

Significance
Most childhood outcomes pattern by socioeconomic status (SES). Children from low-SES families complete less education, have worse health, and are convicted of more crimes. To ameliorate these disparities, policymakers are incorporating character-skills training into school curricula and social services. Among other goals, these programs attempt to improve self-control, or the ability to resist temptations that interfere with long-term aspirations. However, data suggest that self-control has unforeseen consequences for the health of low-SES youth. Here, we follow 292 African American teenagers as they transition into adulthood. Among low-SES youth, self-control forecasted better psychosocial outcomes, including less depression, substance use, and aggression. However, it also forecasted more rapid immune cell aging, highlighting the potential health costs of successful adjustment for disadvantaged youth.
Keywords: health disparities, resilience, stress, poverty, aging
Abstract
There are persistent socioeconomic disparities in many aspects of child development in America. Relative to their affluent peers, children of low socioeconomic status (SES) complete fewer years of education, have a higher prevalence of health problems, and are convicted of more criminal offenses. Based on research indicating that low self-control underlies some of these disparities, policymakers have begun incorporating character-skills training into school curricula and social services. However, emerging data suggest that for low-SES youth, self-control may act as a “double-edged sword,” facilitating academic success and psychosocial adjustment, while at the same time undermining physical health. Here, we examine this hypothesis in a five-wave study of 292 African American teenagers from rural Georgia. From ages 17 to 20 y, we assessed SES and self-control annually, along with depressive symptoms, substance use, aggressive behavior, and internalizing problems. At age 22 y, we obtained DNA methylation profiles of subjects’ peripheral blood mononuclear cells. These data were used to measure epigenetic aging, a methylation-derived biomarker reflecting the disparity between biological and chronological aging. Among high-SES youth, better mid-adolescent self-control presaged favorable psychological and methylation outcomes. However, among low-SES youth, self-control had divergent associations with these outcomes. Self-control forecasted lower rates of depressive symptoms, substance use, aggressive behavior, and internalizing problems but faster epigenetic aging. These patterns suggest that for low-SES youth, resilience is a “skin-deep” phenomenon, wherein outward indicators of success can mask emerging problems with health. These findings have conceptual implications for models of resilience, and practical implications for interventions aimed at ameliorating social and racial disparities.
Self-control is a powerful determinant of success across the lifespan. Defined as the capacity to regulate one’s thoughts, feelings, and actions (1), self-control helps people to resolve motivational conflicts between concrete, proximal goals and abstract, distal goals (2). People with good self-control resist temptations that otherwise would impede progress toward valued long-term goals. At the same, these individuals more easily initiate and sustain behaviors that facilitate attainment of those goals. In prospective studies that follow children into adulthood, self-control consistently presages favorable life outcomes. Youth who exhibit greater self-control go on to perform better in school, earn higher salaries, remain stably employed, and save more money. These youth are less likely to use drugs, be arrested for and convicted of crimes, and develop psychiatric disorders. In early adulthood, these youth also show better physical health (3–8). These associations are generally independent of confounds like demographic characteristics, general intelligence, and psychiatric history.
In the United States, there are persistent socioeconomic disparities in many aspects of child development (9, 10). Relative to their affluent peers, children of lower socioeconomic status (SES) experience more academic difficulties, complete less education, have a higher prevalence of physical health problems, teenage pregnancies, and activity-limiting conditions and are more likely to be convicted of, and incarcerated for, criminal offenses (11–13). Recognizing that disparities in self-control partly underlie these trends (3), scholars are increasingly advocating for programs that provide low-SES youth with character-skills training, which along with self-control, includes traits like “grit,” optimism, and persistence (14–17). These efforts have gained momentum among policymakers. For example, the US government’s Administration for Children and Families is developing behavioral interventions to enhance the outcomes of social-service programs that it offers to low-income American families. Self-control is a major target of these interventions.
As interest in character-skills development has surged, a parallel literature has been developing, which suggests that self-control may have unforeseen health consequences, particularly for low-SES children from minority backgrounds. Brody et al. (18) followed rural African American children over 8 y, many of whom were living below the federal poverty threshold. Teachers made annual ratings of children’s self-control from ages 11 to 13 y, which were used to forecast young adult outcomes; when assessed at age 19 y, children with better self-control went on to display what psychologists call resilience. Despite being low-SES, these children had fewer depressive symptoms and less substance use, rule breaking, and aggressive behavior as young adults. In analyses of health status, however, the opposite pattern emerged. To the extent that they had better self-control, low-SES children went on to experience greater cardiometabolic risk as young adults, as reflected on a composite of obesity, blood pressure, and the stress hormones cortisol, epinephrine, and norepinephrine. Similar conclusions emerged in a subsequent analysis of the same cohort, which mapped the trajectories of a subgroup of participants who would normatively be viewed as resilient. These individuals had achieved sustained academic success—they had graduated from high school and were now attending college—despite living in challenging neighborhoods with concentrated poverty. Compared with other participants, this cohort had lower rates of cigarette, alcohol, and marijuana use at age 20 y. However, this resilience was only “skin deep.” Despite academic success and healthy lifestyles, these youth showed relatively poor cardiometabolic health at age 20 y, as reflected in obesity, blood pressure, and stress hormones (19).
