

Abstract
The purpose of the present study was to investigate the potential associations of binge drinking detected at the exit of nightclubs and risk behaviors and alcohol effects just after leaving the venue in a representative sample of Brazilian nightclub patrons according to sex. For this purpose, a portal survey study called Balada com Ciência was conducted in 2013 in the megacity of São Paulo, Brazil, using a two-stage cluster sampling survey design. Individual-level data were collected in 2422 subjects at the entrance and 1822 subjects at the exit of 31 nightclubs, and breath alcohol concentration (BrAC) was measured using a breathalyzer. The following day, 1222 patrons answered an online follow-up survey that included questions about risk behaviors and alcohol effects practiced just after leaving the nightclub. Weighted logistic regressions were used to analyze binge drinking associated with risk behaviors by sex. For both sexes, the most prevalent risk behaviors practiced after leaving a nightclub were drinking and driving (men=27.9%; women=20.4%), the use of illicit drugs (men=15.8%; women=9.4%) and risky sexual behavior (men=11.4%; women=6.8%). The practice of binge drinking increased the behavior of illicit drug use after leaving the nightclub by 2.54 times [95% CI: 1.26-5.09] among men who drank and increased the risk of an episode of new alcohol use by 5.80 times [95% CI: 1.50-22.44] among women who drank. Alcoholic blackouts were more prevalent among men [OR=8.92; 95% CI: 3.83-20.80] and women [OR= 5.31; 95% CI: 1.68-16.84] whose BrAC was equivalent to binge drinking compared with patrons with a lower BrAC. Public policies aiming to reduce patrons’ BrAC at the exit of nightclubs, such as staff training in responsible beverage service and legislation to prevent alcohol sales to drunk individuals, would be useful to protect patrons from the risk behaviors associated with binge drinking in nightclubs.
Introduction
Alcohol consumption is a well-known cause of morbidity, mortality and social damage around the world and is a major component of the global burden of disease, particularly in the Americas and Europe [1, 2]. Compared with the other most populous countries, Brazil is ranked as having the second highest rate of major complications resulting from alcohol consumption, according to disability-adjusted life years lost [3].
Noteworthy is the fact that the severity of the consequences of alcohol consumption depends on the frequency of consumption and the quantities consumed [4]. A standard pattern of risky consumption that has aroused international interest and only recently began to be investigated in Brazil is called "binge drinking" (BD) [5] or "heavy episodic drinking" [6]. This pattern is usually characterized by the use of at least four doses of alcohol on a single occasion for women and five doses for men, which leads to an ethanol concentration in the blood of 0.08% or higher [7]. The regulation of the four drink cutoff for women was defined based on women’s lower rate of metabolism for alcohol, which leads to higher blood alcohol levels compared with men for the same quantity of alcohol [8]. However, the BD definition is controversial and permeated by the conceptualization of conflicts, which are influenced by the culture of the use and pharmacokinetic aspects of alcohol [9, 10]. These episodes of acute alcohol abuse not only have an influence on overall mortality but also contribute to acute consequences, particularly accidents [11] and violence [12], thus endangering the intoxicated and the community. BD is associated with higher rates of sexual abuse, suicide attempts, unprotected sex, unwanted pregnancies, alcohol overdose, falls, gastritis and pancreatitis [13].
However, it has been emphasized that there are clear gender differences regarding the effects of alcohol [14]. Men are consistently more than twice as likely as women to report episodes of alcohol intoxication and alcoholism [15–19]. However, after fewer years of heavy drinking, alcoholic women are more likely than men to develop cirrhosis [20], alcohol-induced damage of the heart muscle [21] and nerve damage [22]. Finally, the metabolism of alcohol is affected by the body’s amount of water and fat, which are responsible for the difference in the number of doses that define an episode of binge drinking for men and women [14].
Binge drinking occurs mostly in recreational settings, such as nightclubs [23]. Nightclubs are places attended mostly by youth and young adults that seek different forms of entertainment at these venues, in which the use of alcohol and other drugs act as important mediators [24]. However, they are also places where breaking social rules is tolerated and pleasure is stimulated [25], which contributes to a higher exposure of patrons to risks [26]. International findings show that the excessive consumption of alcohol in nightclubs and bars is associated with more episodes of physical aggression [27], sexual risk behaviors [28] and sexual violence [29] in these establishments and traffic accidents [30] on the way to or back from the venue.
In Brazil, one study reported that 40% of young people (18–24 years) engaged in BD at least once in the 12 months preceding the survey, and nightclubs are the places of choice for this practice [31]. Among teenage high school students in this country, the picture is even more alarming, with 35% of high school students in one study reporting engaging in BD in the month preceding the survey; again, nightclubs are the location of choice for this practice [32].
It is noteworthy that most of the literature concerning the consequences of binge drinking in nightclubs is restricted to risky behaviors that occur within the venue. However, considering that patrons leave the venues with high alcoholic concentrations [33], the consequences of alcoholic intoxication can also be evaluated and noted in the behavior practiced just after leaving the establishment, offering important results for the development of public policies. Thus, the objectives of this paper were 1) to describe the frequency of risk behaviors practiced by nightclub patrons just after the departure from the venues and 2) to identify possible associations between the occurrence of these events and of alcohol effects with the standard binge drinking values (breath alcohol concentration ≥ 0.38 mg/L) measured on the breath of this population when exiting these establishments, according to the sex of the patrons.
Materials and Methods
Sampling
This study was a two-stage cluster sampling portal survey among nightclub patrons interviewed at the entrance and exit of nightclubs and the following day. The first stage consisted of a systematic sample of nightclubs with a selection probability proportional to the nightclub’s maximum capacity. The second stage was a systematic sampling of every third person in the entrance line of the nightclubs. Data were collected during the first semester of 2013 in the city of São Paulo, Brazil.
For the selection of the venues, nightclubs were defined as leisure venues that sell alcoholic beverages, have one or more dance floors, and offer individual control of patron entry and exit through the payment of an entrance fee. The nightclub frame list was created by an active search of magazines and guides specializing in leisure activities and a search of the first ten pages returned from a Google search using the following key words: ‘São Paulo bars, nightclubs and discos’ (in Portuguese). The final frame list consisted of 150 nightclubs meeting the inclusion criteria, from which 40 nightclubs and potential replacements were chosen [34].
