

Abstract
Context:
Participation in lacrosse has dramatically increased since 2001. Changes in the game rules, sport equipment, and athlete characteristics have all contributed to the injury patterns in lacrosse over time.
Objective:
A summary of lacrosse-related musculoskeletal injuries.
Data Sources:
Medline, CINAHL, Scopus, and Web of Science were searched for articles relating to the epidemiology and mechanisms of lacrosse injuries in high school and collegiate lacrosse players.
Study Selection:
The search strategy used the following keywords: lacrosse, injury, musculoskeletal, high school, intercollegiate, knee, shoulder, fracture, ankle, foot, concussion, and surveillance. Studies were included if they reported injury risk, injury type, or injury mechanism in high school or collegiate lacrosse players.
Study Design:
Systematic review.
Level of Evidence:
Level 4.
Data extraction:
Injury type, frequency, and mechanism as well as population were extracted.
Results:
Thirteen cohort studies and an additional 15 case series and reports were included. For all lacrosse players, ankle, knee, and hand/wrist were key sites for acute injury. Among collegiate players, preseasonal play elicits more injuries than seasonal play. Female players incur more noncontact and overuse injuries than male players. Boys have 3 to 5 times the risk for sustaining a fracture compared with girls in competition and practice. Women experienced fewer concussions but more facial fractures than men. Injuries to the foot/ankle, head, face, and wrist/hand more often required surgery in girls than in boys.
Conclusion:
Male players incur more injuries than female players. However, because of the collisional nature of play, more shoulder, arm, and upper leg injuries occur in male players. Fractures to the head and hand occur relatively more frequently in female players. Injury risk can be modified with appropriate training regimens and by respecting the game rules.
Keywords: lacrosse, injury, knee, ankle, fracture
US Lacrosse is the national governing body for both women’s and men’s lacrosse. National participation in lacrosse continues to increase rapidly. Participation surveys conducted by US Lacrosse revealed that there was a 10% growth in the sport from 2009 to 2010, with a total of 624,593 players competing on organized teams in the United States.17 This is a dramatic increase in the number of lacrosse players from 2001, with initial tracking numbers indicating 253,931 competitive players. The youth lacrosse contingent has expanded rapidly from 220,797 boys and girls in 2006 to 351,275 in 2011. From 2006 to 2010, the national participation in high school lacrosse increased by 12.2%, reaching 255,314 players by 2010. The National Collegiate Athletic Association (NCAA) reported that men’s lacrosse experienced an 18% net gain in the number of teams from 2010 to 201128 and an increase in the number of athletes from 6551 to 10,903 from 2001 to 2012.29 Women’s lacrosse has also quickly grown. The number of female athletes increased from 5326 to 8482 from 2001 to 2012.29
The explosive growth of the sport has caused an infusion of novice players with varying levels of skill. This growth, particularly in youth and high school lacrosse programs, may not be consistently matched with experienced, knowledgeable coaching and refereeing resources. As lacrosse game rules evolve and equipment properties change, the pattern of musculoskeletal injuries may change. The nature of the lacrosse game involves unique physical challenges that can result in overuse and acute injuries. The combination of the physical stressors and variance in skill level can create a playing environment conducive to injury.
Data are too few in the youth lacrosse or box lacrosse contingents about which conclusions can be developed. The scant evidence from 1 study shows that most injuries are relatively minor in boys and girls, and only a few severe injuries occurred.20 Thus, as most of the musculoskeletal injuries occur in players older than 14 years, this review will present the available data from male and female high school and collegiate lacrosse athletes.