These findings suggest that self-control may act as a “double-edged sword” in low-SES youth, facilitating academic success and psychosocial adjustment, while at the same time undermining cardiometabolic health. What could explain these divergent outcomes? Research shows that for low-SES youth, particularly those of African American descent, achieving normatively favorable outcomes poses intense self-regulatory demands (20–22). Because such demands result in sustained activation of stress hormone systems (18, 19, 23–25), we reasoned they would prematurely age bodily tissue through a process known as weathering (26). Here, we test this hypothesis in a new sample of rural African American youth, who were followed across the transition from adolescence to adulthood. To clarify the mechanisms by which skin-deep resilience develops, we focus on aging of immune cells, using an epigenetic biomarker derived from DNA methylation. This epigenetic clock has been validated in cells from over a dozen tissues and reflects the disparity between biological and chronological age. Using this metric, faster aging rates have been documented in tumor-derived cells from over 20 cancers, as well as liver biopsies from obese patients (27–29). Faster epigenetic aging also presages higher risks for all-cause mortality (30).
Results
The subjects were part of a larger study, Adults in the Making (AIM), which included five waves of assessment (31). As Table 1 shows, the sample consisted of adolescents from predominately working-poor families; 65% of the subjects lived in single-parent households, and 45% had incomes below the federal poverty threshold. Fewer than 10% of subjects were from households where a caregiver had a bachelor’s degree. Annually from ages 17 to 19 y, subjects completed validated measures of self-control, which were supplemented by caregiver reports. From these data, we generated a composite indicator of “Self-Control” by aggregating standardized values across assessments, respondents, and instruments (see details in Methods). At each wave, we also gathered socioeconomic data from caregivers and formed a composite that assigned one point for each of six indicators of disadvantage (see details in Methods). Psychosocial outcomes were assessed annually from ages 17 to 20 y, via youth reports of depressive symptoms and substance use, as reflected in cigarette, alcohol, and marijuana consumption and parent reports of aggressive behavior and internalizing symptoms. Approximately 2 y later, when subjects were an average of 22 y old, we collected blood to measure epigenetic aging. DNA was extracted from peripheral blood mononuclear cells (PBMCs) and hybridized to HumanMethylation450 BeadChips following the manufacturer’s protocol; β values were used to generate two metrics of epigenetic aging, based on formulas provided by Horvath (27) and Hannum (28). All data are contained in Dataset S1.
Table 1.
Characteristics of the sample at study entry, when subjects were age 17 y (n = 292)
| Characteristics | Percentage or mean SD |
| Female sex, % | 63.7 |
| Parent education | |
| <High school, % | 20.6 |
| High school degree or GED, % | 25.5 |
| Some college or trade school, % | 44.1 |
| ≥College graduate, % | 9.8 |
| Single-parent household, % | 64.7 |
| Family median monthly income | $2,019.13 |
| Family poverty by federal guidelines, % | 43.8 |
Initially, we tested hypotheses in linear regression equations, where outcomes were predicted from three blocks of variables: covariates, main effects of Self-Control and “Disadvantage” at ages 17–19 y, and the interaction of these variables. In all equations, sex was modeled as a covariate, as was receipt of the AIM intervention (which did not affect behavioral or epigenetic outcomes reported here; P > 0.37). Consistent with previous research, there were main effects of adolescent self-control on all age 20 y psychosocial outcomes, even after accounting for age 17 y values (SI Appendix, Table S1; P = 0.0005–0.02; ΔR2 = 0.01–0.04). To the extent that they had better self-control in mid-adolescence, subjects experienced declines in depressive symptoms, internalizing problems, substance use, and aggressive behavior as they transitioned into adulthood. These patterns were consistent across strata of disadvantage, except in the case of substance use, where there was a significant interaction (P = 0.05). We used standard methods to clarify the nature of this interaction (32), plotting estimated age 20 y substance use by lower (−1.5 SD) and higher (+1.5 SD) levels of Self-Control and Disadvantage, after partialing out covariates. SI Appendix, Fig. S1 shows that as disadvantage increased, self-control’s association with substance use became more negative.