A sample size of 1600 patrons was calculated so that the prevalence of alcohol intoxication could be estimated to within 5 percentage points (absolute precision) of the true value set to 50% (maximum variance) with 95% confidence with two stages of cluster sampling and a design effect of 2 [35]. Taking into account a refusal rate of 30% and a maximum follow-up loss of 40% from patron entrance to patron exit, which was based on previous studies by Clapp et al. [36], it was determined that 2912 patrons should be initially approached. The adopted inclusion criteria were the intention to enter the nightclub and being at least 18 years old. In the case of refusal, data on age and sex were registered, and the next person in line was approached.
Details on the sample weights calculated from non-response and post-stratification are described in Carlini et al. [37].
Data collection and instruments
The selected patrons who agreed to participate in the study answered a questionnaire on sociodemographic variables, the practice of pre-drinking, alcohol use patterns, drug use, and other risk behaviors in nightclubs in the past 12 months prior to the interview. The patrons also had their breath alcohol concentrations (BrAC) measured at the time of the interview by means of a breathalyzer (calibrated Draguer Alcoltest 7410 plus RS), and each patron received a bracelet with a unique numeric code for identification at the time of nightclub exit. At the nightclub exit line, the same participating patrons—identified by their bracelets—were approached once more and invited to answer another questionnaire regarding the use of alcohol, illicit drugs and other risk behaviors they could have engaged in while inside the nightclub. At the end of the exit interview, breath alcohol concentration was measured once more. Additionally, a project folder containing information regarding the post-nightclub questionnaire that would be sent by e-mail the next day was handed to the participants.
On the day after the nightclub interview, the link to the online post-nightclub questionnaire was sent by e-mail to the interviewees who had answered the questionnaire in the entrance line of the nightclub 12 hours before. The first module consisted of questions regarding patron risk behaviors after exiting the nightclub, and the second module consisted of questions from the AUDIT, which served as a basis for the identification of high-risk groups and their randomization to participate in an electronic social norms intervention to reduce harmful drinking.
This manuscript presents the results for the first module of the online survey “behaviors after leaving the nightclub”, as dependent variables and the data from the exit BrAC (mg/L) and entrance interviews as independent variables. Fig 1 describes the flow of participants in the interviews of the study.
Fig 1. Flowchart for patron’s recruitment and data collection at three time points, “Balada com Ciência” Portal Survey, São Paulo, Brazil, 2013.

Variables
Dependent variables
To proceed with the analysis, the 40 binary (yes/no) questions about risk behaviors were grouped to create eight variables. Data on risk behaviors and alcohol effects were obtained from the interviewees’ responses to the online follow-up questionnaire. Six categories of risk behaviors were created: “drink and drive”; “illicit drug use after leaving”; “new alcohol use”; “violent behavior”; “accidents”; “sexual risk behavior”; and “policy involvement”. Two categories of alcohol effects identified after leaving the nightclub were created: “physical complications” and "blackout". All these variables were categorized as “no” or “yes”.
The variable “illicit drug use after leaving” included the use of at least one of the following substances: marijuana or hashish, cocaine, ecstasy, tobacco, crack, inhalants, ketamine, methamphetamine, other amphetamines, benzodiazepines or hallucinogens (such as LSD, mushrooms and peyote). The variable "violent behavior" included self-reported fights or arguments with family, fights or discussions with friends, colleagues or boyfriend/girlfriend, or fights or arguments with strangers, and the suffering or practicing of physical assault and vandalism (e.g., stealing traffic signs, plundering). "Accidents" included "I suffered a car accident" and "I suffered some other accident". The variable "sexual risk behavior" included the occurrence of sexual intercourse without a condom with a steady partner, sexual intercourse without a condom with a casual partner, the occurrence of sexual intercourse in which there was regret and sexual intercourse against their will. “Physical complications” included “vomited; felt physically bad; got sick” and “fainted”. The variable "blackout" included little or no memories of the period. When scoring any of these topics, the variable under which it was located was considered a case.
Independent variables
The following socio-demographic variables were also analyzed: age (18–24, 25–34, 35–44, 45+); marital status (single, married, others); and education (middle school, high school, college, graduation). Socioeconomic status (SES) was evaluated as indexed in relation to a highly standardized Brazilian survey assessment of SES known as the Associação Brasileira de Empresas de Pesquisa (Brazilian Association of Research Agencies) index. This index is based on the education level of the head of the household, the possession of various types of household goods (e.g., television sets) and the number of housekeepers. This scale was used to sort participants into standardized subgroups labeled A–E (in which A was the highest economic strata). To facilitate the interpretation and improve the accuracy of estimates in the regression models, for the SES variable, the D and E classes were grouped together [38].
BrAC was measured with a breathalyzer test after each interview and categorized in the analysis into three groups: “non-drinker”, “BrAC 0.01–0.37 mg/L”, or “BrAC ≥0.38 mg/L”. Binge drinking was defined as a BrAC ≥0.38 mg/l, which corresponds to a blood alcohol concentration of 0.08% [(mean concentration for a binge drinking episode) [7, 39]. Except for the measure of BrAC, all other variables were self-reported.
BrAC is the main independent variable and risky behaviors are dependent variables in each logistic regression because binge drinking occurred before the risk behavior or alcohol effect (there is a temporal relationship between these variables.
Fig 2 describes the moment in which each of the variables used in the statistical analysis were collected and brings the variables used in the analysis of this manuscript (see S1 File).
Fig 2. Description of the 3 time points of data collection among nightclub patrons in the study “Balada com Ciência” Portal Survey, São Paulo, Brazil, 2013.
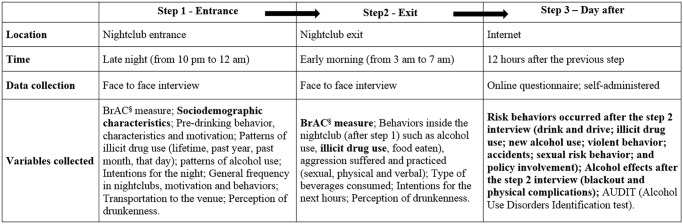
§BrAC—Breath alcohol concentration; Only the bold variables were used in the present analysis.
