

Abstract
Single-port access laparoscopic surgery has recently emerged as a method to improve morbidity and cosmetic benefit of conventional laparoscopic surgery. Herein, we report the experience of transumbilical incision laparoscopic sigmoidectomy with one assist port in a 71-year-old man who had developed recurrent sigmoid volvulus in these several years since his first visit to the hospital. The patient presented abdominal distension and severe constipation. A plain x-ray film and CT of the abdomen showed grossly distended sigmoid colon loops and stenosis of recto-sigmoid colon. Sigmoid volvulus associated with megacolon was diagnosed and emergence endoscopic decompression was performed. After his condition improved, transumbilical incision laparoscopic sigmoidectomy was carried out as the minimally invasive approach, due to the several risk of patient such as aging and pulmonary disorder. Postoperative course was uneventful and on postoperative visit to the hospital he reported resolution of abdominal distension.
Background
Sigmoid volvulus is a leading cause of acute colonic obstruction in South America, Africa, Eastern Europe and Asia. It is rare in developed countries such as the USA, UK, Japan and Australia.1 Unfortunately, mortality remains excessive for this type of colon obstruction.2 3 When diagnosis of primary sigmoid volvulus is confirmed, initial non-operative treatment should be acceptable when there are no compelling signs, and subsequent elective surgery following non-operative reduction is recommended.4 While there have been a number of surgical procedures to treat sigmoid volvulus after non-operative reduction,2 3 5 recent several reports have described that laparoscopy-assisted colectomy may be useful for sigmoid volvulus as minimally invasive surgery. Minimally invasive surgery for colon resections has already demonstrated benefits such as smaller abdominal incision, less postoperative pain, decreased length of stay and reduced surgical site infection over the conventional open technique.6 One possibility for reducing access surgery is a single port with multiple trocar channels introduced by a single incision through the umbilicus. Data already exist for this new approach to standard laparoscopic procedures such as cholecystecmomy,7 appendectomy8 and sleeve gastrectomy.9 In this article, we describe our treatment of a patient with umbilical incision laparoscopic sigmoid resection with one assist port during the same hospital stay. We believe that this is the first reported treatment of sigmoid volvules by an umbilical incision laparoscopic sigmoid resection.
Case presentation
A 71-year-old man with abdominal distension and severe constipation was referred to our hospital. He had a medical history of cerebral infarction 6 years earlier, resulting in a right hemiparesis. In these several years, he admitted to the hospital with the diagnosis of sigmoid volvulus and non-operative treatment was carried out several times. A plain x-ray of his abdomen showed grossly distended sigmoid colon loops, being the so-called coffee-bean sign (figure 1A) and stenosis of rectosigmoid colon by CT (figure 1B). The results of laboratory examinations were as follows: white blood cells 7700/mm3, haematocrit 43.3%. Other serum chemistries were within normal limits, except for high C reactive protein of 1.30 mg/dl (normal range within 0.3 mg/dl). Pulmonary functional tests results revealed mild air flow obstruction with forced expiratory volume in 1 s/forced vital capacity of 1.40/3.15 litre (predicted values were 2.57/3.38 litre). Sigmoid volvulus associated with megacolon was diagnosed and emergence colonoscopy was initially performed using endoscopy. The volvulus was successfully decompressed and derotated. Because the