Methods
We conducted a literature search from 1965 to March of 2014 in Medline, CINAHL, Scopus, and Web of Science. The search strategy identified studies in English with MeSH/keywords with all subheadings and free text, including lacrosse, injury, musculoskeletal, high school, intercollegiate, knee, shoulder, fracture, ankle, foot, concussion, and surveillance. Studies were included if they reported injury risk, injury type, or injury mechanism in high school or collegiate lacrosse players. A total of 715 abstracts were retrieved and reviewed by the authors to determine whether the study met the criteria. Over 15 case reports and additional studies of lacrosse-related injuries were included to help provide insight on the mechanism of injury and positional injury risk. The lists of references of retrieved publications were manually checked to add any citations missed by the electronic searches. A total of 13 studies were included in this review (Figure 1).
Figure 1.
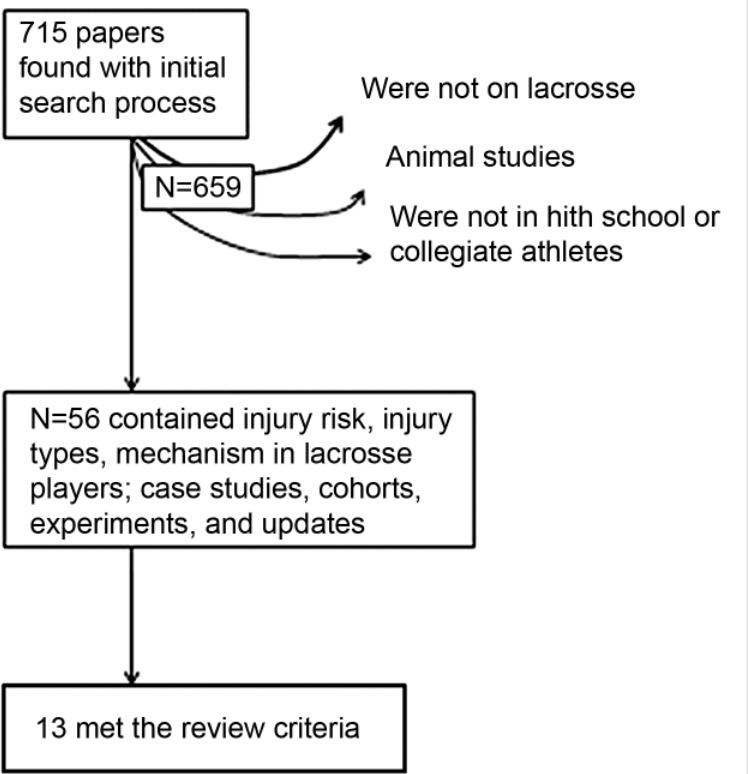
Study inclusion flow diagram.
Nature of the Current Evidence
Data were primarily derived from public high school reporting studies,12,18 surveillance systems,33,34,36 injury updates26 or video review of game play.4,9 The majority of the evidence is epidemiologic, with additional case reports and series of specific injury mechanisms.1,10,14-16,22,24,30,31,35 One cross-sectional study examined lacrosse injuries in persons 4 to 59 years old but fell outside the high school and collegiate classifications.6 A reportable injury is one that occurred as a result of participation in an organized team activity (practice, competition) and required medical attention by an athletic trainer or physician and caused the athlete to miss lacrosse participation for 1 or more days. Injury documentation was obtained primarily from on-site athletic trainers.
Boys’ and Men’s Injuries
A full description of injuries incurred is available in Appendices 1 and 2 (available at http://sph.sagepub.com/content/suppl).