We repeated these analyses with indicators of epigenetic age acceleration. SI Appendix, Table S2 shows the significant Self-Control × Disadvantage interactions for both metrics (P = 0.003–0.004; ΔR2 = 0.03–0.04). We plotted these interactions in Figs. 1 and 2 and computed simple slopes, again using standard methods (32). For subjects who were less disadvantaged, the patterns mirrored behavioral outcomes. In other words, better mid-adolescent self-control presaged less epigenetic aging of PBMCs by young adulthood. However, as in previous reports of skin-deep resilience, psychosocial and biomedical outcomes diverged among the sample’s more disadvantaged youth. For them, better mid-adolescent self-control presaged more epigenetic aging of PBMCs by young adulthood. At the sample’s typical level of disadvantage, self-control and epigenetic age were unrelated.
Fig. 1.
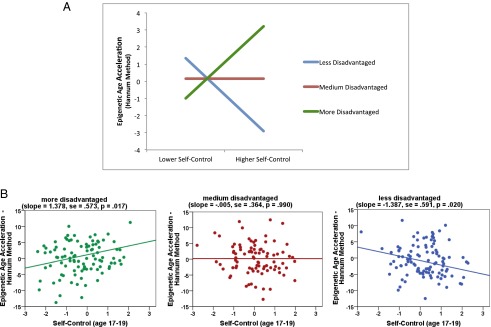
Self-control’s association with epigenetic age acceleration varies according to SES. (A) Depiction of estimated Hannum values at lower (−1.5 SD) and higher (+1.5 SD) levels of self-control and socioeconomic disadvantage. (B) Depiction of individual data points and regression slopes for subjects who are more (≥1.5 SD above sample mean) (Left), medium (−1.49 to +1.49 SD) (Center), and less (less than or equal to −1.5 SD) (Right) disadvantaged relative to the sample distribution.
Fig. 2.
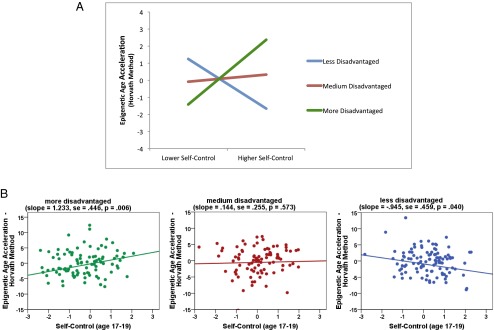
Self-control’s association with epigenetic age acceleration varies according to SES. (A) Depiction of estimated Horvath values at lower (−1.5 SD) and higher (+1.5 SD) levels of self-control and socioeconomic disadvantage. (B) Depiction of individual data points and regression slopes for subjects who are more (≥1.5 SD above sample mean) (Left), medium (-1.49 to +1.49 SD) (Center), and less (less than or equal to −1.5 SD) (Right) disadvantaged relative to the sample distribution.
Although these patterns are suggestive of skin-deep resilience, they do not address convergence of outcomes at the individual level. In other words, they do not answer the following question: Are the same disadvantaged youth, with high self-control, having relatively good psychosocial and relatively poor epigenetic outcomes? To address this question, we performed latent class growth analyses (33), using data from ages 17 to 19 y to sort youth into categories based on Disadvantage and Self-Control. Model-fit indices suggested a parsimonious four-group solution (SI Appendix, Tables S3 and S4). The solution first stratified the sample into groups who were more or less disadvantaged and then into groups in whom self-control was either stably low or high increasing (i.e., grew steadily across adolescence). The percentage of subjects in each group was 14% (more disadvantaged/low self control), 27% (more disadvantaged/high self control), 26% (less disadvantaged/low self control), and 33% (less disadvantaged/high self control).
When the groups were compared, results mirrored regression analyses. Specifically, better mid-adolescent self-control presaged favorable young adult psychosocial outcomes across the sample (SI Appendix, Table S5). On all four of psychosocial outcomes—depressive symptoms, internalizing problems, substance use, and aggressive behavior—the groups high in self-control fared better (Fig. 3), as reflected by smaller intercept values and/or more favorable trajectories. However, for epigenetic aging, self-control’s effects depended on the level of disadvantage (F = 3.48–3.89; P = 0.01–0.02; SI Appendix, Table S6 and Fig. 4). Among more disadvantaged subjects, better self-control was associated with a 1.46- to 2.27-y acceleration of epigenetic aging (by Hannum and Horvath methods, respectively). By contrast, among less-disadvantaged subjects, better self-control was associated with a 0.27- to 2.14-y deceleration (by Horvath and Hannum methods, respectively).