Statistical analysis
A descriptive analysis was conducted of the socio-demographic characteristics, BrAC measured at the exit of the nightclub, illicit drug use and risk behaviors according to sex. All the data are presented as proportions. The distribution of BrAC measured at the exit of the nightclub according to socio-demographic, illicit drug use and risk behavior characteristics was analyzed. Intergroup comparisons were performed using Pearson’s chi-square (χ2) test with the Rao-Scott correction [40]. The null hypothesis was rejected at a level of significance of 5%. The association between each risk behavior and BrAC was analyzed using logistic regression models stratified by sex, with a backward stepwise procedure. The reference categories for this analysis were “no driving”, “no illicit drug use”, “no new alcohol use”, “no violence behavior”, “no physical complication”, “no sexual risk behavior”, “no sexual assault”, “no physical discomfort”, “no policy involvement” and “no blackout”. To evaluate the possible effects of binge drinking BrAC measures at the exit of the nightclub on the occurrence of these risk behaviors just after leaving the venue, the models considered only drinkers (BrAC≥0.01 mg/L). The models were adjusted by age, marital status, education, socioeconomic status and illicit drug use (use of drugs concomitantly to alcohol use inside the nightclub: marijuana or hashish, cocaine, ecstasy, tobacco, crack, inhalants, ketamine, methamphetamine, other amphetamines, benzodiazepines or hallucinogens). These analyses were performed using the Stata statistical software package, version 13. In this model, the magnitude of the associations was estimated using odds ratios and their respective 95% CIs. The analysis incorporated weights to correct for the different selection probabilities of the participants, and the results are expressed as weighted values.
Ethical considerations
The Research Ethics Committee of the Universidade Federal de São Paulo (protocol 21477) approved this study. No interviews were conducted with patrons showing signs of severe intoxication, following the guidelines for screening described in Perham et al. [41].
Results
A total of 1222 individuals answered the 3 phases of the study (interview at the entrance and exit of the nightclub and the online questionnaire the following day). At the time of the interviews, the population of those surveyed corresponded to 5789 nightclub patrons of the city of São Paulo, Brazil. These patrons were primarily young (18–24 years old), single, middle to high social class and with high-school education completed for both sexes. Binge drinking BrAC levels at the exit were detected among 29.6% of the men and 22.1% of the women interviewed. As for risk behaviors, despite the low frequency of occurrence, men were usually exposed to a greater extent than women. The most prevalent risk behavior after leaving the nightclub for both sexes was drinking and driving (Table 1).
Table 1. Weighted distribution of sociodemographic characteristics, binge drinking, risk behaviors and alcohol effects after leaving a nightclub by sex among patrons in São Paulo, Brazil–“Balada com Ciência” portal survey (N = 1222).
| MEN | WOMEN | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| N = 694 | N = 528 | ||||||||
| Variables | Categories | Wg% # | Wgn & | Unwgn $ | Wg% # | Wgn & | Unwgn $ | p-value* | |
| Sociodemographics | Age | < = 24 | 48.8 | 1488 | 344 | 52.0 | 1426 | 281 | 0.355 |
| 25–34 | 36.8 | 1122 | 256 | 36.6 | 1003 | 182 | |||
| 35–44 | 9.9 | 301 | 68 | 10.6 | 290 | 60 | |||
| 45+ | 4.5 | 137 | 26 | 0.8 | 23 | 5 | |||
| Marital status | Single | 89.7 | 2757 | 632 | 86.5 | 2395 | 458 | 0.175 | |
| Married | 6.5 | 181 | 43 | 8.1 | 227 | 47 | |||
| Other | 3.8 | 103 | 17 | 5.4 | 112 | 21 | |||
| Education | Middle school | 2.5 | 26 | 19 | 2.9 | 12 | 17 | 0.508 | |
| High school | 52.3 | 603 | 361 | 55.8 | 480 | 295 | |||
| College | 36.0 | 2088 | 239 | 30.1 | 1950 | 159 | |||
| Graduation | 9.2 | 276 | 64 | 10.4 | 284 | 54 | |||
| Socioeconomic Status ¥ | A | 28.7 | 876 | 193 | 26.6 | 731 | 135 | 0.362 | |
| B | 55.8 | 1700 | 381 | 58.1 | 1592 | 311 | |||
| C | 14.3 | 440 | 114 | 14.0 | 385 | 74 | |||
| D/E | 1.1 | 32 | 6 | 1.3 | 34 | 8 | |||
| Inside the nightclub | Binge drinking § | Non-drinker | 41.5 | 1264 | 292 | 55.3 | 1514 | 285 | 0.076 |
| BrAC 0.01–0.37 mg/L | 28.9 | 880 | 197 | 22.6 | 618 | 124 | |||
| BrAC≥0.38 mg/L | 29.6 | 903 | 205 | 22.1 | 604 | 118 | |||
| Illicit drug use inside nightclub | Yes | 32.9 | 1002 | 226 | 22.1 | 605 | 116 | 0.002 | |
| After leaving the nightclub | Illicit drug use after leaving | Yes | 15.8 | 481 | 108 | 9.4 | 257 | 49 | 0.001 |
| Drink and drive | Yes | 27.9 | 850 | 194 | 20.4 | 558 | 98 | 0.032 | |
| New alcohol use | Yes | 9.2 | 281 | 67 | 7.1 | 194 | 37 | 0.221 | |
| Violent behavior | Yes | 3.8 | 117 | 33 | 2.8 | 78 | 16 | 0.358 | |
| Accidents | Yes | 1.0 | 29 | 8 | 0.7 | 18 | 3 | 0.597 | |
| Sexual risk behavior | Yes | 11.4 | 81 | 346 | 6.8 | 36 | 186 | 0.003 | |
| Policy involvement | Yes | 0.4 | 13 | 4 | 0.8 | 21 | 4 | 0.363 | |
| Physical complications | Yes | 7.4 | 224 | 50 | 9.4 | 257 | 43 | 0.432 | |
| Blackout | Yes | 9.7 | 297 | 72 | 8.1 | 223 | 40 | 0.507 | |
# Weighted proportions in percentage;
& Weighted sample size (data were weighted to be representative of the nightclubs in São Paulo, Brazil);
$ Sample size.
¥ Socioeconomic status classification by ABEP (ABEP, 2012).
* Rao-Scott chi-square test.
§ BrAC—Breath alcohol concentration.
Among the individuals who drank in the nightclubs, the sociodemographic characteristics, illicit drug use inside the venue, risk behaviors after leaving the nightclub and alcohol effects were compared according to the alcohol concentration in their breath at the exit and by sex, as shown in Tables 2 and 3. There were no sociodemographic differences in each alcoholic group (binge vs. non-binge) for both sexes. However, a trend of significance (p = 0.052) was noted for illicit drug use within the nightclub among women, i.e., women who presented an alcoholic dosage equivalent to the practice of binge drinking reported lower consumption of illegal drugs within the venue compared with women who drank but had lower BrAC measures (Table 2). Regarding the risk behaviors practiced after leaving the nightclub and the possible effects of alcohol, there was a higher proportion of illicit drug use after leaving, physical complications and blackout among men with a BrAC ≥0.38 mg/L compared with drinkers with lower alcoholic strengths. Among women, there was a higher prevalence of new episodes of alcohol use and blackout after leaving the nightclub among those with a BrAC ≥0.38 mg/L (Table 3).
