

Abstract
We report a case of a 41-year-old lady, who developed severe hypotension and sinus bradycardia, following oral consumption of 20 g of phenytoin and 500 mg of glibenclamide. She required high dose of inotropes and a temporary transvenous pacer for her hemodynamic instability. This life-threatening cardiotoxicity of phenytoin could have been due to its interaction with sulphonylurea. It is imperative to be aware of drug interactions, due to which, life-threatening cardiovascular manifestations following phenytoin toxicity can occur.
Keywords: Cardiotoxicity, glibenclamide, sulphonylurea
INTRODUCTION
Phenytoin overdose through oral route presents predominantly with neurologic manifestations. Though cardiotoxic effect of phenytoin following rapid parenteral administration is well documented, there are few reports of symptomatic bradycardia following oral toxicity. We, hereby, report a patient of phenytoin and glibenclamide overdose, manifesting as severe bradycardia with hemodynamic instability, who recovered with temporary transvenous pacing.
CASE REPORT
A 41-year-old female presented to our emergency department a day after ingestion of 200 tablets of phenytoin 100 mg (20 g) and 100 tablets of glibenclamide 5 mg (500 mg) with suicidal intent. She was not a diabetic and these tablets were purchased by her mother who suffered from epilepsy and diabetes. She was taken to a local hospital, stomach wash and i.v. dextrose was given and referred to our centre. Referral slip had documented a pulse rate of 68/min and BP of 100/70 mmHg. At arrival to our ED she was stuporous. Her pulse rate was 56/min, BP of 70/50 mmHg with poor respiratory efforts. She was intubated and connected to mechanical ventilator immediately. Blood sugar was 112 mg/dl. A diagnosis of phenytoin toxicity causing hemodynamic instability was made and resuscitative measures initiated. Baseline ECG revealed sinus rhythm with bradycardia and no evidence of ischemia [Figure 1]. Arterial blood gas (ABG) showed fully compensated high anion gap metabolic acidosis secondary to hypotension. Serial phenytoin levels are shown in Table 1. Lab investigations revealed normal renal and thyroid functions with deranged liver function [Table 2].
Figure 1.
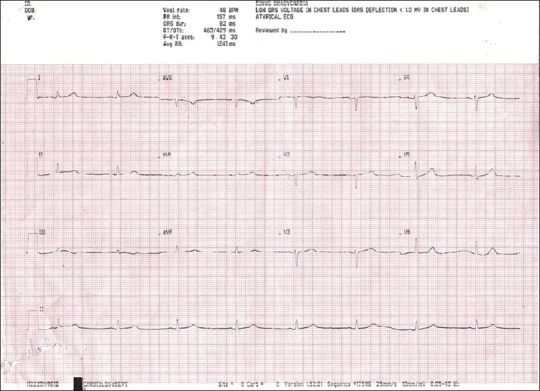
ECG on day of admission showing sinus bradycardia with a PR interval of 160 msec and corrected QTc of 430 msec
Table 1.
Serial serum phenytoin level

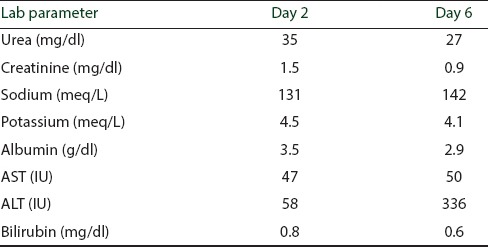
Table 2.