Fig. 3.
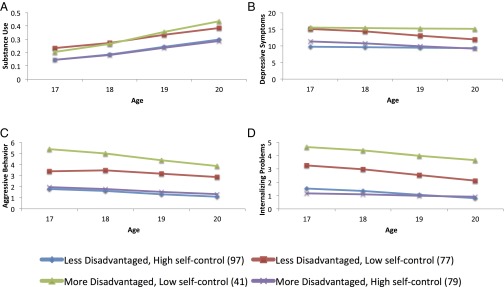
Trajectories of psychosocial adjustment from ages 17 to 20 y as a function of latent class grouping on self-control and socioeconomic disadvantage. Outcomes are substance use (A), depressive symptoms (B), aggressive behavior (C), and internalizing problems (D).
Fig. 4.

Epigenetic age acceleration by latent class grouping on self-control and socioeconomic disadvantage. (A) Hannum metrics. (B) Horvath metrics.
Discussion
Previously, we reported a pattern of skin-deep resilience in low-SES African American youth, wherein self-control portends favorable psychosocial outcomes but worse cardiometabolic health status (18, 19). Here, we extend these findings to a new cohort of adolescents making the transition into adulthood and highlight premature aging of PBMCs as a mechanism that could underlie this phenomenon. How this process unfolds remains unclear. We considered the role of obesity, because youth who exhibit skin-deep resilience have greater body mass (18, 19), which in turn relates to faster epigenetic aging (29). However, mediation analyses did not yield support for this scenario nor one wherein these youth have more general life stress (SI Appendix, Table S7). Nonetheless, the patterns here converge with evidence that relentlessly pursuing goals can undermine health (34), particularly when structural forces like discrimination impede progress toward those goals (20, 23). As disadvantaged youth strive for favorable life outcomes, they have substantial barriers to overcome and competing demands to balance, including resource-deprived schools, family obligations, and managing social identity threats (35). These challenges are particularly salient for African Americans.
Navigating these challenges requires intense and persistent self-control (36), which is metabolically and behaviorally demanding to sustain. Acutely, exerting self-control triggers the release of stress hormones (24, 25) and erodes the ability to resist tempting stimuli, like high-fat food (37). These effects subside when people can suspend willpower and indulge in restorative activities. However, for lower-SES youth, opportunities for respite are likely to be infrequent. To achieve upward mobility, these youth must overcome multiple obstacles and often do so with limited support from their schools, peers, and families (12). Even if they succeed, these youth may go on to experience alienation in university and workplace settings and discrimination if they are African American. Collectively, these experiences seem likely to cause persistent activation of stress-response systems, in particular the sympathetic nervous system and hypothalamic–pituitary–adrenocortical axis. The hormonal products of these systems, glucocorticoids and catecholamines, are elevated in youth who exhibit skin-deep resilience (18, 19). These hormones also can modify the chromatin architecture of leukocytes by altering the enzymatic activity of DNA methyltransferases, as well as histone deacetylases and acetyltransferases (38).
Future research should explicitly test these mechanistic hypotheses. We are unable to do so here because AIM did not assess stress hormone output or obtain methylation profiles during adolescence. A follow-up study with multiple waves of psychosocial, hormonal, and epigenetic data would be ideally suited to identifying mechanisms. In future research, it also will be important to establish the demographic circumstances in which skin-deep resilience develops. To date, this work has focused exclusively on low-SES, African American youth, living in rural areas of the South. As a consequence, it remains unclear whether vulnerability to skin-deep resilience accrues by virtue of race, class, geography, or interaction(s) of these factors. Further research is also needed to clarify the nature and meaning of self-control in the population of interest here. Self-control is a multidimensional construct, and the questionnaires we used capture elements of industriousness, seriousness, impulsivity, and perseverance. To understand the origins of skin-deep resilience, research must determine which of these characteristics presage health problems. Laboratory observations would be especially valuable in this regard, providing researchers with an opportunity to catalog specific behaviors and their relationship with health outcomes. These observations also would clarify whether our questionnaires are capturing the same phenomenon across the sample. It is possible these scales capture distinct behaviors and/or competencies in disadvantaged youth who go on to have better vs. worse health outcomes. Finally, additional research is needed to understand the causes and effects of epigenetic age acceleration, particularly in youth. Although epigenetic clocks are widely believed to reflect premature aging (27–30), they also might conceivably tap cellular maturation in younger populations. If so, our findings would suggest that self-control forecasts precocious development in at-risk youth, rather than weathering. Viewed in light of our previous findings on cardiometabolic risk (18, 19), we see this as an unlikely possibility but one that should be considered in future research.