Table 2. Weighted distribution of sociodemographic and drug use characteristics according to sex and BrAC measured at nightclub exits among patrons in São Paulo, Brazil–“Balada com Ciência” portal survey (N = 664 drinkers).
| MEN | WOMEN | ||||||
|---|---|---|---|---|---|---|---|
| BrAC § 0.01–0.37 mg/L | BrAC≥0.38 mg/L | BrAC 0.01–0.37 mg/L | BrAC≥0.38 mg/L | ||||
| (no binge drinking) | (binge drinking) | (no binge drinking) | (binge drinking) | ||||
| Variables | Categories | (N = 197) | (N = 205) | p-value* | (N = 124) | (N = 116) | p-value* |
| Age | < = 24 | 52.9 | 54.4 | 0.878 | 56.4 | 62.2 | 0.454 |
| 25–34 | 34.6 | 35.2 | 38.2 | 30.8 | |||
| 35–44 | 8.7 | 8.3 | 5.5 | 6.0 | |||
| 45+ | 3.8 | 2.1 | 0 | 1.0 | |||
| Marital status | Single | 90.6 | 94.9 | 0.400 | 94.4 | 93.3 | 0.833 |
| Married | 6.3 | 3.9 | 3.7 | 5.3 | |||
| Others | 3.1 | 1.2 | 1.9 | 1.5 | |||
| Education | Middle school | 3.2 | 2.1 | 0.892 | 3.7 | 4.2 | 0.181 |
| High school | 52.4 | 54.5 | 54.7 | 63.8 | |||
| College | 34.2 | 34.2 | 34.6 | 20.5 | |||
| Graduation | 10.3 | 9.2 | 7.0 | 11.5 | |||
| Socioeconomic Status ¥ | A | 33.9 | 30.5 | 0.253 | 24.7 | 23.0 | 0.496 |
| B | 51.2 | 57.7 | 62.8 | 58.5 | |||
| C | 14.9 | 10.7 | 11.9 | 16.5 | |||
| D/E | 0 | 1.1 | 0.6 | 2.0 | |||
| Illicit drug use inside nightclub | No | 66.4 | 57.8 | 0.120 | 81.4 | 67.6 | 0.052 |
| Yes | 33.6 | 42.2 | 18.6 | 32.4 | |||
Table 3. Weighted distribution of risk behaviors and alcohol effects after leaving a nightclub, according to sex and BrAC measured at nightclub exits among patrons in São Paulo, Brazil–“Balada com Ciência” portal survey (N = 664 drinkers).
| MEN | WOMEN | |||||||
|---|---|---|---|---|---|---|---|---|
| BrAC § 0.01–0.37 mg/L | BrAC≥0.38 mg/L | BrAC 0.01–0.37 mg/L | BrAC≥0.38 mg/L | |||||
| (no binge drinking) | (binge drinking) | (no binge drinking) | (binge drinking) | |||||
| Variables | Categories | (N = 197) | (N = 205) | p-value* | (N = 124) | (N = 116) | p-value* | |
| Risk behavior | Illicit drug use after leaving | Yes | 9.9 | 20.7 | <0.001 | 8.5 | 11.5 | 0.496 |
| Drink and drive | Yes | 20.6 | 14.9 | 0.105 | 10.7 | 8.8 | 0.602 | |
| New alcohol use | Yes | 11.8 | 10.8 | 0.718 | 3.4 | 17.7 | 0.005 | |
| Violent behavior | Yes | 3.6 | 5.3 | 0.442 | 3.7 | 5.9 | 0.449 | |
| Accidents | Yes | 0.9 | 1.1 | 0.853 | 1.1 | 0.5 | 0.507 | |
| Sexual risk behavior | Yes | 9.4 | 13.2 | 0.268 | 7.6 | 5.0 | 0.285 | |
| Policy involvement | Yes | 0.3 | 0.3 | 0.971 | 1.1 | 0.5 | 0.507 | |
| Alcohol effects | Physical complications | Yes | 4.3 | 14.1 | <0.001 | 9.5 | 16.6 | 0.122 |
| Blackout | Yes | 3.1 | 21.3 | <0.001 | 4.7 | 20.5 | <0.001 | |
* Rao-Scott chi-square test [40].
§ BrAC—Breath alcohol concentration.
The associations between each risk behavior practiced after leaving the nightclub by sex and according to the BrAC levels measured at the exit of the nightclub are presented in Tables 4 and 5. For both sexes, a BrAC ≥0.38 mg/L was positively associated with risk behaviors and/or alcohol effects, after adjusting for potentially confounding variables. Considering risk behaviors, the practice of binge drinking increased the behavior of illicit drug use after leaving the nightclub by 2.54 times [95% CI: 1.26–5.09] among men and increased the risk of a new episode of alcohol use by 5.80 times [95% CI: 1.50–22.44] among women. Physical complications and blackouts were more likely to be reported among men and women identified with a binge drinking measure. Among men, binge drinking increased the occurrence of physical complications by 3.51 times [95% CI: 1.96–6.30] and the occurrence of "blackout" by 8.92 times [95% CI: 3.83–20.80] in the adjusted models. For women, binge drinking increased the occurrence of physical complications by 2.40 times [95% CI: 1.20–4.70] and the occurrence of "blackout" by 5.31 times [95% CI: 1.68–16.84] in the adjusted models.
Table 4. Association between risk behaviors and alcohol effects after leaving a nightclub and binge drinking BrAC measure at nightclub exits among male patrons in São Paulo, Brazil—Balada com Ciência portal survey (N = 402 men drinkers).
| MEN BrAC≥0.38 mg/L § ** | |||||
|---|---|---|---|---|---|
| Variables* | UnOR (95% CI) | p-value | $ AdOR (95% CI) | p-value | |
| Risk behavior after leaving the nightclub | Illicit drug use after leaving | 2.36(1.46–3.82) | 0.001 | 2.54(1.26–5.09) | 0.010 |
| Drink and drive | 0.68(0.42–1.09) | 0.107 | 0.66(0.39–1.13) | 0.131 | |
| New alcohol use | 0.90(0.51–1.60) | 0.711 | 0.83(0.47–1.50) | 0.535 | |
| Violent behavior | 1.50(0.51–4.40) | 0.445 | 1.52(0.51–4.54) | 0.442 | |
| Accidents | 1.21(0.18–8.30) | 0.836 | 1.13(0.16–7.84) | 0.898 | |
| Sexual risk behavior | 1.47(0.73–3.00) | 0.270 | 1.50(0.76–2.97) | 0.237 | |
| Policy involvement | 0.94(0.50–17.65) | 0.971 | 0.97(0.05–18.9) | 0.983 | |
| Alcohol effects | Physical complications | 3.65(20.7–6.43) | <0.001 | 3.51(1.96–6.30) | <0.001 |
| Blackout | 8.50(3.74–19.16) | <0.001 | 8.92(3.83–20.80) | <0.001 | |
* Risk behaviors/alcohol effect were the dependent variables.