Laboratory parameters of the patient on days 2 and 6 after consumption of drugs
Since BP did not improve with fluid bolus, central line was placed and her central venous pressure was found to be 14 cm of normal saline. She was started on noradrenaline (NE) followed by dopamine infusion. Her inotropic support was titrated gradually and she required 40 μg/min of NE and 15 μg/min/kg of dopamine to maintain a BP of 90/60 mmHg and output of 1500 ml over the next 24 hours. On day 2 she developed bradycardia with rate of 40/min and BP dropped to 80/60 mmHg. ECG showed it to be a sinus bradycardia with a PR interval of 160 msec and corrected QTc of 430 msec [Figure 1]. Owing to hemodynamic instability, unresponsiveness to atropine and inotropes, she was transvenously paced through right femoral vein and ECG was recorded [Figure 2]. Following pacing, her inotropic requirements came down to about 20 μg/min of NE and 8 μg/kg/min of dopamine on day 3. Her temporary venous pacer was turned off on day 5 as her intrinsic rate improved to 80/min and she was off inotropes. She was on 10% dextrose infusion for first 3 days but hypoglycemia was never documented. On day 4 of hospital stay, her sensorium normalized, nystagmus was present. ECHO did not reveal any systolic dysfunction. She was extubated on day 6 and discharged on day 12. At discharge, she was completely asymptomatic without any neurologic sequelae.
Figure 2.
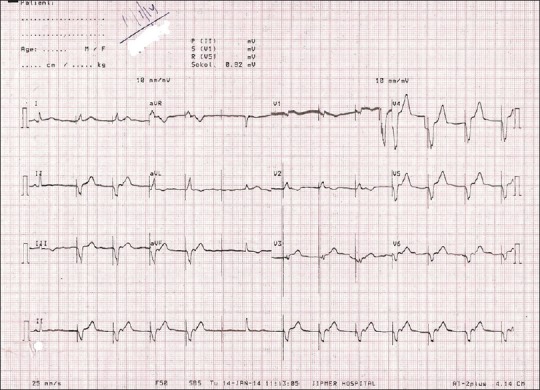
Post-pacing ECG showing left bundle branch block
DISCUSSION
Phenytoin toxicity usually results from intentional overdose, dosage adjustments, drug interactions, or alterations in physiology. Acute toxicity following oral ingestion manifests with central nervous system manifestations affecting the cerebellar and vestibular systems. Phenytoin concentration greater than 30 mg/l are associated with ataxia and poor coordination and concentration exceeding 50 mg/l cause lethargy, slurred speech, pyramidal and extrapyramidal manifestations and even coma.[1,2] Cardiovascular toxicity following parenteral administration of phenytoin is known. It impairs myocardial contractility, decreases peripheral vascular resistance and depresses cardiac conduction. A case study of 200 patients receiving intravenous phenytoin showed an incidence of 3.5% cardiovascular complications with no associated mortality. Hypotension, dysrhythmia, and cardiac arrest correlated with the rate of administration and total dose infused.[3] Cardiotoxicity following oral ingestion of phenytoin is documented in literature by Su et al. and Thimmisetty et al.[4,5] Wyte and Berk evaluated 57 patients with severe oral phenytoin overdose (defined as mean peak level of 40 μg/ml) and concluded that there was no clinically significant cardiotoxicity.[6] The largest case series of phenytoin toxicity was reported by Curtis et al. They studied 94 patients with phenytoin overdose but none of them manifested hemodynamic instability or clinically significant electrocardiographic abnormalities.[7] We hypothesize that the cardiotoxicity experienced by our patient could be due to the drug interaction between phenytoin and glibenclamide. p-Hydroxylation is the major metabolic pathway of phenytoin, and forms 5-(p-hydroxyphenyl)-5-phenylhydantoin (HPPH), which accounts for 90% of all metabolites in humans. This conversion is catalysed mainly by CYP2C9, although CYP2C19 also plays a role.[8] Although there are no in vivo studies of the effect of glibenclamide on CYP2C9-catalyzed metabolism, an in vitro study showed that it strongly inhibited CYP2C9-catalyzed phenytoin metabolism in a competitive manner and concluded that clinically significant drug-drug interactions will ensue when glibenclamide is co-administered with agents that are cleared primarily by the CYP2C9-mediated pathway and those with narrow therapeutic range such as phenytoin.[9]
There are few reports of cardiotoxicity from sulphonylurea overdose in previous literature, and concerns persist about their potential to inhibit ischemic preconditioning via blockade of myocardial KATP channels. Although the effect of phenytoin on the electrophysiology of SA node in situ heart is variable, high plasma levels usually do not cause severe bradycardia in patients without sinus node disease.[10] The severe bradycardia noted in our patient without any evidence of pre-existing sinus node disease could have been due to the interaction of phenytoin with the sulphonyl urea leading to its accumulation to extremely high levels. Glibenclamide has been shown to have anti-arrhythmic effect similar to class 3 agents in vitro[11] but there is no data regarding the electrophysiological effects in vivo, when these two antiarrhythmic are taken together in toxic dose. Nordin C refers to proarrythmic effect of hypoglycemia;[12] however, this patient did not have hypoglycemia due to continuous dextrose infusion since admission.