Since 2000, the prevalence of childhood poverty in America has increased and so have the magnitude of socioeconomic disparities in many aspects of youth development (39). These trends are fueling concerns about public health, human capital, and economic security in the coming decades (15, 17). As one way to counteract these effects, policymakers are drawing on self-control research and incorporating character-building interventions into school curricula and government programs. Although these interventions will likely improve the educational and psychosocial outcomes of low-SES youth, the accumulating data on skin-deep resilience suggest the potential for unintended health consequences. Ironically, the children most vulnerable to such consequences—those from disadvantaged families—already have disproportionately more health problems. Thus, to maximize return on human-capital investments, policymakers should broaden character-building programs to include health education and, where possible, monitoring and treatment of emerging medical problems. This approach could mitigate health problems that prevent upwardly mobile youth from realizing their full potential. More broadly, these findings challenge our view of what it means to be resilient. Current thinking suggests that if low-SES youth do well in school and stay out of trouble, they have overcome disadvantage. As we show, that is only partially accurate.
Methods
Sample.
AIM was a randomized trial focused on alcohol- and substance-use prevention in African American teenagers who were making the transition to adulthood (31). It recruited 496 youth from public schools in six rural counties in Georgia. Subjects were enrolled at age 17 y and randomly assigned to AIM or control condition. The intervention consisted of six weekly group meetings held at community facilities, with separate parent and youth skill-building sessions and a family curriculum. The University of Georgia’s Institutional Review Board approved AIM’s protocol. At each wave, parents gave written consent and youths gave written assent or consent.
The intervention did not influence any of the psychosocial or epigenetic outcomes reported here (P > 0.37; SI Appendix, Tables S1 and S2), but receipt of AIM is nonetheless controlled in all analyses. Of the 496 Wave 1 participants, 424 provided self-report data at Wave 4 (age 20 y, a retention rate of 85.5%). Of these youth, 292 (68.9%) agreed to the blood draw at age 22 y and constitute the analytic sample. Using independent t tests and χ2 analyses, we compared these youth with the broader sample and found no differences on major study variables listed in Table 1. There was one exception: missing methylation data were more common in male versus female subjects, χ2 (1) = 5.76, P = 0.02. Thus, sex was controlled in all analyses.
Psychosocial Assessments.
Self-control and socioeconomic disadvantage were assessed annually from ages 17 to 19 y. At each wave, subjects completed the 11-item Self-Control Inventory (40) and 23-item Self-Regulation Questionnaire (41). To supplement self-reports, we had a caregiver describe each subject’s disposition on the Self-Control Inventory. Both of these scales have been extensively validated and showed high internal consistency (α = 0.87–0.96), cross-wave stability (r = 0.54–0.63), and parent-child concordance here (r = 0.30). These scales also were strongly intercorrelated (average r = 0.76). Accordingly, we formed a formed a Self-Control composite by aggregating standardized scores across assessments, respondents, and instruments. At each wave, we also gathered SES data from caregivers and formed a disadvantage composite that assigned one point for each of six risk indicators: household income below the federal poverty line, receipt of Temporary Assistance for Needy Families, caregiver report of income as insufficient to meet all needs, and primary caregiver without high school education or current employment.
Psychosocial outcomes were assessed annually from age 17 to 20 y. At each wave, we obtained youth self-reports of depressive symptoms (42) and substance use (31). For the latter, subjects reported their past-month cigarette, alcohol, and marijuana use and the number of times they drank alcohol to excess. Responses were made on seven-point scales with the categories 0, 1–2, 3–5, 6–9, 10–19, 20–39, and 40+. Responses to these four items were summed to form a substance use composite. Simultaneously, we obtained caregiver reports of youth aggressive behavior and internalizing symptoms (43). Cronbach’s α values on these instruments ranged from 0.82–0.85.
DNA Methylation.