§ BrAC—Breath alcohol concentration.
** BrAC was the independent variable, considering no binge drinking as the reference (reference category = BrAC 0.01–0.37mg/L).
$ Final logistic model was adjusted by age, marital status, education, socioeconomic status and drug use inside the nightclub and the negative variables was references (e.g., no drink and drive, no new alcohol use, no accidents).
Table 5. Association between risk behaviors and alcohol effects after leaving a nightclub and binge drinking BrAC measures at nightclub exits among female patrons in São Paulo, Brazil—Balada com Ciência portal survey (N = 242 women drinkers).
| WOMEN BrAC≥0.38 mg/L § ** | |||||
|---|---|---|---|---|---|
| Variables* | UnOR (95% CI) | p-value | $ AdOR (95% CI) | p-value | |
| Risk behavior after leaving the nightclub | Illicit drug use after leaving | 1.39(0.52–3.74) | 0.498 | 0.64(0.18–2.44) | 0.535 |
| Drink and drive | 0.80(0.33–1.90) | 0.603 | 0.84(0.29–2.40) | 0.738 | |
| New alcohol use | 5.86(1.58–21.8) | 0.010 | 5.80(1.50–22.44) | 0.013 | |
| Violent behavior | 1.60(0.45–5.73) | 0.453 | 1.29(0.35–4.63) | 0.691 | |
| Accidents | 0.40(0.02–7.08) | 0.521 | 0.36(0.03–4.14) | 0.399 | |
| Sexual risk behavior | 0.63(0.26–1.51) | 0.289 | 0.61(0.28–1.35) | 0.215 | |
| Policy involvement | 0.40(0.03–7.10) | 0.521 | 0.36(0.03–4.14) | 0.399 | |
| Alcohol effects | Physical complications | 1.89 (0.82–4.33) | 0.126 | 2.40(1.20–4.70) | 0.015 |
| Blackout | 5.25(1.94–14.22) | 0.002 | 5.31(1.68–16.84) | 0.006 | |
* Risk behaviors/alcohol effect were the dependent variables.
§ BrAC—Breath alcohol concentration.
** BrAC was the independent variable, considering no binge drinking as the reference (reference category = BrAC 0.01–0.37mg/L).
$ Final logistic model was adjusted by age, marital status, education, socioeconomic status and drug use inside the nightclub and the negative variables was references (e.g., no drink and drive, no new alcohol use, no accidents).
Discussion
This study has evaluated the possible effects of a BrAC equivalent to binge drinking practices on risk behaviors among men and women at nightclub exits in Sao Paulo, Brazil. The results suggested that the prevalence of the practice of binge drinking was the same for both sexes. For men and women, the most prevalent risk behaviors practiced after leaving a nightclub were drinking and driving, the use of illicit drugs and risky sexual behavior. Concerning the harmful effects of alcohol, blackout episodes after leaving the nightclub were reported for nearly 10% of the patrons of these venues. In addition, men and women who practiced binge drinking were more likely to report episodes of blackout and physical complications of alcohol consumption than drinkers who left the establishments with lower dosages. Gender differences were observed regarding risk behaviors according to BrAC. Among women, the practice of a new episode of alcohol consumption after leaving the nightclub was significantly higher among patrons with a binge drinking pattern. Among men, the same was true for an increase in the use of illicit drugs after leaving the venue. In both sexes, the behaviors were more prevalent among patrons whose BrAC was equivalent to binge drinking compared with patrons whose BrAC was lower than that of binge drinking practices.
It is noteworthy that studies at nightclubs usually give attention to events occurring within the venue and their association with reported or measured alcohol intoxication [42, 43]. In the present study, we pushed forward to understand what happens after a patron leaves a nightclub; in other words, we investigated the most common effects of alcohol and risk behaviors to which they are exposed and their associations with the patrons’ BrAC when they left the venue.
The prevalence of patrons detected with a binge drinking BrAC in Sao Paulo nightclubs was lower than that found in a study conducted in bars and nightclubs of four European cities [33], in which 50.4% of respondents had engaged in binge drinking. It was also lower than the 35.5% prevalence of binge drinking identified among North-Americans approached on the Mexican-US border when returning from bars and nightclubs in the city of Tijuana [44]. In addition, the prevalence of 22% among women and 29% among men for the practice of binge drinking on the day of the nightclub survey was similar to that found for the Brazilian general population when considering a full year interval to measure binge drinking in the past year [45]. However, there has been no previous study on Brazilian drinking environments that allows a proper comparison for trends in prevalence.
Drinking and driving appeared to be the most common risk behavior among patrons after leaving the nightclub. Nevertheless, among this population, increased alcohol breath concentration did not appear to influence this behavior; thus, for both sexes, there was no statistically significant association between drinking and driving and the practice of binge drinking. However, Voas et al. [46] suggested that the efforts of public policies to reduce the pattern of drinking and driving between patrons at drinking locations have shown effects because over time, there appears to be a reduction in the number of drivers with high alcohol blood concentration returning from drinking locations. The present study highlights that the rate of individuals who drink and drive (27.9% of men and 20.4% women) was much higher than the 4.2% found in a representative sample of a population of drivers from Brazilian roads [47]. However, it should be noted that Brazil has one of the most stringent laws for alcohol consumption and traffic. This law, known in Brazil as the "dry law", indicates that no alcohol blood/breath concentration is accepted among drivers, and the penalty for a BrAC >0.01 mg/L ranges from fines to car seizure and arrests (Law No. 12,760 / 2012). However, we have noted that a large portion of the patrons do not felt intimidated by this law, which suggests the need for law enforcement and more sobriety checkpoints.
The use of illicit drugs following the departure of nightclubs, which was already considerably higher than the past month illicit drug use among the Brazilian general population (4.5%) [48], was increased among men with a binge drinking BrAC. However, this percentage was much lower than that found in a study in San Francisco (USA), in which it was estimated that 30% of nightclub attendees had used illicit substances [46]. Nevertheless, we highlight here a greater exposure to the risks of legal, psychological and physical consequences of drug use associated with alcohol use by characterizing polydrug use [49] practiced by these respondents.
