

Social and communication deficits are considered core features for children with autism spectrum disorders-ASD (American Psychiatric Association, 2012). Children with ASD including high functioning autism have lower levels of communication than typically developing children, and have difficulty with processing and interpreting social situations with peers, teachers and family members (Jones & Schwartz, 2009). Common signs related to these deficits include trouble relating to others or not appearing to have interest in others, avoiding eye contact and preferring to be alone, and problems understanding other people’s feelings and social cues. Some children with ASD seem interested in others but have difficulty knowing how to relate and communicate with others and express their emotions (Koegel, Koegel, Fredeen, & Gengoux, 2008; Cotugno, 2009; Reichow & Volkmar, 2010). Thus, research to identify approaches that enhance social skills and communication competence in natural settings continues to be at the forefront in the search for evidence-based practices (Goldstein, 2002; Guralnick, 1999; Kasari & Lawton, 2010; Koegel, Kuriakose, Singh, & Koegel, 2012; Reichow & Volkmar, 2010; Smith et al., 2007; Strain & Schwartz, 2001).
Of particular importance to improving the core deficits of children with ASD (social, communication, interpersonal skills) is the use of effective interventions within the context of natural settings and with typically developing peers (Kamps et al., 2002). Peer mediation through networks, or small groups of peers recruited to serve a role (e.g., facilitate activity engagement or reinforce play behaviors, tutor academics), is one example of an effective intervention that can naturally target social interactions (Bauminger, Solomon, Aviezer, Keung, Brown & Rogers, 2008; Garrison-Harrell, Kamps & Kravits, 1997; Haring & Breen, 1992; Kamps, Potucek, Lopez, Kravits, & Kemmerer, 1997; Kasari, Freeman, & Paparella, 2006; Koegel, Vernon et al., 2012; Parker & Kamps, 2011; Thiemann & Goldstein, 2004).
Much of the intervention research targeting social and communication skills for children with ASD incorporates the use of evidence-based practices including (a) written and picture cues, social scripts, and other visual representations of communication (Bryan & Gast, 2000; Ganz, Kaylor, Bourgeois, & Hadden, 2008; MacDuff, Ledo, McClannahan, & Krantz, 2007; Quill, 1997); and (b) direct instruction of targeted behaviors using social skills curricula (Bauminger, 2007; Goldstein, 2002; Gonzalez-Lopez & Kamps, 1997; Kamps et al., 2002; Lerner & Mikami, 2012; McMahon, Vismara, & Solomon, 2012). The use of text cues in the form of scripts and fading of scripts has research support for use with children with ASD (Krantz & McClannahan, 1993). For example, Brown, Krantz, McClannahan and Poulson (2008) used social scripts to increase verbal interactions for three children with ASD. The researchers were able to fade use of the scripts and demonstrated generalization to novel settings within natural environments (sporting goods store, convenience store, video store). Ganz and colleagues (Ganz et al., 2008) used social scripts and visual cues to increase context appropriate conversation with children with ASD and peers during academic and play activities in their school setting. Similarly, Spencer and Higbee (2012) used scripts to increase functional conversation skills including correct use of prepositions and conjunctions (e.g., “I love to play and paint with you.” “I love to paint with you because you’re fun.”) for a young girl with autism and confederate peers.
Several studies have combined these interventions with peers as change agents to improve social behaviors. Peer training was found effective for teaching peer models to use skills such as prompting, time delay, use of social scripts and text cues, and reinforcement in several studies (English, Goldstein, Shafer, & Kaczmarek, 1997; Kamps et al., 1997; Kohler, Greteman, Raschke, & Highnam, 2007; Morrison, Kamps, Garcia, & Parker, 2001; Pierce & Schreibman, 1997; Strain & Bovey, 2011; Thiemann & Goldstein, 2004; Woods & Poulson, 2006). For example, in the Kamps et al. (1997) study, peer networks supported three students with ASD during centers, recess, lunch and academic periods using visual cues, prompting, and reinforcement for engagement and appropriate social behaviors. Sample text cues used to request peer assistance during academic sessions were “Check my work, please.”, “May I have the ______?”, and “Help me.” Sample scripts during centers included “Let’s play this game.”, “My turn.”, and “Look at this book.” Results indicated improved social interaction and engagement during small group peer network activities.
