

Abstract
A 37-year-old woman presented with a chief complaint of fecoptysis since 1 month. She belongs to low socio-economic status. There was no history of pulmonary tuberculosis or trauma.With the help of radiological findings, the authors were able to establish this rare diagnosis ‘right-sided diaphragmatic hernia complicated with broncho-pleuro-colonic fistula presenting as fecoptysis’. Diaphragmatic hernia is a common finding in day to day practice. Fistula between bowel loops and other viscera are also common entity, but fistula between pulmonary air-way passage and colon is a rare finding. Right-sided broncho-pleuro-colonic fistula is an extremely rare entity among these conditions.
Background
Fecoptysis is an uncommon symptom in adults which prompt us that there has to be a fistulous communication between bowel loop and air-way passage. Radiological modalities were favouring us that the lesion was on right side. We were able to demonstrate the fistulous tract between hepatic flexure and lower lobe bronchus. After extensive literature search, we found that such type of cases were least reported. Emphasis were given on the site of lesion, aetiology and presenting symptoms.Most of these type of cases were reported on the left side or communication with stomach and air way passage. Our case is unique which is on the right side and aetiology is different and not yet reported in literature to the best of our knowledge.
Case presentation
A 37-year-old woman of low socio-economic status, presented with chief complaint of fecoptysis since 1 month. There was no history of pulmonary tuberculosis or trauma. On examination, she was afebrile. Mild tenderness was observed over right chest wall. On auscultation breath sound were markedly decreased on the right side as compared to the left side. She was advised to take blood test including complete haemogram, plain abdominal-chest x-ray and barium meal follow through.
Erythrocyte sedimentation rate (Westergren method) was mildly raised to ~30 mm/first hour. Haemoglobin was decreased (~7 gm/dl). Eosinophil count was mildly raised (~7% ). These were the only positive results in blood test. Three consecutive sputum smears were negative for Mycobacterium tuberculosis.
Investigations
Plain radiograph of abdomen and chest revealed raised right dome of diaphragm (>3 cm ) as compared to left dome. Right hemithorax was with air-bronchogram in right mid-zone and speckled calcific foci in right side of abdomen and chest suggesting faecolith (figure 1). Barium meal follow through examination revealed ascending migration of hepatic flexure and abnormal communication with pleural cavity and right lower lobe bronchus (figure 2). At same sitting plain computed axial tomography of patient was performed and reformatted image revealed raised right dome of diaphragm and communication of hepatic flexure with right lower lobe bronchus through focal defect in right dome (figure 3).
Figure 1.

Plain radiograph of abdomen including chest revealed raised right dome of diaphragm with opaque right hemithorax with air-bronchogram in right mid-zone with speckled calcific foci in right side of the abdomen and chest probably suggesting faecolith.
Figure 2.
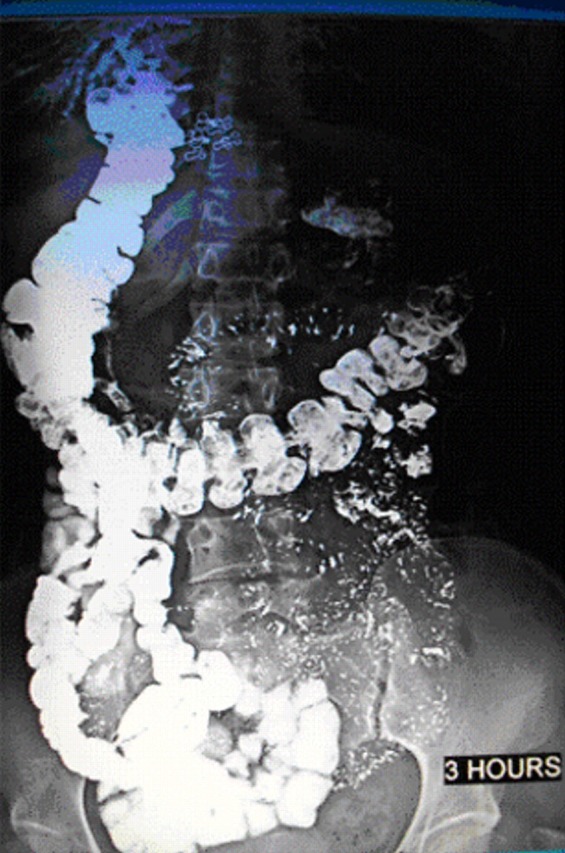
Barium meal follow through examination revealed-ascending migration of hepatic flexure and abnormal communication with pleural cavity and right lower lobe bronchus.
Figure 3.

Plain computed axial tomography of the patient was performed and reformatted image revealed raised right dome of diaphragm with communication of hepatic flexure with right lower lobe bronchus through focal defect in right dome of diaphragm.
Differential diagnosis
-
▶
Pulmonary tuberculosis
-
▶
Crohn’s disease
-
▶
Trauma.
Treatment
Surgical closure of fistulous tract and ligation of lower lobe bronchus/lower lobe resection.
Outcome and follow-up
Definite management was not yet done.
Discussion
Extensive thorough search of literature revealed only three cases of right-sided broncho-pleuro-colonic fistula. Common aetiology of broncho-colonic fistula was trauma. However Crohn’ disease, subphrenic abscess, empyema and ruptured liver abscess were another reasons causing fistula between pulmonary airways and colon. Traumatic rupture of the diaphragm with subsequent herniation of the colon may be frequently encountered but in the absence of infection, it would seem that fistula formation is an extremely rare entity.4 5
Learning points.
-
▶
Patient presenting with fecopytysis, must think about fistula between bowel and airway passage.
-
▶
Common aetiology of broncho-pleuro-colonic fistula are very few (a) trauma, (b) Crohn’s disease, (c) diaphragmatic hernia and (e) infection.
-
▶
Avoid barium meal follow through study with water soluble iodinated contrast media in this type of cases to avoid pulmonary oedema.
-
▶
This would be first case reported in literature to the best of our knowledge.
Footnotes
Competing interests: None.
Patient consent: Obtained.
References
- 1.Cecconi F. Arch Ital Chir (Bologna) 1958;2:84. [PubMed] [Google Scholar]
- 2.Edmunds LH, Williams GM, Welch CE. External fistulas arising from the gastrointestinal tract. Ann Surg 1960;152:445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Keeley JL, Campbell TA. Duodenobronchofistula: with a summary of abdominothoracic fistulas. J Thoracic Cardiovasc Surg 1960;39:538. [PubMed] [Google Scholar]
- 4.Domej W, Kullnig P, Petritsch W, et al. Colobronchial fistula: a rare complication of Crohn’s colitis. J R Soc Med 2001;94:258–9. [DOI] [PubMed] [Google Scholar]
- 5.Irving M. Colo-broncho-cutaneous fistula complicating traumatic diaphragmatic rupture. J R Soc Med 2001;94:258–9. [DOI] [PMC free article] [PubMed] [Google Scholar]