Boys’ High School and Collegiate Populations
Studies from public school systems and regional camps show that the overall injury rate is slightly higher in boys than girls, with 2.89 versus 2.54 injuries per 1000 athlete-exposures (AEs).12 Boys have a 3 times higher game-to-practice injury ratio than girls during seasonal play.12 Boys are also more likely to sustain injuries to the shoulder, arm, and upper leg than girls.12,36
Upper Extremity Injury and Shoulder Instability
Boys have twice the proportion of serious elbow injuries (requiring emergency care in the hospital) and 5 times the proportion of serious shoulder injuries than girls.36 Interestingly, the absolute injury rate is relatively low for elbow injury or pathology, even with a long lever arm. Key rotations in the lacrosse throwing motion are largely dependent on rotations at the pelvis, upper torso, and shoulder and not the elbow.32,37 The percentage of boys and men who experience shoulder injuries ranges from 5% to 12.4%.8,12 Emergent injuries to the shoulder are 5 times more common in boys than girls.36 Interestingly, the prevalence of shoulder injuries increases in parallel with the level of contact and amount of protective equipment.36
Knee and Hip Injuries
Boys incurred similar anterior cruciate ligament injury rates as girls (0.79 vs 0.78), but lower meniscal injury rates (0.44 vs 0.61) and higher medial collateral ligament injury rates (0.76 vs 0.29).33 The rate of knee injuries is higher in summer camps, where there is an intense volume of activity.12 Lacrosse players had the highest percentage of knee injuries requiring surgical repair before return to play compared with other contact and noncontact sports.33 Hip injuries in lacrosse players are relatively rare26 and occur in low frequencies (3.3-5.6 per 1000 AEs).8
Ankle Injuries
Boys are 1.4 times more likely to sustain ankle injury than girls during summer camp.12 The NCAA Surveillance System found that ankle ligament sprains comprise 14.4% of the total injuries reported for men’s lacrosse.
Fractures
Compared with girls, the overall fracture rate is higher in boys irrespective of the nature of the AE, and 17.2% of these fractures required surgery.34 A total of 69.3% of fracture injuries requiring surgical repair included hand/finger, lower leg, nose, ankle, and forearm.34 After ligament sprains, fractures were the second most common diagnosis requiring surgery in high school athletes.34 Some evidence indicates that increasing age is inversely related to the proportion of fractures in injured players.34 Body mass index has not been found to be related to fracture incidence.34 Irrespective of player position, high speed lacrosse ball impact can strike the throat and cause displaced transcricoid fracture.10 Newer helmet designs have begun to incorporate longer chin protectors that may offer more protection of the throat but reduce forward flexion of the neck.
Concussion
The incidence of concussions in boys lacrosse has increased considerably from 1998 to 2008, with a rate of 0.1 concussions per 1000 AEs in 1998 up to 0.6 in 2008, which corresponds to an annual increase by 16.5%.18 Lacrosse concussion rates are second only to boys’ football.18 Helmets alone do not always protect against concussion injury.3,8
Girls’ and Women’s Injuries
Girls and women are not permitted to make body contact with another player, but may check (defined as “an attempt to dislodge the ball from an opponent’s stick by using controlled stick-to-stick contact”)32 the opponent’s stick with their own only when the 1 player has possession of the ball. No additional stick-to-stick contact is permitted. In girls’ lacrosse, the goalie is also required to wear a padded/protective girdle and shin guards. The last major difference between the male and female play of lacrosse is penalties or fouls. In girls’/women’s lacrosse, when a penalty or foul is called by the referee, all players on the field must stop instantly.
Girls’ High School and Collegiate Populations
A summary of the injuries reported is available in Appendices 1 and 2 (available at http://sph.sagepub.com/content/suppl). The only protective gear women and girls wear are goggles and mouth guards. Overall, the injury patterns differ from the boys in several respects. A total of 12.8% and 32.5% of the injuries occurred within the goal area and within the goal’s 8-meter arc, respectively.7 At the time of the injury, 69.7% of women were handling the ball and/or were in loose ball scenarios.7
Upper Extremity and Shoulder Injuries
Girls and women do have lower rates of injury to the shoulders and arm during competition and practice, with frequencies of these injuries ranging from 1.6% to 4.1% of the total injuries reported.12 Emergent shoulder injuries occur 5 times less in girls than boys, and fewer of these injuries were fractures.