When youth were age 22 y, phlebotomists went to their homes and collected antecubital blood. PBMCs were isolated through density-gradient centrifugation (Ficoll-Paque Media PM 400; GE Healthcare). Genomic DNA was extracted with Qiagen DNA Mini Kits, and quality was verified on an Agilent 2100 Bioanalyzer. Methylation profiling was then conducted by the University of Minnesota’s Genome Center, following the manufacturer’s protocol for the Illumina HumanMethylation 450 BeadChip. The resulting data were inspected for complete bisulfite conversion, and average β values for each targeted CpG residue were determined using the Illumina Genome Studio Methylation Module, Version 3.2; β values were calculated as the ratio of methylated probes to the sum of methylated and unmethylated probes, ranging from 0 (entirely unmethylated) to 1 (fully methylated). The resulting data were then cleaned using a Perl-based algorithm (44) to remove those β values with detection P values, an index of the likelihood that the observed sequence represents random noise, that were greater than 0.05. Nearly all probes (99.76%) yielded reliable data by this criterion.
Epigenetic Age Acceleration.
Two epigenetic aging metrics have been proposed, which use distinct targets, covariates, and formulas. Horvath’s clock was estimated with a publicly available R script, which aggregates methylation values from 353 CpG sites (27). Hannum’s clock was estimated by summing weighted methylation values from 71 CpG sites, using coefficients he validated for PBMCs (28).
Latent Class Growth Analyses.
To evaluate the convergence of psychosocial and epigenetic outcomes, we performed latent class growth analyses (33). First, to characterize trajectories of self-control and socioeconomic disadvantage from ages 17 to 19 y, we estimated a three-wave latent growth curve model with parallel outcomes. Linear models were fit with four individual growth parameters: two intercept parameters representing self-control and disadvantage at age 17 y and two linear slope parameters representing changes in these outcomes through age 19 y. Next, we used latent class growth analysis to estimate person-specific intercepts and trajectories and then clustered subjects into groups exhibiting similar patterns. Analyses were conducted using Mplus Version 7.2. Fit indices were obtained for models with two to six classes (SI Appendix, Table S3). Lower Akaike Information Criterion and Bayesian Information Criterion scores represent better-fitting models, whereas higher entropy scores reflect greater classification accuracy. To select a final solution, we considered these fit indices, along with theoretical parsimony and the size of resulting subgroups. In view of these criteria, a four-group model was selected, as detailed in Results. Next, we estimated a series of multigroup latent growth models, comparing the four groups’ trajectories of psychosocial outcomes from ages 17 to 20 y (SI Appendix, Table S5). Because epigenetic age acceleration was only measured at age 22 y, we used univariate ANOVAs to compare the groups with respect to this measurement (SI Appendix, Table S6).
Mediation Models.
To examine whether body mass or life stress might operate as pathways underlying skin-deep resilience, we estimated a series of mediation models (45). Body mass was measured during a home assessment and calculated as weight in kilograms divided by the square of height in meters. Life stress was assessed annually from age 17 to 19 y with an event checklist. Youth reported whether each of 12 events (e.g., death of a friend, parental divorce, serious injury) had occurred during the past 6 mo. The average count across waves was used to represent life stress.
Supplementary Material
Acknowledgments
This work was supported by National Institutes of Health Grants HD030588, HL108723, HL122328, DA027827, and DA19230.
Footnotes
The authors declare no conflict of interest.
This article is a PNAS Direct Submission.
See Commentary on page 10078.
This article contains supporting information online at www.pnas.org/lookup/suppl/doi:10.1073/pnas.1505063112/-/DCSupplemental.
References
- 1.de Ridder DT, Lensvelt-Mulders G, Finkenauer C, Stok FM, Baumeister RF. Taking stock of self-control: A meta-analysis of how trait self-control relates to a wide range of behaviors. Pers Soc Psychol Rev. 2012;16(1):76–99. doi: 10.1177/1088868311418749. [DOI] [PubMed] [Google Scholar]
- 2.Fujita K. On conceptualizing self-control as more than the effortful inhibition of impulses. Pers Soc Psychol Rev. 2011;15(4):352–366. doi: 10.1177/1088868311411165. [DOI] [PubMed] [Google Scholar]