patient tolerated well and his general condition recovered after the endoscopic decompression, emergency surgery was avoided and an elective operation was scheduled. After discussion on the patient's concerns, laparoscopy-assisted colon resection was suggested without making the patient endure a large painful laparotomy incision. Before entering the surgery, the patients were well informed about the advantages and disadvantages of laparoscopic surgery. The patient was prepared for surgery with fasting and intravenous hyperalimentation to avoid recurrent intestinal torsion. In the operating room, the patient was placed in the lithotomy position. The 4 cm vertical umbilical incision was made referred to the technique described by Casciola et al10 and wound retractor (ALEXIS wound retractor XS; Applied Medical, Rancho Santa Margarita, California, USA) was adapted. Surgical glove was covered and a 12 mm umbilical port was placed through a glove finger, as well as parallel 5 mm ports (Tyco Healthcare, Mansfield, Mass, USA) in the same incision, then pneumoperitoneum was induced (figure 2A). A flexible laparoscopic camera (LTFVP, Olympus, Tokyo, Japan) is inserted via the middle finger port. On exploring abdomen, distended sigmoid colon, long loop and enlarged transverse colon were observed (figure 2B). Other areas of colon were not so dilated. To suspend and expose sigmoid colon, one additional 5 mm laparoscopic trocar and cannula was then inserted in the peritoneal cavity at the left lower quadrant under laparoscopic vision. The mesosigmoiditis was moderate, and there was mild adhesion to transverse mesocolon; however, it was viable and not twisted. Colorectal junction and sigmoid suspension and exposition were achieved by using an articulated grasper (Roticulator, Coviden, Norwalk, Connecticut, USA). The redundant sigmoid colon was mobilised by a laparoscopic lateral dissection sequence and was gently exteriorised. For the separation of the ligament and the mesocolon, we used the SonoSurg scissors (Olympus). The distended sigmoid colon was removed through the umbilical incision. Functional end-to-end gastrointestinal anastomosis-stapled anastomosis was established between the descending colon and sigmoid colon. Intraoperative anastomosis testing with air was satisfactory. Abdominal cavity was drained with a 19Fr J-Vac drain inserted from assistant 5 mm puncture incision. The resected segment of sigmoid colon measured 50 cm (figure 3). The operation time was 165 min and blood loss was 55 ml. Subsequent histological examination demonstrated hypertrophy of mucosal grand and neuroband. There was no aganglionic lesion, suggesting that the megacolon was thought to have been caused by her long history of severe constipation. The patient had an unremarkable postoperative course and was discharged on postoperative day 8. Figure 4 shows the completely healed scar at postoperative day 30.
Figure 1.
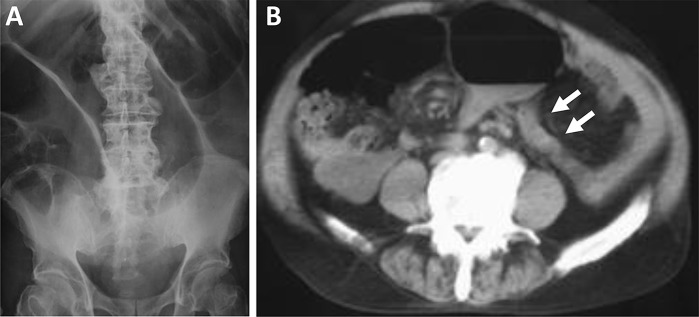
(A) Abdominal plain x-ray showing the ‘coffee-bean’ deformetry indicative of a distended sigmoid colon. (B) CT showing stenosis of rectosigmoid colon and distension of proximal sigmoid colon, indicating the torsion in this area.
Figure 2.
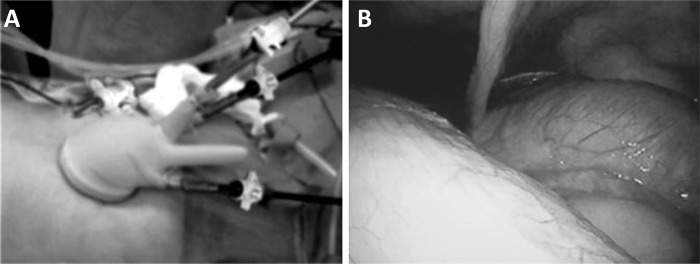
(A) Exterior view of umbilical laparoscopic surgery. We used an extrasmall wound retractor (ALEXIS wound retractor XS; Applied Medical, Rancho Santa Margarita, California, USA) and a surgical glove as a single port. The wound retractor was set-up through a small umbilical incision and the surgical glove attached with one 10 mm trocar and two 5 mm trocars was fixed to the outer ring of the wound retractor. (B) Intraoperative views of sigmoidectomy. Distended sigmoid colon, long loop and enlarged transverse colon were observed.