Lower Extremity Injuries
During regular-season play, girls have higher rates of knee injuries than boys.12 During summer camp play, the primary injury types for girls were overuse (19% of total injuries), illegal stick/object hit (19%), ball contact with the body (15%), and falling to the ground with or without body contact (24%)12; 39.3% of lacrosse players with knee injuries required surgery, second only to cheerleading at 40%.33 Surgery was required for meniscus (22%) and ligament (65.4%) injuries to the knee. The NCAA Surveillance System data from 15 sports revealed that anterior cruciate ligament injuries comprised 4.3% of all injuries in women’s lacrosse.13 Women experience relatively low rates of hip and pelvis muscle-tendon strain compared with other lower extremity joints (2.3% to 5.0% in practices and games).7 Ankle injuries comprise 15% to 25.1%12,25 of total injuries in girls and women.
Fractures
The hand/wrist is the most commonly fractured site in girls’ lacrosse.34 Boys and men incur head or facial fractures at a frequency of 3% to 3.5% of all head injuries, whereas girls and women incur higher fracture frequencies of 14.0% to 20.9% of all head injuries.19
Head Injuries and Concussions
Evidence from district-mandated electronic medical records indicates concussion injury is increasing in girls similar to that in boys.18 Interestingly, girls have higher rates of head injuries than boys,12 but the overall concussion incidence is lower in girls than in boys. Data from the Consumer Product Safety Commission’s National Electronic Injury Surveillance System showed that female players in general had a greater percentage of head and face injuries than male players (30.1% vs 18.0%, respectively).6 Importantly, the incidence of head injuries is greater in varsity high school players compared with junior varsity.4
Positional Differences in Injury Risk
Goalies
Hand grip on the stick may expose the thumbs to injury.9 An extremely rare injury is commotio cordis.23 Adolescents are more likely to experience this injury, where it can happen with a low-velocity impact.23 Commotio cordis has occurred in midfielders as well as goalies wearing proper chest protection.23
Defensemen
There has not yet been a rigorous analysis of position-specific musculoskeletal injuries in lacrosse defenders.
Attack and Midfielders
Up to 52.5% of hand and finger injuries in men’s and women’s lacrosse were caused by offensive stick hits, and 42.7% to 59.4% of injuries occurred in the thumb.2 Early data of a small cohort indicated that 28% of attackmen who attended a summer league incurred acromioclavicular joint dislocations and clavicular fractures in attackers.31
Conclusion
Male players incur a greater number of injuries than female players, but the prevalence and type of injuries differ. Because of contact, more shoulder, arm, and upper leg injuries occur in male players, and more fractures to the head and hand occur in female players. Common injury sites for lacrosse players in all age groups and sexes include the ankle, knee, and hand/wrist. Injury risk can be modified with appropriate training protocols and with respect of the rules of play.
Supplementary Material
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
References
- 1. Attia MW, Russell J. Isolated first rib fracture in a high school lacrosse player. Pediatr Emerg Care. 2010;16:31-32. [DOI] [PubMed] [Google Scholar]
- 2. Bowers AL, Horneff JG, Baldwin KD, Huffman GR, Sennett BJ. Thumb injuries in intercollegiate men’s lacrosse. Am J Sports Med. 2010;38:527-531. [DOI] [PubMed] [Google Scholar]
- 3. Caswell SV, Deivert RG. Lacrosse helmet designs and the effects of impact forces. J Athl Train. 2002;37:164-171. [PMC free article] [PubMed] [Google Scholar]
- 4. Caswell SV, Lincoln AE, Almquist JL, Dunn RE, Hinton RY. Video incident analysis of head injuries in high school girls’ lacrosse. Am J Sports Med. 2012;40:756-762. [DOI] [PubMed] [Google Scholar]
- 5. Centers for Disease Control and Prevention. Injury prevention & control: traumatic brain injury. http://www.cdc.gov/concussion/policies.html. Accessed June 12, 2013.