Among women, a notable risk behavior increased by binge drinking was the new use of alcohol, in other words, additional drinking after leaving the nightclub. This behavior requires attention because it may suggest a potential alcohol craving for higher alcohol doses induced by the alcohol intoxication, suggesting that one’s own alcohol intoxication prevents adequate control of the amount of alcohol ingested [50]. Thus, in this scenario, women who were already intoxicated, particularly those who should not continue consuming alcohol that night, were the ones most likely to report a new alcohol use. This behavior increases the risk inherent to the alcohol intoxication, which can lead to an alcoholic coma or sexual abuse, as described by Testa et al. [51].
There were also clear deleterious effects of alcohol on the body in approximately 10% of the patrons who reported blackouts and/or physical complications because of alcohol consumption. Again, we face the question of the limits of consumption. It was expected that binge practices would be associated with an increase of these physical effects; however, surprisingly, binge drinking increased the occurrence of these effects by 9 times in men and 5 times in women. Blackouts are one of the most complex effects of alcohol intoxication and are responsible for psychological stress among patrons because this exposes them to risk behaviors that they cannot even report because of the memory loss associated with the blackout [52]. Considering this scenario, all the behaviors reported the next day by these patrons may be underestimated because they do not remember parts of the end of the night.
The scientific literature is scarce regarding the population prevalence of alcohol induced harm in drinking environments. In this sense, this study fills an important gap in the field of individual and public health by identifying the possible role of binge drinking. However, regardless of binge drinking, sexual risk behavior, which is more prevalent among men, draws attention for its potential life-long effects. In Brazil, according to recent governmental data [53], the recrudescence of the HIV epidemic is concentrated among young adults aged 20–25 years; this is coincidently the age category investigated in this survey. This phenomenon indicates the need for tailored campaigns to raise awareness of contagion risks for several STDs in these establishments because of the behavior after leaving the venue and the influence of alcohol on decision making.
The findings presented here are interesting not only in what was found but also in what was not found. Explicitly, many risk behaviors that have previously been identified as associated with binge drinking were not identified in this study in a drinking environment, such as sexual risk behaviors and violent behaviors [27, 54]. However, the binge drinking definition of 5/4 (men/women) doses was established according to findings that after the consumption of this amount or more, individuals are at a greater risk for exhibiting serious alcohol-related problems, such as fights, trouble with police, injuries, and drunk driving, among other subsequent negative health and social consequences [5]. Therefore, this study suggests that ethnicity and sociocultural aspects may influence the binge cutoff measure for the Brazilian population because the majority of the risk behaviors were not associated with the National Institute on Alcohol Abuse and Alcoholism (NIAAA) binge drinking measure of 0.08% BAC (or a BrAC ≥ 0.38 mg/L) [7, 39].
Although this is an innovative study, some limitations are present. The first is the sample loss to follow-up during the different phases of the study. Of the 1832 patrons whose BrAC was measured at the exit of the nightclubs, only 1222 of them answered the online questionnaire 24 hours later that reported their behavior practiced after leaving the venue. Also, the exclusion of highly intoxicated patrons at the exit (n = 67 cases) can probably have underestimate some risky behavior prevalence. In addition, the small number of cases in some response categories, such as "accidents" and "policy involvement” (problems with the police) were difficult to analyze in the logistic regression model. Although an online, anonymous questionnaire increases the validity of the reporting of illegal activities or risk behaviors, it is noted here that the alcoholic blackout could have compromised the validity of the response of the patrons who experienced it.
Conclusions
We note that exposure to risk behaviors among patrons is not limited to events within the venue but also to events occurring after the departure of these establishments and appear to be associated with alcoholic consumption. These results suggest that public policy should provide more efforts at reducing alcoholic harm among nightclubs patrons, taking into account that the risk episodes may occur just after leaving the venue. One of the initial measures to guarantee a lower BrAC at nightclub exits would be nightclub staff training in responsible beverage service (RBS) and future legislation to prevent alcohol sales to drunk individuals, as evidenced by the study of Hughes et al. [55]. However, it is worth noting that the alcohol consumption market in Brazil is unregulated [56], and few or no actions to regulate the physical availability of alcohol [57] have been tested in Brazil. Therefore, it is suggested that the results of this study can guide international effective alcohol public policies aimed at the protection of nightclub patrons by using a triad of education, regulation and effective enforcement, which will allow observable changes in future generations.
Supporting Information
Dataset of the variables used in this manuscript.
(XLSX)
Data Availability
All relevant data are within the paper and its Supporting Information files.
Funding Statement
This work was supported by FAPESP (São Paulo State Research Foundation) - research grant to Dr. Sanchez (grant number 2011/51658-0) (http://www.bv.fapesp.br/pt/pesquisa/?sort=-data_inicio&q2=%28id_pesquisador_exact%3A106030%29+AND+%28%28situacao_exact%3A%22Em+andamento%22+AND+auxilio%3A%2A%29%29). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1. WHO. Global Status Report on Alcohol and Health. Geneva: World Health Organization; 2014. [Google Scholar]
- 2. WHO. The Global burden of disease: 2004 update. Geneva: World Health Organization; 2008. [Google Scholar]
- 3. Rehm J, Mathers C, Popova S, Thavorncharoensap M, Teerawattananon Y, Patra J. Global burden of disease and injury and economic cost attributable to alcohol use and alcohol-use disorders. Lancet. 2009;373(9682):2223–33. 10.1016/S0140-6736(09)60746-7 [DOI] [PubMed] [Google Scholar]
- 4. Norström T, Ramstedt M. Mortality and population drinking: a review of the literature. Drug Alcohol Review. 2005;24(6):537–47. [DOI] [PubMed] [Google Scholar]
- 5. Wechsler H, Nelson TF. Binge drinking and the American college student: what's five drinks? Psychol Addict Behav. 2001;15(4):287–91. [DOI] [PubMed] [Google Scholar]
- 6. Kuntsche E, Rehm J, Gmel G. Characteristics of heavy episodic drinkers in Europe. Soc Sci Med. 2004;59:113–27. [DOI] [PubMed] [Google Scholar]
- 7.NIAAA. National Institute of Alcohol Abuse and Alcoholism Council Approves Definition of Binge Drinking. NIAAA Newsletter. 2004;3(Winter 2004.).