Figure 3.

Appearance of sigmoidectomy specimen.
Figure 4.
Postoperative view of the abdomen 4 weeks after surgery for a patient who underwent sigmoidectomy and ileorectal anastomosis.
Outcome and follow-up
During his postoperative recovery, the patient experienced remarkably little pain. On his postoperative visit to the hospital he reported resolution of abdominal distension and constipation.
Discussion
We show the first transumbilical sigmoidectomy with one assist port for sigmoid volvulus. Laparoscopic colectomy has been shown to facilitate patient recovery compared with open colorectal surgery.6
Attempts to minimise the surgical trauma and improve the cosmetic results of laparoscopic sigmoidectomy have illustrated the patient's satisfaction with these approaches.11 12 Recent reports have described that laparoscopic-assisted colectomy may be a useful alternative in high-risk patients or in the elderly who may not tolerate conventional colon surgery,13 14 and treating benign conditions laparoscopically is attractive as the surgeon does not have to worry about tumour clearance and resection margin unlike in malignant conditions. Patients’ preferences have stimulated attempts to develop safe ‘scarless’ surgical procedures. And the use of the umbilicus as the port in umbilical single-port access procedures shows a promise for future ‘scarless’ laparoscopic procedures.
The management of patients with intractable constipation who fail to respond to non-surgical intervention continues to represent a challenge for general and colorectal surgeons. When the diagnosis of sigmoid volvulus is made, deciding upon the most appropriate management option can be difficult. Unless there is clinical evidence of bowel gangrenosis and perforation at the time of diagnosis, non-operative decompression should be attempted initially.4 Although non-operative treatment by endoscopy has yielded good results, a high rate of recurrence ranging from 40% to 90% has been reported.3 15 Therefore, following non-operative decompression, elective surgery to reduce the risk of subsequent recurrence should be performed. Various surgical procedures for sigmoid volvulus have been described in the literature, including mesocolonoplasty, sigmoidectomy and subtotal colectomy.2 3 5 While Morrissey and Deroide16 advocated subtotal colectomy at the time of initial surgery for sigmoid volvulus with megacolon as the procedure of choice in patients, Mellor et al17 showed that sigmoid colectomy was the commonest employed and the recommended operation. We performed only sigmoidectomy, without any surgical procedure for the enlarged transverse colon considering several risks of the patient such as his age and pulmonary disorder. However, our patient will need to be followed up carefully to observe for any signs of recurrence of the volvulus.
In this article, we tried reduced port access sigmoidectomy because patient had several preoperative complications. This approach was almost successfully completed only with one assist port to grasp the distended sigmoid colon, which was useful for keeping a better laparoscopic view. To the best of our knowledge, this is the first report describing the reduced port surgery for a patient with recurrent sigmoid volvulus. Transumbilical surgery should have the potential advantages for recurrent sigmoid volvulus, because we can select the same surgical procedure from umbilicus when it recurs. Furthermore, we can use one assist skin incision as the portion inserting an indwelling drain to confirm the leakage of anastmosis. Transumbilical sigmoidectomy is feasible using a combination of conventional straight and articulated laparoscopic instruments. This surgical procedure only reproduced a standard laparoscopic sigmoidectomy and the use of articulated instruments allows avoidance of other incisions or the use of transparietal sling suture for exposition. The umbilical incisional approach decreases parietal trauma, and offers better cosmesis and less risk of development of hernia compared with a standard laparoscopic one. Our patient who underwent surgery with a transumbilical access assisted one port was highly satisfied with the cosmetic outcome.
The umbilical incision laparoscopic surgery appears to be a promising alternative method for sigmoid resections to manage sigmoid volvulus.
Learning points.
When sigmoid volvulus is diagnosed, initial non-operative treatment should be acceptable and subsequent elective surgery is recommended.
