

Abstract
Vitamin D deficiency is common and may contribute to osteopenia, osteoporosis and falls risk in the elderly. Screening for vitamin D deficiency is important in high-risk patients, especially for patients who suffered minimal trauma fractures. Vitamin D deficiency should be treated according to the severity of the deficiency. In high-risk adults, follow-up serum 25-hydroxyvitamin D concentration should be measured 3–4 months after initiating maintenance therapy to confirm that the target level has been achieved. All patients should maintain a calcium intake of at least 1,000 mg for women aged ≤ 50 years and men ≤ 70 years, and 1,300 mg for women > 50 years and men > 70 years.
Keywords: elderly, osteoporosis, vitamin D
Madam Fatimah walked into your consultation room with the aid of a single point stick. She was there for a review following a left hip fracture that was treated surgically with open reduction and internal fixation 12 weeks ago. You reviewed her hospital records through your National Electronic Health Record account and noted that her last serum 25-hydroxyvitamin D [25(OH)D] test, which had been done in hospital, had found a 25(OH)D level of < 5 µg/mL with normal calcium levels and kidney function. You noted that she was started on the bisphosphonate Fosamax at 70 mg/wk.
HOW COMMON IS THIS IN MY PRACTICE?
Vitamin D deficiency in the elderly population
Vitamin D deficiency is common among elderly patients in temperate countries, especially in early spring due to reduced cutaneous synthesis during the winter months,(1,2) and in housebound individuals(3) and medical inpatients.(4) The prevalence of vitamin D deficiency is even higher in elderly patients with fragility fractures, ranging from 55%–91.6%.(5-7) A recent local study in Singapore showed a vitamin D deficiency prevalence of 57.5% and vitamin D insufficiency of 34.5% in elderly patients admitted to hospital with hip fractures.(8)
Consequences of vitamin D deficiency
Vitamin D deficiency results in abnormalities in calcium, phosphorus and bone metabolism. Specifically, it causes a decrease in the efficiency of intestinal calcium and the phosphorus absorption of dietary calcium and phosphorus, resulting in an increase in parathyroid levels.(9,10) In secondary hyperparathyroidism, serum calcium is maintained at the normal range at the expense of mobilising calcium from the skeleton and increasing phosphorus wasting in the kidneys. This process causes a generalised decrease in bone mineral density, resulting in osteopenia and osteoporosis. The secondary hyperparathyroidism also causes phosphaturia, which results in a low or low-normal serum phosphorus level. This leads to inadequate calcium-phosphorus levels and a mineralisation defect in the skeleton. In young children with little mineral in their skeleton, this defect results in rickets. In adults, the result is osteomalacia. Quantified by bone mineral density scores, osteomalacia presents symptomatically with isolated or generalised aches and pains in bones and muscles.(11) In the elderly, vitamin D deficiency causes increasing sway and frequent falls,(12,13) increasing the risk of fracture. In addition to improvements in bone density and the prevention of falls and fracture, vitamin D may have several other putative benefits, including beneficial effects on the immune and cardiovascular systems.(14)
Some risk factors
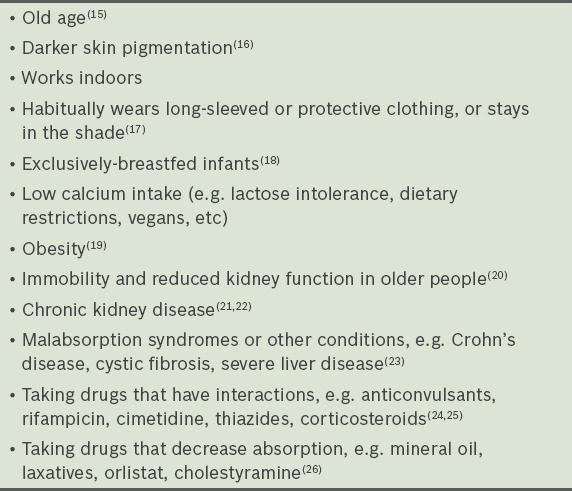
Table I shows some common risk factors for vitamin D deficiency in the general population. For the elderly in Singapore, being housebound and of Malay ethnicity is significantly associated with vitamin D deficiency. In a recent study, 90.5% of the Malay patients had a vitamin D level of less than 20 µg/mL compared to 55.0% of the Chinese patients.(8) Those at risk of vitamin D deficiency may be able to overcome it by increasing their exposure to sunlight or dietary intake of vitamin D. In children and adults, exposing the hands, face and arms to the sun for 10–15 minutes per day is usually sufficient. However, the amount of vitamin D that is produced from sunlight depends on the time of day, geographic location and the colour of one’s skin. Vitamin D can also be obtained from food and dietary supplements. However, sources in food are limited and include oily fish such as salmon, sardines and mackerel, fortified foods such as margarine, dairy products and cereals, as well as eggs and liver. As vitamin D production in skin and from dietary intake varies among individuals, some patients require vitamin D supplementation.