- 8. Wechsler H, Dowdall GW, Davenport A, Rimm EB. A gender-specific measure of binge drinking among college students. Am J Public Health. 1995;85(7):982–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Courtney KE, Polich J. Binge drinking in young adults: Data, definitions, and determinants. Psychol Bull. 2009;135(1):142–56. 10.1037/a0014414 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Lange JE, Voas RB. Defining binge drinking quantities through resulting blood alcohol concentrations. Psychol Addict Behav. 2001;15(4):310–6. [DOI] [PubMed] [Google Scholar]
- 11. Zhao G, Wu C, Houston RJ, Creager W. The effects of binge drinking and socio-economic status on sober driving behavior. Traffic Inj Prev. 2010;11(4):342–52. 10.1080/15389581003789573 [DOI] [PubMed] [Google Scholar]
- 12. Brewer RD, Swahn MH. Binge drinking and violence. JAMA. 2005;294(5):616–8. [DOI] [PubMed] [Google Scholar]
- 13. Naimi TS, Brewer RD, Mokdad A, Denny C, Serdula MK, Marks JS. Binge drinking among US adults. JAMA. 2003;289(1):70–5. [DOI] [PubMed] [Google Scholar]
- 14. Wilsnack R, Wilsnack S, Obot I. Why study gender, alcohol and culture? In: Obot I, Room R, editors. Alcohol, Gender and Drinking Problems: Perspectives from Low and Middle Income Countries. Geneva: World Health Organization; 2005. p. 1–23. [Google Scholar]
- 15. Rehm J, Monteiro M, Room R, Gmel G, Jernigan D, Frick U, et al. Steps towards constructing a global comparative risk analysis for alcohol consumption: determining indicators and empirical weights for patterns of drinking, deciding about theoretical minimum, and dealing with different consequences. Eur Addict Res. 2001;7(3):138–47. [DOI] [PubMed] [Google Scholar]
- 16. Grant BF, Dawson DA, Stinson FS, Chou SP, Dufour MC, Pickering RP. The 12-month prevalence and trends in DSM-IV alcohol abuse and dependence: United States, 1991–1992 and 2001–2002. Drug Alcohol Depend. 2004;74(3):223–34. [DOI] [PubMed] [Google Scholar]
- 17. Grucza RA, Norberg K, Bucholz KK, Bierut LJ. Correspondence between secular changes in alcohol dependence and age of drinking onset among women in the United States. Alcohol Clin Exp Res. 2008;32(8):1493–501. 10.1111/j.1530-0277.2008.00719.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Grucza RA, Bucholz KK, Rice JP, Bierut LJ. Secular trends in the lifetime prevalence of alcohol dependence in the United States: a re-evaluation. Alcohol Clin Exp Res. 2008;32(5):763–70. 10.1111/j.1530-0277.2008.00635.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. McClatchley K, Shorter GW, Chalmers J. Deconstructing alcohol use on a night out in England: Promotions, preloading and consumption. Drug Alcohol Rev. 2014;33(4):367–75. 10.1111/dar.12150 [DOI] [PubMed] [Google Scholar]
- 20. Loft S, Olesen KL, Døssing M. Increased susceptibility to liver disease in relation to alcohol consumption in women. Scand J Gastroenterol. 1987;22(10):1251–6. [DOI] [PubMed] [Google Scholar]
- 21. Fernández-Solà J, Estruch R, Nicolás JM, Paré JC, Sacanella E, Antúnez E, et al. Comparison of alcoholic cardiomyopathy in women versus men. Am J Cardiol. 1997;80(4):481–5. [DOI] [PubMed] [Google Scholar]
- 22. Ammendola A, Gemini D, Iannaccone S, Argenzio F, Ciccone G, Ammendola E, et al. Gender and peripheral neuropathy in chronic alcoholism: a clinical-electroneurographic study. Alcohol Alcohol. 2000;35(4):368–71. [DOI] [PubMed] [Google Scholar]
- 23. Calafat A, Blay NT, Hughes K, Bellis M, Juan M, Duch M, et al. Nightlife young risk behaviours in Mediterranean versus other European cities: are stereotypes true? Eur J Public Health. 2011;21(3):311–5. 10.1093/eurpub/ckq141 [DOI] [PubMed] [Google Scholar]
- 24. Calafat A, Juan M, Duch MA. Preventive interventions in nightlife: a review. Adicciones. 2009;21(4):387–413. [PubMed] [Google Scholar]
- 25. Graham K, Bernards S, Osgood DW, Wells S. Bad nights or bad bars? Multi-level analysis of environmental predictors of aggression in late-night large-capacity bars and clubs. Addiction. 2006;101(11):1569–80. [DOI] [PubMed] [Google Scholar]
- 26. Duff C. The pleasure in context. Int J Drug Policy. 2008;19(5):384–92. [DOI] [PubMed] [Google Scholar]
- 27. Blay N, Calafat A, Juan M, Becona E, Mantecon A, Ros M, et al. [Violence in nightlife environments and its relationship with the consumption of alcohol and drugs among young Spaniards]. Psicothema. 2010;22(3):396–402. [PubMed] [Google Scholar]
- 28. Bellis MA, Hughes K, Calafat A, Juan M, Ramon A, Rodriguez JA, et al. Sexual uses of alcohol and drugs and the associated health risks: a cross sectional study of young people in nine European cities. BMC Public Health. 2008;8:155 10.1186/1471-2458-8-155 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Kelley-Baker T, Mumford EA, Vishnuvajjala R, Voas RB, Romano E, Johnson M. A Night in Tijuana: Female Victimization in a High-Risk Environment. J Alcohol Drug Educ. 2008;52(3):46–71. [PMC free article] [PubMed] [Google Scholar]
- 30. Livingston M, Chikritzhs T, Room R. Changing the density of alcohol outlets to reduce alcohol-related problems. Drug Alcohol Rev. 2007;26(5):557–66. [DOI] [PubMed] [Google Scholar]
- 31. Laranjeira R, Pinsky I, Zaleski M, Caetano R. First Brazilian Household Survey of Patterns of Alcohol Use. Brasília: Secretaria Nacional Antidrogas, Presidência da República; 2007. [Google Scholar]
- 32. Sanchez ZM, Martins SS, Opaleye ES, Moura YG, Locatelli DP, Noto AR. Social factors associated to binge drinking: a cross-sectional survey among Brazilian students in private high schools. BMC Public Health. 2011;11:201 10.1186/1471-2458-11-201 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Hughes K, Quigg Z, Eckley L, Bellis M, Jones L, Calafat A, et al. Environmental factors in drinking venues and alcohol-related harm: the evidence base for European intervention. Addiction. 2011;106 Suppl 1:37–46. 10.1111/j.1360-0443.2010.03316.x [DOI] [PubMed] [Google Scholar]
- 34. Voas RB, Furr-Holden D, Lauer E, Bright K, Johnson MB, Miller B. Portal surveys of time-out drinking locations: a tool for studying binge drinking and AOD use. Eval Rev. 2006;30(1):44–65. [DOI] [PubMed] [Google Scholar]
- 35. Lwanga SK, Lemeshow S. Sample size determination in health studies: a practical manual. Geneva: World Health Organization; 1991. [Google Scholar]
- 36. Clapp JD, Holmes MR, Reed MB, Shillington AM, Freisthler B, Lange JE. Measuring college students' alcohol consumption in natural drinking environments: field methodologies for bars and parties. Eval Rev. 2007;31(5):469–89. [DOI] [PubMed] [Google Scholar]
- 37. Carlini C, Andreoni S, Martins SS, Benjamin M, Sanudo A, Sanchez ZM. Environmental characteristics associated with alcohol intoxication among patrons in Brazilian nightclubs. Drug Alcohol Rev. 2014;33(4):358–66. 10.1111/dar.12155 [DOI] [PubMed] [Google Scholar]
- 38.ABEP, 2012. ABEP—Associação Brasileira de Empresas de Pesquisa. Critério de Classificação Econômica no Brasil [Criteria for Economic Classification in Brazil]. Associação Brasileira de Empresas de Pesquisa, Rio de Janeiro. Available: http://www.abep.org/criterioBrasil.aspx.