This transumbilical surgical procedure only reproduced a standard laparoscopic sigmoidectomy and the use of articulated instruments allows avoidance of other incisions.
Selection of minimal surgery should be recommended for an elderly patient with high preoperative risk.
Footnotes
Competing interests: None.
Patient consent: Obtained.
References
- 1.Raveenthiran V, Madiba TE, Atamanalp SS, et al. Volvulus of the sigmoid colon. Colorectal Dis 2010;12(7 Online):e1–17. [DOI] [PubMed] [Google Scholar]
- 2.Ryan P. Sigmoid volvulus with and without megacolon. Dis Colon Rectum 1982;25:673–9. [DOI] [PubMed] [Google Scholar]
- 3.Bak MP, Boley SJ. Sigmoid volvulus in elderly patients. Am J Surg 1986;151:71–5. [DOI] [PubMed] [Google Scholar]
- 4.Chung YF, Eu KW, Nyam DC, et al. Seow-Choen F. Minimizing recurrence after sigmoid volvulus. Br J Surg 1999;86:231–3. [DOI] [PubMed] [Google Scholar]
- 5.Subrahmanyam M. Mesosigmoplasty as a definitive operation for sigmoid volvulus. Br J Surg 1992;79:683–4. [DOI] [PubMed] [Google Scholar]
- 6.Marohn MR, Hanly EJ, McKenna KJ, et al. Laparoscopic total abdominal colectomy in the acute setting. J Gastrointest Surg 2005;9:881–6; discussion 7. [DOI] [PubMed] [Google Scholar]
- 7.Tacchino R, Greco F, Matera D. Single-incision laparoscopic cholecystectomy: surgery without a visible scar. Surg Endosc 2009;23:896–9. [DOI] [PubMed] [Google Scholar]
- 8.Nguyen NT, Reavis KM, Hinojosa MW, et al. A single-port technique for laparoscopic extended stapled appendectomy. Surg Innov 2009;16: 78–81. [DOI] [PubMed] [Google Scholar]
- 9.Saber AA, El-Ghazaly TH, Dewoolkar AV, et al. Single-incision laparoscopic sleeve gastrectomy versus conventional multiport laparoscopic sleeve gastrectomy: technical considerations and strategic modifications. Surg Obes Relat Dis 2010;6:658–64. [DOI] [PubMed] [Google Scholar]
- 10.Casciola L, Codacci-Pisanelli M, Ceccarelli G, et al. A modified umbilical incision for specimen extraction after laparoscopic abdominal surgery. Surg Endosc 2008;22:784–6. [DOI] [PubMed] [Google Scholar]
- 11.Bucher P, Pugin F, Morel P. Single port access laparoscopic right hemicolectomy. Int J Colorectal Dis 2008;23:1013–16. [DOI] [PubMed] [Google Scholar]
- 12.Lacy AM, Delgado S, Rojas OA, et al. MA-NOS radical sigmoidectomy: report of a transvaginal resection in the human. Surg Endosc 2008;22:1717–23. [DOI] [PubMed] [Google Scholar]
- 13.Liang JT, Lai HS, Lee PH. Elective laparoscopically assisted sigmoidectomy for the sigmoid volvulus. Surg Endosc 2006;20:1772–3. [DOI] [PubMed] [Google Scholar]
- 14.Greene FL. Laparoscopic management of colorectal cancer. CA Cancer J Clin 1999;49:221–8. [DOI] [PubMed] [Google Scholar]
- 15.Ballantyne GH. Review of sigmoid volvulus: history and results of treatment. Dis Colon Rectum 1982;25:494–501. [DOI] [PubMed] [Google Scholar]
- 16.Morrissey TB, Deitch EA. Recurrence of sigmoid volvulus after surgical intervention. Am Surg 1994;60:329–31. [PubMed] [Google Scholar]
- 17.Mellor SG, Phillips RK. The aetiology and management of sigmoid volvulus in the UK: how much colon need be excised? Ann R Coll Surg Engl 1990;72:193–5. [PMC free article] [PubMed] [Google Scholar]