CONCLUSIONS
To conclude, we want to highlight the drug interaction between glibenclamide and phenytoin which probably lead to severe bradycardia and hypotension in the patient but recovered with timely insertion of a temporary pacemaker.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Craig S. Phenytoin poisoning. Neurocrit Care. 2005;3:161–70. doi: 10.1385/NCC:3:2:161. [DOI] [PubMed] [Google Scholar]
- 2.Doyon S. Anticovulsants. In: Flomenbaum NE, Goldfrank LR, Hoffman RS, Howland MA, Lewin NA, Nelson LS, editors. Goldfrank'S Toxicologic Emergencies. 8th ed. New York: McGraw-Hill; 2006. pp. 733–5. [Google Scholar]
- 3.Earnest MP, Marx JA, Drury LR. Complications of intravenous phenytoin for acute treatment of seizures. Recommendations for usage. JAMA. 1983;249:762–5. [PubMed] [Google Scholar]
- 4.Su CM, Kung CT, Wang YC, Lu CH. Life-threatening cardiotoxicity due to chronic oral phenytoin overdose. Neurol India. 2009;57:200–2. doi: 10.4103/0028-3886.51296. [DOI] [PubMed] [Google Scholar]
- 5.Thimmisetty RK, Gorthi JR, Abu Hazeem M. Oral phenytoin toxicity causing sinus arrest: A case report. Case Rep Cardiol 2014. 2014 doi: 10.1155/2014/851767. 851767. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wyte CD, Berk WA. Severe oral phenytoin overdose does not cause cardiovascular morbidity. Ann Emerg Med. 1991;20:508–12. doi: 10.1016/s0196-0644(05)81604-x. [DOI] [PubMed] [Google Scholar]
- 7.Curtis DL, Piibe R, Ellenhorn MJ, Wasserberger J, Ordog G. Phenytoin toxicity: A review of 94 cases. Vet Hum Toxicol. 1989;31:164–5. [PubMed] [Google Scholar]
- 8.Bajpai M, Roskos LK, Shen DD, Levy RH. Roles of cytochrome P4502C9 and cytochrome P4502C19 in the stereoselective metabolism of phenytoin to its major metabolite. Drug Metab Dispos. 1996;24:1401–3. [PubMed] [Google Scholar]
- 9.Kim KA, Park JY. Inhibitory effect of glyburide on human cytochrome p450 isoforms in human liver microsomes. Drug Metab Dispos. 2003;31:1090–2. doi: 10.1124/dmd.31.9.1090. [DOI] [PubMed] [Google Scholar]
- 10.Wit AL, Rosen MR, Hoffman BF. Electrophysiology and pharmacology of cardiac arrhythmias. VIII. Cardiac effects of diphenylhydantoin. B Am Heart J. 1975;90:397–404. doi: 10.1016/0002-8703(75)90331-2. [DOI] [PubMed] [Google Scholar]
- 11.Cacciapuoti F, Spiezia R, Bianchi U, Lama D, D’Avino M, Varricchio M. Effectiveness of glibenclamide on myocardial ischemic ventricular arrhythmias in non-insulin-dependent diabetes mellitus. Am J Cardiol. 1991;67:843–7. doi: 10.1016/0002-9149(91)90617-t. [DOI] [PubMed] [Google Scholar]
- 12.Nordin C. The proarrhythmic effect of hypoglycemia: Evidence for increased risk from ischemia and bradycardia. Acta Diabetol. 2014;51:5–14. doi: 10.1007/s00592-013-0528-0. [DOI] [PubMed] [Google Scholar]