- 39. Haffner HT, Graw M, Dettling A, Schmitt G, Schuff A. Concentration dependency of the BAC/BrAC (blood alcohol concentration/breath alcohol concentration) conversion factor during the linear elimination phase. Int J Legal Med. 2003;117(5):276–81. [DOI] [PubMed] [Google Scholar]
- 40. Rao J, Scott A. On Simple Adjustments to Chi-Square Tests with Sample Survey Data. The Annals of Biostatistics. 1987;15(1):385–97. [Google Scholar]
- 41. Perham N, Moore SC, Shepherd J, Cusens B. Identifying drunkenness in the night-time economy. Addiction. 2007;102(3):377–80. [DOI] [PubMed] [Google Scholar]
- 42. Graham K, Osgood DW, Zibrowski E, Purcell J, Gliksman L, Leonard K, et al. The effect of the Safer Bars programme on physical aggression in bars: results of a randomized controlled trial. Drug Alcohol Rev. 2004;23(1):31–41. [DOI] [PubMed] [Google Scholar]
- 43. Graham K, Bernards S, Abbey A, Dumas T, Wells S. Young women's risk of sexual aggression in bars: the roles of intoxication and peer social status. Drug Alcohol Rev. 2014;33(4):393–400. 10.1111/dar.12153 [DOI] [PubMed] [Google Scholar]
- 44. Lange JE, Voas RB. Youth escaping limits on drinking: binging in Mexico. Addiction. 2000;95(4):521–8. [DOI] [PubMed] [Google Scholar]
- 45. Castroand DS, Sanchez ZM, Zaleski M, Alves HN, Pinsky I, Caetano R, et al. Sociodemographic characteristics associated with binge drinking among Brazilians. Drug Alcohol Depend. 2012; 126(1–2):272–6. 10.1016/j.drugalcdep.2012.05.017 [DOI] [PubMed] [Google Scholar]
- 46. Voas RB, Johnson MB, Miller BA. Alcohol and drug use among young adults driving to a drinking location. Drug Alcohol Depend. 2013;132(1–2):69–73. 10.1016/j.drugalcdep.2013.01.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Pechansky F, Duarte Pdo C, De Boni R, Leukefeld CG, von Diemen L, Bumaguin DB, et al. Predictors of positive Blood Alcohol Concentration (BAC) in a sample of Brazilian drivers. Rev Bras Psiquiatr. 2012;34(3):277–85. [DOI] [PubMed] [Google Scholar]
- 48. Duarte P, Stempliuk V, Barroso L. Relatório Brasileiro sobre Drogas [Brazilian Report on Drugs]. Brasilia: Secretaria Nacional de Políticas Sobre Drogas (SENAD); 2010. 456 p. [Google Scholar]
- 49. Smith GW, Farrell M, Bunting BP, Houston JE, Shevlin M. Patterns of polydrug use in Great Britain: findings from a national household population survey. Drug Alcohol Depend. 2011;113(2–3):222–8. 10.1016/j.drugalcdep.2010.08.010 [DOI] [PubMed] [Google Scholar]
- 50. Day AM, Celio MA, Lisman SA, Spear LP. Gender, history of alcohol use and number of drinks consumed predict craving among drinkers in a field setting. Addict Behav. 2014;39(1):354–7. 10.1016/j.addbeh.2013.10.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Testa M, Vanzile-Tamsen C, Livingston JA. The role of victim and perpetrator intoxication on sexual assault outcomes. J Stud Alcohol. 2004;65(3):320–9. [DOI] [PubMed] [Google Scholar]
- 52. Rose ME, Grant JE. Alcohol-induced blackout. Phenomenology, biological basis, and gender differences. J Addict Med. 2010;4(2):61–73. 10.1097/ADM.0b013e3181e1299d [DOI] [PubMed] [Google Scholar]
- 53. Kerr LR, Mota RS, Kendall C, Pinho Ade A, Mello MB, Guimaraes MD, et al. HIV among MSM in a large middle-income country. Aids. 2013;27(3):427–35. 10.1097/QAD.0b013e32835ad504 [DOI] [PubMed] [Google Scholar]
- 54. Abbey A, Zawacki T, Buck PO, Clinton AM, McAuslan P. Sexual assault and alcohol consumption: what do we know about their relationship and what types of research are still needed? Aggression and Violent Behavior. 2004;9(3):271–303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Hughes K, Bellis MA, Leckenby N, Quigg Z, Hardcastle K, Sharples O, et al. Does legislation to prevent alcohol sales to drunk individuals work? Measuring the propensity for night-time sales to drunks in a UK city. J Epidemiol Community Health. 2014;68(5):453–6. 10.1136/jech-2013-203287 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Laranjeira RR. Brazil's market is unregulated. BMJ. 2007; 335(7623):735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Babor T, Caetano R, Casswell S, Edwards G, Giesbrecht N, Graham K, et al. Alcohol: No Ordinary Commodity-Research and Public Policy. 2nd ed Oxford, UK: Oxford University Press; 2010. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Dataset of the variables used in this manuscript.
(XLSX)
Data Availability Statement
All relevant data are within the paper and its Supporting Information files.