Parker and Kamps (2011) taught two 7 and 8 year old children with autism to follow steps in a task analysis while participating in games, cooking, and eating in a restaurant with peers. Students with ASD and their peers also used social scripts consisting of sample conversational statements about the activities to increase communication during the groups (e.g., “This is a fun game.”, “It’s your turn.”, “What’s next in the recipe?”). Results of the intervention indicated improved task engagement and increased communication with peers even following fading of the scripts. Thiemann and Goldstein (2004) similarly used direct instruction, feedback, and written text cues to teach requests for information or items, niceties, compliments, suggestions, and secures for attention for five children with ASD and ten peers. Results showed improved social skills use, quality of child-peer interactions, teacher ratings of social skills, and acceptance and friendship ratings by peers. In addition, students decreased their reliance on adult prompting over time as well as inappropriate behaviors.
A range of intervention contexts, targeted skills, and social outcomes have been reported following peer inclusive groups and networks. Examples include peer social groups to improve joint attention and symbolic play in young children with autism (Kasari, et al., 2006; Koegel, Vernon, & Koegel, 2009; Pollard, Betz, & Higbee, 2012); the use of augmentative systems with peers (Garrison-Harrell, Kamps & Kravits, 1997; Kravits, Kamps, Carnazzo, & Potucek, 2002); social skills instruction to improve conversations and interactions with peers (Cotugno, 2009; Laugeson, Frankel, & Mogil, 2009; Morrison et al., 2002; Thiemann & Goldstein, 2004); and peer training to increase interactions during recess and recreational groups (Harper, Symon, & Frea, 2008; Kasari, Rotheram-Fuller, Locke, & Gulsrud, 2011; Lang et al., 2011; McFadden, Kamps, & Heitzman-Powell, 2012).
Findings for peer networks and social skills interventions have shown promising results; however, remaining gaps in the research preclude practical implementation (Kasari & Lawton, 2010; Koenig, De Los Rees, Cicchetti, Scahill, & Klin, 2009; Reichow & Volkmar, 2010). Limitations of the current evidence include the use of clinical settings for social skills interventions, often times without the benefit of typical peers; teaching discrete social behaviors without demonstrating generalization to functional use in natural environments; and loosely defined components of the intervention or lack of monitoring of the independent variable (Kasari & Lawton, 2010; Smith et al., 2007). This study seeks to address these issues through the use of a clearly defined, manualized peer network social skills intervention implemented in a natural setting with typical peers to teach socially functional target behaviors to children with ASD.
Purpose and Research Questions
The purpose of this study was to evaluate the impact of a peer network intervention for increasing the communicative acts of elementary students with ASD. The study adds to previous peer mediation social skills literature by (1) including scripted lessons for teachers to guide direct instruction of skills, (2) expanding targeted social skills to include conversations and turn taking, rather than the simple occurrence of ‘social interaction’ or ‘cooperative play’, and (3) monitoring of participants’ use of specific skills with direct observations and fidelity of the intervention groups. The study replicates prior research in the use of text cues and feedback within treatment sessions (Parker & Kamps, 2011; Thiemann & Goldstein, 2001; 2004); and application of intervention in natural settings with school staff as implementers and typical peers as peer network members (Kamps et al., 1997; 2002). The specific research question addressed by this study is: Does an explicit social skills instructional program combined with visual cues within the context of peer networks yield increased communication for participants with ASD?
Method
Participants, Setting, and Materials
Participants
Four children were chosen from a larger pool of participants who had been selected to participate in a randomized control trial evaluating the effectiveness of peer networks, following university Institutional Review Board approval for human subjects’ research. Seven participants were enrolled in the current year and these four exhibited the lowest and most stable levels of communication and so were included in the study. The participants had been previously diagnosed with ASD either through a clinical assessment or educationally based assessment. In order to be included in the study, participants had to display functional communication, make requests, and express 2–3 word phrases. Additionally, the ability to understand and respond to requests and directions was required. Relevant descriptive information and standard scores for each participant can be found in Table 1.
Table 1.
Participant Information
| Participant | Ethnic | Gender | Age in months | CARS | PPVT* | SRS** | Vineland Communication |
|---|---|---|---|---|---|---|---|
| 1 | White | M | 79 | 34 | 88 | 70 | 95 |
| 2 | White | M | 93 | 41 | 82 | 54 | 84 |
| 3 | White | M | 76 | 35 | 82 | 73 | 70 |
| 4 | White | M | 77 | 36.5 | 85 | 66 | 70 |
CARS=Childhood Autism Rating Scale score; PPVT=Peabody Picture Vocabulary Test standard score; Social Responsiveness Scale T score; Vineland Communication subtest standard score
Participant 1 was a 6 year old, first grade student who spent the majority of the day in general education, with the exception of speech therapy. He was on grade level academically and able to follow directions and classroom routines. He engaged in some interactions, initiated to peers on a limited basis, and briefly responded if approached by a peer and/or adult. Communications tended to be on perseverative topics, and he did not orient his body towards the person to whom he was responding or listen to their responses. The school’s speech language pathologist (SLP) was the interventionist for Participant 1.