Table I.
Common risk factors for vitamin D deficiency.
WHAT CAN I DO IN MY PRACTICE?
Screen for vitamin D deficiency in high-risk populations. In this vignette, the population consists of elderly patients with a history of fragility fractures. Fig.1 shows the decision-making process for vitamin D screening, as adapted from Australian clinical practice guidelines.(27)
Ensure that patients on antiosteoporosis treatment have adequate vitamin D replacement. Vitamin D replacement regimes may differ according to the severity of the patient’s deficiency and tolerability of the medication.
Retesting of vitamin D levels is advisable three months after commencing of supplementation.
Fig. 1.
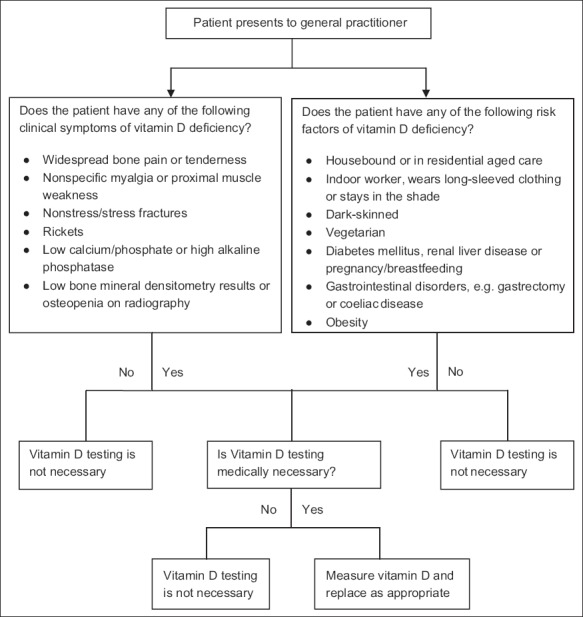
Flow chart shows the decision-making process for vitamin D screening.
Classifying and treating vitamin D deficiency
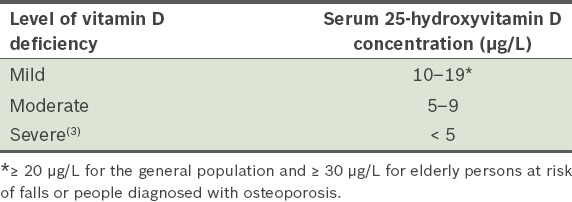
Classifying the severity of a patient’s vitamin D deficiency helps the physician to customise an appropriate replacement regimen (Table II).
Table II.
Severity of vitamin D deficiency.
Who should be treated with vitamin D supplementation
Vitamin D supplementation is recommended in people who have a confirmed vitamin D deficiency [25(OH)D < 30 µg/L].
Treatment targets and frequency of review
Serum 25(OH)D concentration should be maintained at ≥ 20 µg/L in the general population and ≥ 30 µg/L in elderly persons at risk of falls or people diagnosed with osteoporosis. When initiating treatment for vitamin D deficiency/insufficiency or changing the dose, serum 25(OH)D typically should not be measured again for at least three months; this allows it to reach a steady state. After reaching the desired vitamin D concentration, no further testing is needed unless risk factors change. More frequent monitoring is required for patients with intestinal malabsorption who require high-dose oral therapy.
Regimens
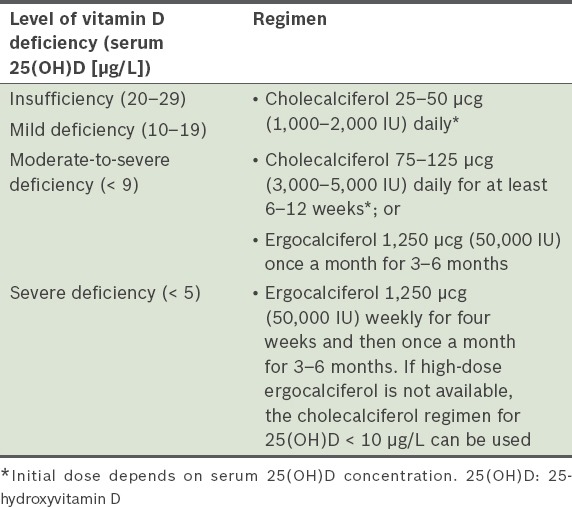
Oral vitamin D supplements are available in vitamin D3 (cholecalciferol) or vitamin D2 (ergocalciferol) forms. Cholecalciferol, rather than ergocalciferol, is suggested when it is available. All patients should maintain a daily calcium intake of 1,300 mg (particularly older people in institutions), since the combination of calcium and vitamin D prevents fractures. Table III lists the recommended treatment regimens. Physicians should wait at least three months before checking the patient’s serum 25(OH)D concentration again and should change to the therapy for mild vitamin D deficiency when the level rises to 10–19 µg/L. Most patients need ongoing treatment at the lower dose of cholecalciferol (i.e. 1,000 IU) daily.