- 6. Diamond PT, Gale SD. Head injuries in men’s and women’s lacrosse: a 10 year analysis of the NEISS database. National Electronic Injury Surveillance System. Brain Inj. 2001;15:537-544. [DOI] [PubMed] [Google Scholar]
- 7. Dick R, Lincoln AE, Agel J, Carter EA, Marshall SW, Hinton RY. Descriptive epidemiology of collegiate women’s lacrosse injuries: National Collegiate Athletic Association Injury Surveillance System, 1988-1989 through 2003-2004. J Athl Train. 2007;42:262-269. [PMC free article] [PubMed] [Google Scholar]
- 8. Dick R, Romani WA, Agel J, Case JG, Marshall SW. Descriptive epidemiology of collegiate men’s lacrosse injuries: National Collegiate Athletic Association Injury Surveillance System, 1988-1989 through 2003-2004. J Athl Train. 2007;42:255-261. [PMC free article] [PubMed] [Google Scholar]
- 9. Elkousy HA, Janssen H, Ferraro J, Levin LS, Speer K. Lacrosse goalkeeper’s thumb. A preventable injury. Am J Sports Med. 2000;28:317-321. [DOI] [PubMed] [Google Scholar]
- 10. French C, Kelley R. Laryngeal fractures in lacrosse due to high speed ball impact. J Am Med Assoc Otol Head Neck Surg. 2013;139:735-738. [DOI] [PubMed] [Google Scholar]
- 11. Hall C, Friel K, Dong M, et al. Epidemiology of injuries in the elite level female high school lacrosse player. Res Sports Med. 2013;21:229-239. [DOI] [PubMed] [Google Scholar]
- 12. Hinton RY, Lincoln AE, Almquist JL, Douoguih WA, Sharma KM. Epidemiology of lacrosse injuries in high school-aged girls and boys: a 3-year prospective study. Am J Sports Med. 2005;33:1305-1314. [DOI] [PubMed] [Google Scholar]
- 13. Hootman JM, Dick R, Agel J. Epidemiology of collegiate injuries for 15 sports: summary and recommendations for injury prevention initiatives. J Athl Train. 2007;42:311-319. [PMC free article] [PubMed] [Google Scholar]
- 14. Hutchinson PH, Stieber J, Flynn J, Ganley T. Complete and incomplete femoral stress fractures in the adolescent athlete. Orthopaedics. 2008;31:604. [PubMed] [Google Scholar]
- 15. Kang L, Belcher D, Hulstyn MJ. Stress fractures of the femoral shaft in women’s college lacrosse: a report of seven cases and a review of the literature. Br J Sports Med. 2005;39:902-906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Klingenstein GG, Martin R, Kivlan B, Kelly BT. Hip injuries in the overhead athlete. Clin Orthop Relat Res. 2012;470:1579-1585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Lacrosse US. USL study reveals continued growth. http://www.uslacrosse.org/multimedia-center/press-releases-news/postid/252/usl-study-reveals-continued-growth.aspx. Accessed April 5, 2013.
