Keschner M, et al. Quadriceps tendon rupture. J Am Acad Orthop Surg 2003;11:192–200. [DOI] [PubMed] [Google Scholar]
- 8.Thaunat M, Gaudin P, Naret C, et al. Role of secondary hyperparathyroidism in spontaneous rupture of the quadriceps tendon complicating chronic renal failure. Rheumatology (Oxford) 2006;45:234–5. [DOI] [PubMed] [Google Scholar]
- 9.MacEachern AG, Plewes JL. Bilateral simultaneous spontaneous rupture of the quadriceps tendons. Five case reports and a review of the literature. J Bone Joint Surg Br 1984;66:81–3. [DOI] [PubMed] [Google Scholar]
- 10.Wener JA, Schein AJ. Simultaneous bilateral rupture of the patellar tendon and quadriceps expansions in systemic lupus erythematosus. A case report. J Bone Joint Surg Am 1974;56823–4. [PubMed] [Google Scholar]
- 11.Hardy JR, Chimutengwende-Gordon M, Bakar I. Rupture of the quadriceps tendon: an association with a patellar spur. J Bone Joint Surg Br 2005;87:1361–3. [DOI] [PubMed] [Google Scholar]
- 12.Dey A, Godsiff SP, Pandey R. Acute calcific tendinitis mimicking patella tendon rupture. Injury Extra 2004;35:104–7. [Google Scholar]
- 13.Uhthoff HK, Sarkar K. Calcifying tendinitis. Baillieres Clin Rheumatol 1989;3:567–81. [DOI] [PubMed] [Google Scholar]
- 14.Hsu CJ, Wang DY, Tseng KF, et al. Extracorporeal shock wave therapy for calcifying tendinitis of the shoulder. J Shoulder Elbow Surg 2008;17:55–9. [DOI] [PubMed] [Google Scholar]
- 15.Ebenbichler GR, Erdogmus CB, Resch KL, et al. Ultrasound therapy for calcific tendinitis of the shoulder. N Engl J Med 1999;340:1533–8. [DOI] [PubMed] [Google Scholar]
- 16.Jim YF, Hsu HC, Chang CY, et al. Coexistence of calcific tendinitis and rotator cuff tear: an arthrographic study. Skeletal Radiol 1993;22:183–5. [DOI] [PubMed] [Google Scholar]