Table III.
Treatment for vitamin D deficiency or insufficiency.
WHEN SHOULD I REFER TO A SPECIALIST?
Referral should be considered when high doses of vitamin D are required in patients with special medical circumstances, including:
Patients with a history of gastrectomy, fat malabsorption or those who require high, ongoing doses of vitamin D replacement due to underlying medical conditions.
Patients presenting with rare cases of rickets or osteomalacia, e.g. X-linked hypophosphataemic rickets, vitamin D-dependent rickets, tumour-induced soteomalacia and renal osteodystrophy. These patients may need complex therapeutic regimens that include calcitriol.
You started Madam Fatimah on cholecalciferol and did a repeat 25(OH)D test four months after her vitamin D replacement. You were happy to see her walking into your consultation room without any walking aids and encouraged her to continue regular brisk walking. You wrote a quick memo to update her attending orthopaedic surgeon at her next review.
TAKE HOME MESSAGES
Vitamin D deficiency is common and may contribute to osteopenia and osteoporosis and falls risk in the elderly.
It is important to screen for vitamin D deficiency in high-risk patients, especially after a minimal-trauma fracture.
Vitamin D deficiency should be treated according to the severity of the deficiency and the availability of vitamin D preparations in the community.
In high-risk adults, follow-up 25(OH)D measurements should be made 3–4 months after initiating maintenance therapy to confirm that the target level has been achieved.
All patients should maintain a calcium intake of at least 1,000 mg for women aged ≤ 50 years and men ≤ 70 years, and 1,300 mg for women > 50 years and men > 70 years.
REFERENCES
- 1.Looker AC, Dawson-Hughes B, Calvo MS, Gunter EW, Sahyoun NR. Serum 25-hydroxyvitamin D status of adolescents and adults in two seasonal subpopulations from NHANES III. Bone. 2002;30:771–7. doi: 10.1016/s8756-3282(02)00692-0. [DOI] [PubMed] [Google Scholar]
- 2.Nurmi I, Kaukonen JP, Lüthje P, et al. Half of the patients with an acute hip fracture suffer from hypovitaminosis D: a prospective study in southeastern Finland. Osteoporos Int. 2005;16:2018–24. doi: 10.1007/s00198-005-1987-0. [DOI] [PubMed] [Google Scholar]
- 3.Lips P. Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone loss and fractures and therapeutic implications. Endocr Rev. 2001;22:477–501. doi: 10.1210/edrv.22.4.0437. [DOI] [PubMed] [Google Scholar]
- 4.Thomas MK, Lloyd-Jones DM, Thadhani RI, et al. Hypovitaminosis D in medical inpatients. N Engl J Med. 1998;338:777–83. doi: 10.1056/NEJM199803193381201. [DOI] [PubMed] [Google Scholar]
- 5.Moniz C, Dew T, Dixon T. Prevalence of vitamin D inadequacy in osteoporotic hip fracture patients in London. Curr Med Res Opin. 2005;21:1891–4. doi: 10.1185/030079905X75023. [DOI] [PubMed] [Google Scholar]
- 6.Beringer T, Heyburn G, Finch M, et al. Prevalence of vitamin D inadequacy in Belfast following fragility fracture. Curr Med Res Opin. 2006;22:101–5. doi: 10.1185/030079906X80332. [DOI] [PubMed] [Google Scholar]
- 7.LeBoff MS, Kohlmeier L, Hurwitz S, Franklin J, Wright J, Glowacki J. Occult vitamin D deficiency in postmenopausal US women with acute hip fracture. JAMA. 1999;281:1505–11. doi: 10.1001/jama.281.16.1505. [DOI] [PubMed] [Google Scholar]
- 8.Ramason R, Selvaganapathi N, Ismail NH, et al. Prevalence of vitamin d deficiency in patients with hip fracture seen in an orthogeriatric service in sunny singapore. Geriatr Orthop Surg Rehabil. 2014;5:82–6. doi: 10.1177/2151458514528952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Holick MF, Siris ES, Binkley N, et al. Prevalence of Vitamin D inadequacy among postmenopausal North American women receiving osteoporosis therapy. J Clin Endocrinol Metab. 2005;90:3215–24. doi: 10.1210/jc.2004-2364. [DOI] [PubMed] [Google Scholar]
