

Description
Focused assessment with sonography in trauma (FAST) is now widely recognised as a mainstream emergency medicine technique in the management of trauma. The conventional areas that are screened for intraperitoneal blood following trauma include the hepatorenal interface (Morison's pouch), perisplenic space, pericardium and the pelvis. In the context of abdominal trauma, fluid or blood is indicated by the presence of black anechoic collections. The utility of FAST in solid organ evaluation is less clear. Historically, EM physicians have avoided (non-binary) qualitative comments on organ structure or disruption.
We report a case where FAST resulted in early diagnosis of splenic rupture, allowing for early institution of prophylactic anti-opportunistic postsplenectomy infection measures and urgent CT.
A gentleman in his 30s presented with blunt trauma to left lateral chest and abdomen. This occurred as a result of being thrown from a motorcycle in a motor-vehicle accident. On presentation, his haemodynamic vital signs were within normal parameters. He exhibited tenderness over the left anterolateral torso.
FAST revealed heterogeneous echogenicity of the spleen consistent with splenic haemorrhage (figures 1 and 2). CT confirmed ruptured spleen (figure 3) and the patient proceeded to laparotomy.
Figure 1.
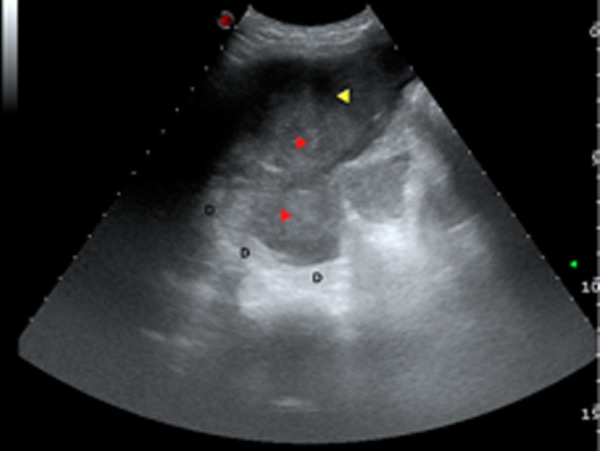
Heterogeneous echogenicity of acute haemorrhage. Red arrowheads shows hyperechoic areas and yellow arrowhead indicates hypoechoic areas. The curvilinear diaphragm is indicated by D.
Figure 2.
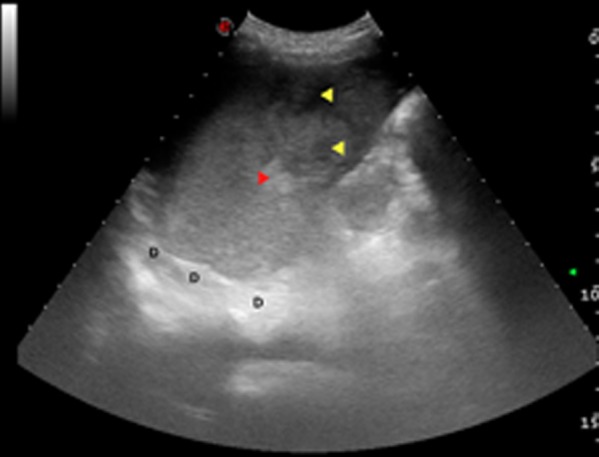
Heterogeneous echogenicity of splenic injury. Red arrowhead indicates hyperechoic area and yellow arrowheads indicate hypoechoic areas. Diaphragm is indicated by D.
Figure 3.

Coronal CT of splenic trauma. L, liver; S, spleen; K, kidney.
Splenic injury without sonographic haemoperitoneum has been frequently described and can occur in up to 29% 1–3 of cases. As emergency physicians’ proficiency in FAST becomes more refined, the subtle architectural and echogenic changes with various pathologies become more apparent. FAST practitioners should be aware of these (sometimes subtle) signs that have the potential to significantly alter and improve patient management.
Learning points.
Splenic injury without sonographic haemoperitoneum occurs in up to 29% of cases.
Normal splenic architecture exhibits homogeneous echogenicity on ultrasound.
Splenic heterogeneous echogenicity on FAST examination should suggest the possibility of severe splenic disruption.
Footnotes
Competing interests: None.
Patient consent: Obtained.
References
- 1.Boscak A, Shanmuganathan K. Splenic trauma: what is new? Radiol Clin North Am (Review) 2012;50:105–22. [DOI] [PubMed] [Google Scholar]
- 2.Shanmuganathan K, Mirvis SE, Sherbourne CD, et al. Hemoperitoneum as the sole indicator of abdominal visceral injuries: a potential limitation of screening abdominal US for trauma. Radiology 1999;212: 423–30. [DOI] [PubMed] [Google Scholar]
- 3.Chiu WC, Cushing BM, Rodriguez A, et al. Abdominal injuries without hemoperitoneum: a potential limitation of focused abdominal sonography for trauma (FAST). J Trauma 1997;42:617–23; discussion 23–5. [DOI] [PubMed] [Google Scholar]