Participant 2 was a 7 year old male who was repeating kindergarten. He had not received any services or interventions prior to entering kindergarten. He spent approximately two-thirds of his day in his general education classroom while the remainder occurred in a resource setting. He engaged in limited social interaction with peers and tended to be very serious and quiet. The few interactions he did engage in were limited to his restricted interests. Participant 2 had a severe articulation delay that further impacted his ability to communicate with his peers. His SLP was the interventionist.
Participant 3 was a 7 year old first grade student who was primarily served in a self-contained classroom due to challenging behavioral issues (e.g., elopement, aggression, and property destruction). He was at grade level but not always responsive to group instruction, due to attention problems. He engaged in little social interactions with peers but did initiate frequently to adults. Many of his social behaviors were related to restricted interests (for example, the same Frisbee® disk during recess, toys that made noises or electronic devices). The school-based SLP was also the interventionist for Participant 3.
Participant 4 was a 6 year old, first grade student. He was in a self-contained classroom for students with autism and attended physical education and art class with his general education peers. He was functioning below first grade level academically. The child rarely communicated with peers or adults, and his communication was limited to echolalia and learned scripted responses. Additionally, vocalizations were not purposefully directed toward others (i.e., eye contact, body position, using peers name). He had a long history of gastro-intestinal medical problems, affecting his school attendance. He received a combined intervention including speech and occupational therapy. Two paraprofessionals trained in the intervention procedure were the interventionists for Participant 4.
Four to six neuro-typical peers were recruited from each participant’s classroom and/or grade level to participate in the social network. Teachers nominated the children as ‘good role models’ for social and communication skills. Following obtaining informed consent from parents/guardian, the peers took turns participating in the social network sessions with two peers per session. Peers were taught prompting procedures during the social group utilizing the manual and scripted lessons and instructions. The training used direct instruction for teaching peers and the participants during group sessions (see intervention).
Training
The intervention was implemented by school staff trained in the manualized peer network procedure. Training, which was done by the researchers, occurred during a 3-hour workshop. Interventionists were provided with the necessary teaching materials including the manual. In addition to the workshop, research staff modeled the intervention in the school setting with the focus child and peers. The research staff modeled the first two lessons as each new skill was introduced (approximately every four weeks), and weekly feedback, coaching, and consultation continued throughout the course of the study.
Setting and Materials
All peer network treatment sessions (scripted teaching and free play) took place in typical settings including the speech therapy room and resource room. The focus child sat in between the two peers at a small table. The interventionist sat at the table only during instructional portions of the session during intervention. Games such as Ned’s Head®, Zingo®, and Memory® were utilized as well as puzzles, books and other cooperative activities available from the interventionists. Interventionists and participants chose activities for sessions. For Participants 1, 2, and 4 – two activities were available for many sessions and children were allowed to choose the activity during the free play time.
In addition to games, intervention session materials included a whiteboard with a visual schedule of the lesson; a teacher script for teaching each skill (see Figure 1); a visual text cue card for students with the name of the skill (e. g., Talk and Share) along with several phrases, such as “Here you go.” “May I have it? and “Thank you.”) (see Figure 2); and a skill feedback card, with 10–15 blank squares was used to reinforce and provide feedback on skill use to all children in the group.
Figure 1.