- 18. Lincoln AE, Caswell SV, Almquist JL, Dunn RE, Norris JB, Hinton RY. Trends in concussion incidence in high school sports: a prospective 11-year study. Am J Sports Med. 2011;39:958-963. [DOI] [PubMed] [Google Scholar]
- 19. Lincoln AE, Hinton RY, Almquist JL, Lager SL, Dick RW. Head, face and eye injuries in scholastic and collegiate lacrosse. Am J Sports Med. 2007;35:207-215. [DOI] [PubMed] [Google Scholar]
- 20. Lincoln AE, Yeger-McKeever M, Romani W, Hepburn LR, Dunn RE, Hinton RY. Rate of injury among youth lacrosse players. Clin J Sports Med. 2014;24:355-357. [DOI] [PubMed] [Google Scholar]
- 21. Marar M, McIlvain NM, Fields SK, Comstock RD. Epidemiology of concussions among United States high school athletes in 20 sports. Am J Sports Med. 2012;40:747-755. [DOI] [PubMed] [Google Scholar]
- 22. Marchant MHJ, Gambardella RA, Podesta L. Superficial radial nerve injury after avulsion fracture of the brachioradialis muscle origin in a professional lacrosse player: a case report. J Shoulder Elbow Surg. 2009;18:e9-e12. [DOI] [PubMed] [Google Scholar]
- 23. Maron BJ, Doerer JJ, Haas TS, Estes NA, Hodges JS, Link MS. Commotio cordis and the epidemiology of sudden death in competitive lacrosse. Pediatrics. 2009;124:966-971. [DOI] [PubMed] [Google Scholar]
- 24. Matich AJ, Petron DJ, Merrell SW, Macintyre JG. Bilateral lower leg pain in a female collegiate lacrosse player. Curr Sports Med Rep. 2009;8:315-317. [DOI] [PubMed] [Google Scholar]
- 25. Matz SO, Nibbelink G. Injuries in intercollegiate women’s lacrosse. Am J Sports Med. 2004;32:608-611. [DOI] [PubMed] [Google Scholar]
- 26. McCulloch PC, Bach BR., Jr Injuries in men’s lacrosse. Orthopaedics. 2007;30:29-34. [DOI] [PubMed] [Google Scholar]
- 27. Mihata LC, Beutler AI, Boden BP. Comparing the incidence of anterior cruciate ligament injury in collegiate lacrosse, soccer, and basketball players: implications for anterior cruciate ligament mechanism and prevention. Am J Sports Med. 2006;34:899-904. [DOI] [PubMed] [Google Scholar]
- 28. National Collegiate Athletic Association. NCAA participation rates going up: at least 444,000 student-athletes playing on 18,000 teams. http://www.ncaa.com/news/ncaa/article/2011-11-02/ncaa-participation-rates-going. Accessed on April 5, 2013.
- 29. National Collegiate Athletic Association. NCAA student-athlete participation hits 450,000. http://www.ncaa.org/about/resources/media-center/news/ncaa-student-athlete-participation-hits-450000. Accessed April 5, 2013.
- 30. O’Neill PJ, Cosgarea AJ, McFarland EG. Unusual double clavicle fracture in a lacrosse player. Clin J Sports Med. 2000;10:69-71. [DOI] [PubMed] [Google Scholar]
- 31. Silloway KA, McLaughlin RE, Edlich RC, Edlich RF. Clavicular fractures and acromioclavicular joint dislocations in lacrosse: preventable injuries. J Emerg Med. 1985;3:117-121. [DOI] [PubMed] [Google Scholar]
- 32. Slater CD, Chen C, Zdziarski LA, et al. Kinematic characterization of lacrosse shooting motions of the dominant and non-dominant side. Med Sci Sport Exerc. 2014;46:S408. [Google Scholar]
- 33. Swenson DM, Collins CL, Best TM, Flanigan DC, Fields SK, Comstock RD. Epidemiology of knee injuries among U.S. high school athletes, 2005/2006-2010/2011. Med Sci Sport Exerc. 2013;45:462-469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Swenson DM, Henke NM, Collins CL, Fields SK, Comstock RD. Epidemiology of United States high school sports-related fractures, 2008-09 to 2010-11. Am J Sports Med. 2012;40:2078-2084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Wild AT, Begly JP, Garzon-Muvdi J, Desai P, McFarland EG. First-rib stress fracture in a high-school lacrosse player: a case report and short clinical review. Sports Health. 2011;3:547-549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Yard EE, Comstock RD. Injuries sustained by pediatric ice hockey, lacrosse, and field hockey athletes presenting to United States emergency departments, 1990-2003. J Athl Train. 2006;41:441-449. [PMC free article] [PubMed] [Google Scholar]
- 37. Zdziarski LA, Chen C, Slater CD, et al. Dominant versus non-dominant lacrosse throw sex differences: a potential for injury? Med Sci Sport Exerc. Annual Meeting 2014; May 27-31, 2014, Orlando, FL. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.