- 10.Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357:266–81. doi: 10.1056/NEJMra070553. [DOI] [PubMed] [Google Scholar]
- 11.Plotnikoff GA, Quigley JM. Prevalence of severe hypovitaminosis D in patients with persistent, nonspecific musculoskeletal pain. Mayo Clin Proc. 2003;78:1463–70. doi: 10.4065/78.12.1463. [DOI] [PubMed] [Google Scholar]
- 12.Bischoff-Ferrari HA, Willett WC, Wong JB, et al. Fracture prevention with vitamin D supplementation: a meta-analysis of randomized controlled trials. JAMA. 2005;293:2257–64. doi: 10.1001/jama.293.18.2257. [DOI] [PubMed] [Google Scholar]
- 13.Bischoff-Ferrari HA, Dawson-Hughes B, Staehelin HB, et al. Fall prevention with supplemental and active forms of vitamin D: a meta-analysis of randomised controlled trials. BMJ. 2009;339:b3692. doi: 10.1136/bmj.b3692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96:1911–30. doi: 10.1210/jc.2011-0385. [DOI] [PubMed] [Google Scholar]
- 15.Durvasula S, Kok C, Sambrook PN, et al. Sunlight and health: attitudes of older people living in intermediate care facilities in southern Australia. Arch Gerontol Geriatr. 2010;51:e94–9. doi: 10.1016/j.archger.2010.01.008. [DOI] [PubMed] [Google Scholar]
- 16.Springbett P, Buglass S, Young AR. Photoprotection and vitamin D status. J Photochem Photobiol B. 2010;101:160–8. doi: 10.1016/j.jphotobiol.2010.03.006. [DOI] [PubMed] [Google Scholar]
- 17.Linos E, Keiser E, Kanzler M, et al. Sun protective behaviors and vitamin D levels in the US population: NHANES 2003-2006. Cancer Causes Control. 2012;23:133–40. doi: 10.1007/s10552-011-9862-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Thandrayen K, Pettifor JM. Maternal vitamin D status: implications for the development of infantile nutritional rickets. Endocrinol Metab Clin North Am. 2010;39:303–20. doi: 10.1016/j.ecl.2010.02.006. [DOI] [PubMed] [Google Scholar]
- 19.Wortsman J, Matsuoka LY, Chen TC, Lu Z, Holick MF. Decreased bioavailability of vitamin D in obesity. Am J Clin Nutr. 2000;72:690–3. doi: 10.1093/ajcn/72.3.690. [DOI] [PubMed] [Google Scholar]
- 20.Oudshoorn C, van der Cammen TJ, McMurdo ME, van Leeuwen JP, Colin EM. Ageing and vitamin D deficiency: effects on calcium homeostasis and considerations for vitamin D supplementation. Br J Nutr. 2009;101:1597–606. doi: 10.1017/S0007114509338842. [DOI] [PubMed] [Google Scholar]
- 21.Patel S, Barron JL, Mirzazedeh M, et al. Changes in bone mineral parameters, vitamin D metabolites, and PTH measurements with varying chronic kidney disease stages. J Bone Miner Metab. 2011;29:71–9. doi: 10.1007/s00774-010-0192-1. [DOI] [PubMed] [Google Scholar]
- 22.Williams S, Malatesta K, Norris K. Vitamin D and chronic kidney disease. Ethn Dis. 2009;19(4 Suppl 5) S5-8-11. [PMC free article] [PubMed] [Google Scholar]
- 23.Lo CW, Paris PW, Clemens TL, Nolan J, Holick MF. Vitamin D absorption in healthy subjects and in patients with intestinal malabsorption syndromes. Am J Clin Nutr. 1985;42:644–9. doi: 10.1093/ajcn/42.4.644. [DOI] [PubMed] [Google Scholar]
- 24.Kennel KA, Drake MT, Hurley DL. Vitamin D deficiency in adults: when to test and how to treat. Mayo Clin Proc. 2010;85:752–7. doi: 10.4065/mcp.2010.0138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Wang S. Epidemiology of vitamin D in health and disease. Nutr Res Rev. 2009;22:188–203. doi: 10.1017/S0954422409990151. [DOI] [PubMed] [Google Scholar]
- 26.Sohl E, van Schoor NM, de Jongh RT, de Vries OJ, Lips P. The impact of medication on vitamin D status in older individuals. Eur J Endocrinol. 2012;166:477–85. doi: 10.1530/EJE-11-0917. [DOI] [PubMed] [Google Scholar]
- 27.Australian Department of Health. Vitamin D Testing Review Report (MBS Review) [Accessed May 20, 2015]. Available at: http://www.msac.gov.au/internet/msac/publishing.nsf/Content/932329F88F2367D3CA257D77008073B9/$File/Vitamin%20D%20testing%20Review%20Report-accessible.pdf .