- 3.Moffitt TE, et al. A gradient of childhood self-control predicts health, wealth, and public safety. Proc Natl Acad Sci USA. 2011;108(7):2693–2698. doi: 10.1073/pnas.1010076108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ayduk O, et al. Regulating the interpersonal self: Strategic self-regulation for coping with rejection sensitivity. J Pers Soc Psychol. 2000;79(5):776–792. doi: 10.1037//0022-3514.79.5.776. [DOI] [PubMed] [Google Scholar]
- 5.Wills TA, Stoolmiller M. The role of self-control in early escalation of substance use: A time-varying analysis. J Consult Clin Psychol. 2002;70(4):986–997. doi: 10.1037//0022-006x.70.4.986. [DOI] [PubMed] [Google Scholar]
- 6.Loeber R, et al. Findings from the Pittsburgh Youth Study: Cognitive impulsivity and intelligence as predictors of the age-crime curve. J Am Acad Child Adolesc Psychiatry. 2012;51(11):1136–1149. doi: 10.1016/j.jaac.2012.08.019. [DOI] [PubMed] [Google Scholar]
- 7.Caspi A, Wright BRE, Moffitt TE, Silva PA. Early failure in the labor market: Childhood and adolescent predictors of unemployment in the transition to adulthood. Am Sociol Rev. 1998;63:424–451. [Google Scholar]
- 8.Duckworth AL, Quinn PD, Tsukayama E. What No Child Left Behind Leaves Behind: The Roles of IQ and Self-Control in Predicting Standardized Achievement Test Scores and Report Card Grades. J Educ Psychol. 2012;104(2):439–451. doi: 10.1037/a0026280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Shonkoff JP, Garner AS. Committee on Psychosocial Aspects of Child and Family Health; Committee on Early Childhood, Adoption, and Dependent Care; Section on Developmental and Behavioral Pediatrics The lifelong effects of early childhood adversity and toxic stress. Pediatrics. 2012;129(1):e232–e246. doi: 10.1542/peds.2011-2663. [DOI] [PubMed] [Google Scholar]
- 10.Evans GW. The environment of childhood poverty. Am Psychol. 2004;59(2):77–92. doi: 10.1037/0003-066X.59.2.77. [DOI] [PubMed] [Google Scholar]
- 11.Braveman PA, Cubbin C, Egerter S, Williams DR, Pamuk E. Socioeconomic disparities in health in the United States: What the patterns tell us. Am J Public Health. 2010;100(Suppl 1):S186–S196. doi: 10.2105/AJPH.2009.166082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Duncan GJ, Brooks-Gunn J. Consequences of Growing Up Poor. Russell Sage Foundation; New York: 1997. [Google Scholar]
- 13.Statistics NCfH . Health, United States 2010. National Center for Health Statistics; Hyattsville, MD: 2011. [Google Scholar]
- 14.Haushofer J, Fehr E. On the psychology of poverty. Science. 2014;344(6186):862–867. doi: 10.1126/science.1232491. [DOI] [PubMed] [Google Scholar]
- 15.Heckman JJ. Schools, Skills, and Synapses. Econ Inq. 2008;46(3):289. doi: 10.1111/j.1465-7295.2008.00163.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mischel W. The Marshmallow Test: Mastering Self-Control. Little, Brown; New York: 2014. [Google Scholar]
- 17.Shonkoff JP. Protecting brains, not simply stimulating minds. Science. 2011;333(6045):982–983. doi: 10.1126/science.1206014. [DOI] [PubMed] [Google Scholar]
- 18.Brody GH, et al. Is resilience only skin deep? Rural African Americans’ socioeconomic status-related risk and competence in preadolescence and psychological adjustment and allostatic load at age 19. Psychol Sci. 2013;24(7):1285–1293. doi: 10.1177/0956797612471954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chen E, Miller GE, Brody GH, Lei MK. Neighborhood poverty, college attendance, and diverging profiles of substance use and allostatic load in rural African American youth. Clin Psychol Sci 2014 doi: 10.1177/2167702614546639. , 10.1177/2167702614546639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sellers SL, Neighbors HW, Zhang R, Jackson JS. The impact of goal-striving stress on physical health of white Americans, African Americans, and Caribbean blacks. Ethn Dis. 2012;22(1):21–28. [PubMed] [Google Scholar]
- 21.Richeson JA, Shelton JN. Negotiating interracial interactions: Costs, consequences, and possibilities. Curr Dir Psychol Sci. 2007;16:316–320. [Google Scholar]
- 22.Inzlicht M, McKay L, Aronson J. Stigma as ego depletion: How being the target of prejudice affects self-control. Psychol Sci. 2006;17(3):262–269. doi: 10.1111/j.1467-9280.2006.01695.x. [DOI] [PubMed] [Google Scholar]
- 23.James SA, Strogatz DS, Wing SB, Ramsey DL. Socioeconomic status, John Henryism, and hypertension in blacks and whites. Am J Epidemiol. 1987;126(4):664–673. doi: 10.1093/oxfordjournals.aje.a114706. [DOI] [PubMed] [Google Scholar]