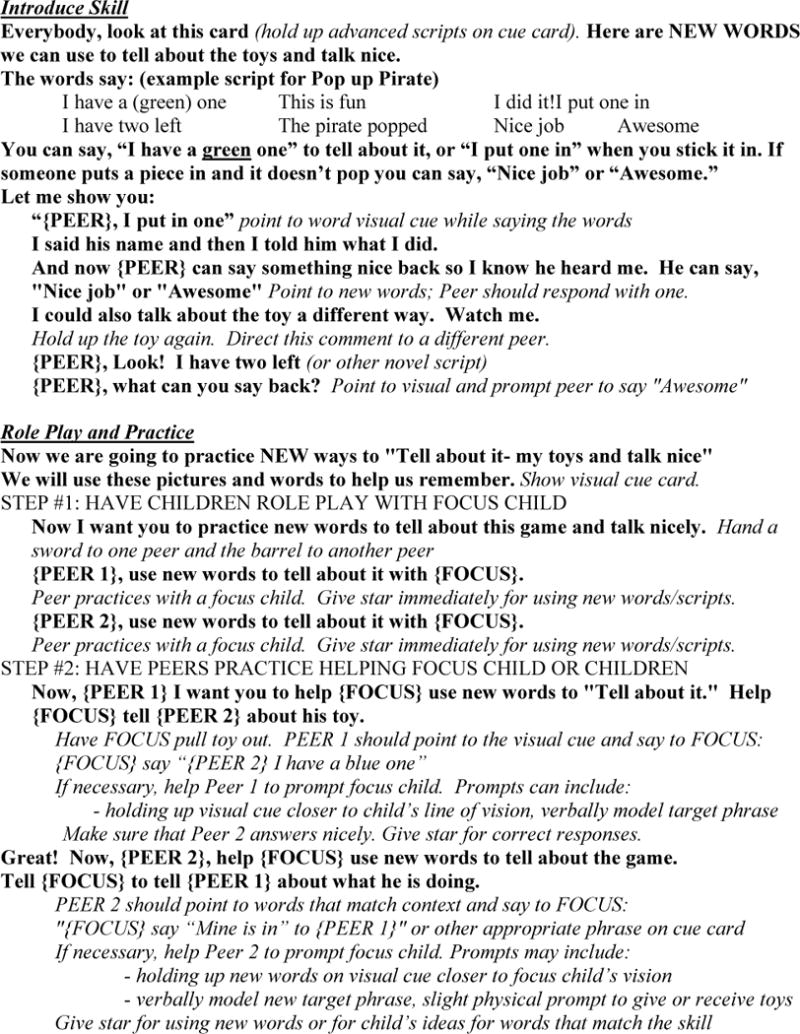
Excerpt from Teaching Script
Figure 2.
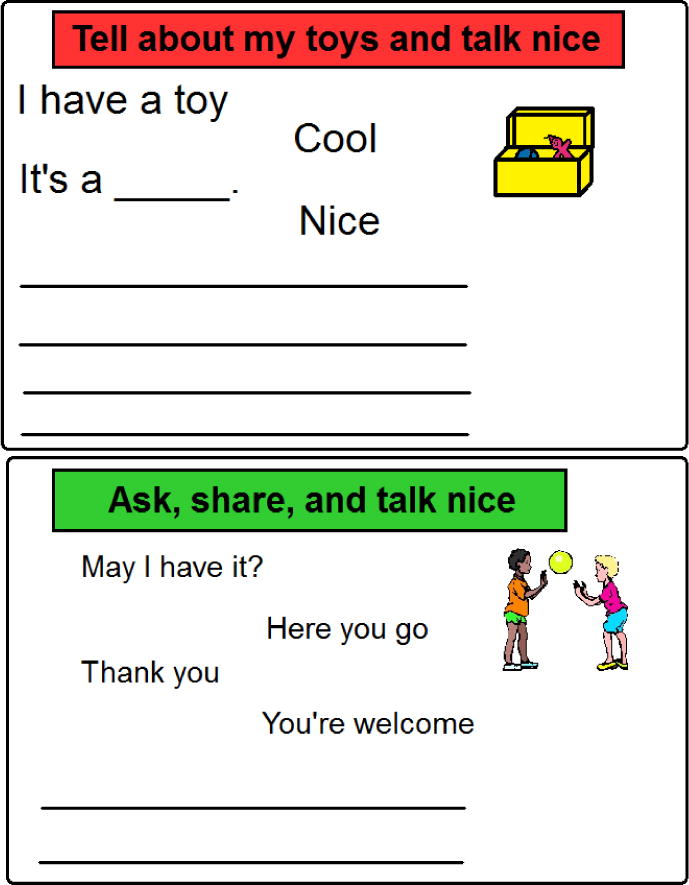
Sample Text Cues
Generalization setting probes were collected for Participants 1, 2, and 4 during naturally occurring activities in the general education classrooms, and at a different time than the treatment sessions. Activities included classroom centers or cooperative group sessions for all three participants and physical education classes during baseline and one follow-up probe for Participant 4. These probes were collected during baseline and following intervention sessions. Activities were those normally assigned by the general education teacher and similar during baseline and intervention conditions. Materials and procedures used during the network treatment sessions (teacher scripts, visual text cues, and reinforcement chart) were not available during generalization probes. Peers who participated in the networks were present during the generalization probes, but not necessarily in close proximity to the participants with ASD. Participant 3 was not included in activities in the general education classroom on a consistent basis, so generalization probes were not able to be collected.