- 24.Gross JJ, Levenson RW. Hiding feelings: The acute effects of inhibiting negative and positive emotion. J Abnorm Psychol. 1997;106(1):95–103. doi: 10.1037//0021-843x.106.1.95. [DOI] [PubMed] [Google Scholar]
- 25.Tomiyama AJ, et al. Low calorie dieting increases cortisol. Psychosom Med. 2010;72(4):357–364. doi: 10.1097/PSY.0b013e3181d9523c. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Geronimus AT. Deep integration: Letting the epigenome out of the bottle without losing sight of the structural origins of population health. Am J Public Health. 2013;103(Suppl 1):S56–S63. doi: 10.2105/AJPH.2013.301380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Horvath S. DNA methylation age of human tissues and cell types. Genome Biol. 2013;14(10):R115. doi: 10.1186/gb-2013-14-10-r115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Hannum G, et al. Genome-wide methylation profiles reveal quantitative views of human aging rates. Mol Cell. 2013;49(2):359–367. doi: 10.1016/j.molcel.2012.10.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Horvath S, et al. Obesity accelerates epigenetic aging of human liver. Proc Natl Acad Sci USA. 2014;111(43):15538–15543. doi: 10.1073/pnas.1412759111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Marioni RE, et al. DNA methylation age of blood predicts all-cause mortality in later life. Genome Biol. 2015;16:25. doi: 10.1186/s13059-015-0584-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Brody GH, Yu T, Chen YF, Kogan SM, Smith K. The Adults in the Making program: Long-term protective stabilizing effects on alcohol use and substance use problems for rural African American emerging adults. J Consult Clin Psychol. 2012;80(1):17–28. doi: 10.1037/a0026592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Cohen J, Cohen P, West SG, Aiken LS. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences. Lawrence Erlbaum; Mahwah, NJ: 2003. [Google Scholar]
- 33.Muthén B, Muthén LK. Integrating person-centered and variable-centered analyses: Growth mixture modeling with latent trajectory classes. Alcohol Clin Exp Res. 2000;24(6):882–891. [PubMed] [Google Scholar]
- 34.Wrosch C, Scheier MF, Miller GE. Goal Adjustment Capacities, Subjective Well-Being, and Physical Health. Soc Personal Psychol Compass. 2013;7(12):847–860. doi: 10.1111/spc3.12074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Johnson SE, Richeson JA, Finkel EJ. Middle class and marginal? Socioeconomic status, stigma, and self-regulation at an elite university. J Pers Soc Psychol. 2011;100(5):838–852. doi: 10.1037/a0021956. [DOI] [PubMed] [Google Scholar]
- 36.Vohs KD. Psychology. The poor’s poor mental power. Science. 2013;341(6149):969–970. doi: 10.1126/science.1244172. [DOI] [PubMed] [Google Scholar]
- 37.Muraven M, Baumeister RF. Self-regulation and depletion of limited resources: Does self-control resemble a muscle? Psychol Bull. 2000;126(2):247–259. doi: 10.1037/0033-2909.126.2.247. [DOI] [PubMed] [Google Scholar]
- 38.Barnes PJ, Adcock IM. Glucocorticoid resistance in inflammatory diseases. Lancet. 2009;373(9678):1905–1917. doi: 10.1016/S0140-6736(09)60326-3. [DOI] [PubMed] [Google Scholar]
- 39.Duncan GJ, Murnane J. Whither Opportunity? Rising Inequality, Schools, and Children’s Life Chances. Russell Sage Foundation; New York: 2011. [Google Scholar]
- 40.Humphrey LL. Children’s and teachers’ perspectives on children’s self-control: The development of two rating scales. J Consult Clin Psychol. 1982;50(5):624–633. doi: 10.1037//0022-006x.50.5.624. [DOI] [PubMed] [Google Scholar]
- 41.Brown JM, Miller WR, Lawendowski LA. In: Innovations in Clinical Practice: A Source Book. VandeCreek L, Jackson TL, editors. Professional Resource Press; Sarasota, FL: 1999. pp. 281–289. [Google Scholar]
- 42.Radloff LS. The CES-D scale: A self-report depression scale for research in the general population. J Appl Psychol Measure. 1977;1:385–401. [Google Scholar]
- 43.Achenbach TM, Rescorla LA. Manual for the ASEBA School-Age Forms & Profiles. Univ Vermont, Research Center for Children, Youth, & Families; Burlington, VT: 2001. [Google Scholar]
- 44.Dogan MV, et al. The effect of smoking on DNA methylation of peripheral blood mononuclear cells from African American women. BMC Genomics. 2014;15:151. doi: 10.1186/1471-2164-15-151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychol Methods. 2002;7(1):83–104. doi: 10.1037/1082-989x.7.1.83. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.