Experimental Design and Measurement
A multiple-baseline single case design across participants was implemented to evaluate the impact of the intervention. The study was carried out over the course of three months with a maximum of three treatment sessions per week. The number of sessions per week varied due to school and classroom schedules (i.e., programs, school closings, holidays), and participant schedule changes (i.e., absences, related services). Participants 1 and 2 received 43 peer network sessions, Participant 3, 34 and Participant 4, 29. Each session consisted of 10-min of adult-led skill instruction using the social skills script, followed by a minimum of 10 to 15 minutes of free play during which data was collected. An additional five minutes were spent for feedback using the feedback chart, awarding of prizes for use of social-communication skills, and clean-up.
Measurement
Baseline data was collected for each participant in the same classroom in which the intervention occurred. The number of communicative acts, including initiations and responses, was the dependent measure. Forms of social-communication coded included sharing/requesting, commenting, turn-taking and response behaviors based on peer’s communication. An initiation was defined as beginning the communication sequence with a communication that was non-contingent to a peer’s previous comment and clearly targeted towards a peer or the group as a whole. A response was defined as a communicative act that began within 3 s of a peer’s communicative act and was clearly contingent on the peer’s communication (a response to an initiation by the peer). Verbalizations and communicative behaviors that were not distinctly intended for a peer were not coded as communicative acts. Thus, behaviors such as talking to objects, talking to the adult in the room, and other communication acts that did not indicate the communicative partner (e.g., eye contact, body orientation, or turn-taking and manipulating materials as part of the cooperative play, etc.) were not coded. Examples of this would be making a statement but appearing to be ‘talking to one self’ rather than communicating with a peer in the group (see Table 2 for definitions).
Table 2.
Operational Definitions of Social-Communicative Behaviors
| Dependent measure | Definition |
|---|---|
| Child Designation | |
| F (focus child) | A communicative act emitted by the participant |
| P (peer) | A communicative act emitted by a peer |
| Response Type | |
| I (initiation) | A communicative act directed to one peer or to the group as a whole that begins a new topic of conversation or is not in response to (within 3 seconds) ongoing communication between or action(s) of group members. |
| R (response) | A communicative act that is in response to or on topic with recent (within 3 sec) initiations or responses of other group members. |
| Social Behavior Definitions | |
| COM (Comment) | A communicative act that refers to ongoing events, items, or actions, but is not a compliment. Examples: “That’s a pirate.” “This is fun,” “I have a fish and an owl.” “I need one more for Zingo.” |
| RQ (Request/Share) | A communicative act whose function is to elicit information, action, or reciprocal communication from group member(s) (i.e., greetings). Examples: “May I have it?” “What did you get?” “Pass Ned’s Head.”, “Where’s the magnet?” |
| TT (Turn-taking) | A communicative act that refers to taking turns or going first, second, third etc. Examples: “Your turn,” “Whose turn?,” You go first.” |
| PLO (Play organizer) | A communicative act that functions to set up a game or activity or labels a general rule of the activity. Examples: “Let’s play Pop Up Pirate.” “You can pass out the cards.” “I’ll be the Rule Ranger.” “Let’s fill all the squares to get Zingo.” “You have to find two things with the magnifying glass.” |
| NIC (Nicety) | A comment that is complimentary. Niceties also include terms synonymous with “good manners” such as “Thank you” and “You’re welcome”. Examples: “Good idea”, “Thanks”, “Cool, you got it!”, “Well done”. |
| NonV (Non-verbal) | A non-verbal communicative act not accompanied by verbal behavior. Examples: waving, looking at a peer when requested to do so, shoulder-tapping, winking, gesturing toward an object or person. |
Noldus Observer XT software (2009) was utilized for data collection via personal digital assistants (PDA). Observers, which included investigators and research assistants trained in the data collection system utilized the Noldus software to record the frequency count of communicative behaviors and identify the type of behavior (e.g., initiation or response) and the functional communicative intent of that behavior (e.g., comment, request/share, play organizer, niceties, non-verbal gestures) that occurred. The use of the software allowed for time stamping of each recorded behavior to allow for accurate analysis of inter-observer agreement. Initiation and response behaviors were coded for both focus children and each peer conversational partner.
Reliability
Two investigators/research assistants trained in the data collection procedure simultaneously, yet independently, coded a minimum of 20% of data sessions across phases utilizing the Noldus Observer XT (2009) software. Time stamping of each recorded behavior allowed for accurate analysis of inter-observer agreement. Exact count-per-interval Inter-Observer Agreement (IOA), which is a percentage of intervals for which the same count of the target behavior was documented by both observers, was calculated for this study. Exact count-per-interval provides a highly precise measure of IOA for frequency count data IOA (Cooper, Heron, & Heward, 2007). The IOA was calculated first by separating each 10-min observation into 5 s intervals. An agreement was indicated for an interval when both observers indicated the same number of communicative acts. A disagreement was recorded for the interval if the count was not equal between the two observers. IOA was calculated by dividing the number of intervals with count agreement by the total number of intervals. Percent of agreement for total communicative acts for participants in baseline sessions ranged from 72–98% and percent of agreement for intervention sessions ranged from 67–97%. The overall mean percent of agreement was 86.9%. Reliability for peers’ total communicative acts was 84% in baseline and 78.2% during intervention (79.2% overall). Reliability for the descriptors of the types of communicative acts (e.g., sharing, commenting) was 87% in baseline and 89% during intervention sessions. Percent of agreement for focus child initiations averaged 90% in baseline and 89% in intervention sessions. The percent of agreement for focus child responses averaged 88% in baseline and 84% in intervention sessions. Reliability for communicative acts for peers averaged 84% in baseline (range, 75–94%) and 78% in intervention sessions (range, 65–89%).
Fidelity of Implementation
A procedural fidelity checklist was completed by research staff trained in the intervention procedures and use of the fidelity checklist. Treatment fidelity was assessed for the majority of the intervention sessions across participants. Twenty-four items on the checklist mirrored procedures from the manual including setting up materials and inclusion of 2 peers, introduction and discussion of the target skill (i.e., following the teacher script), role play practice, and appropriate use of prompting and the reinforcement system. Research staff also utilized the checklist to provide feedback to the interventionists and address issues with procedural integrity. Treatment fidelity was calculated by dividing the number of items completed accurately by the total number of items on the checklist. The average percentage of fidelity across participants was 85.6%, 90%, 78.5%, and 90.5%, respectively. Overall fidelity of implementation was 84%.
Procedures
Baseline
Baseline consisted of a 10-min free play session. During baseline, the focus child sat between two peers at a small table in a quiet room within the school. Three toys were placed on the table including such items as Ned’s Head®, a book, puzzles, and a Memory® game. If these items did not include preferred items, a preferred item was substituted for one of the non-preferred items. The children were told they had free play time. The parameters given for this time were “stay at the table” and “play nicely.” Once the 10-min free play session began, no further prompting or interaction occurred from the adult unless redirection was required due to a child not playing nicely or leaving the table. While the children were playing, a researcher trained in the coding procedures observed the play and coded focus child and peer communicative acts utilizing a PDA. All baseline sessions were video recorded using a small video camera on a tripod.
The systematic introduction of the intervention occurred for the first participant once baseline data for total communicative acts was stable and did not indicate an increasing trend. Subsequent participant’s intervention started once the baseline was stable and the proceeding participant’s intervention data demonstrated a stable improvement from baseline.
Intervention
Once the parameters for introducing the independent variable were met, the peer network social group began. As during baseline, the focus child sat between two peers at a small table. Peers rotated for each day of the week that social groups occurred (i.e., peers 1 and 2 on Monday, peers 3 and 4 on Wed, etc.). During the instruction part of intervention sessions, only one game was present to allow for scripted instruction. The instruction was comprised of four steps including: (1) systematic and direct instruction on the targeted skill, (2) scripted practice of the skill, (3) peer-mediated free play, and (4) review of performance and reinforcement. The whiteboard with the visual schedule was present and each time a step of the group was completed the interventionist crossed the step off the schedule. Each session lasted for 25–30 minutes. Each session began with the interventionist reviewing the group visual schedule as written on the whiteboard. Data collection occurred live or through use of video recordings during the 10-min free play portion of the intervention.
Direct instruction
During direct instruction of the social peer network group, the interventionist sat across from the focus child and peers. To begin the session, the interventionist reviewed the schedule, as written on the whiteboard. The interventionist then proceeded to provide instruction on the communication skill targeted for the session. Each skill was taught in order for 3–4 weeks: sharing and requesting, commenting about toys, commenting about friends’ toys, and play organizers. The interventionist followed a script to provide the instruction and relevant social communication examples (see excerpts Figure 1). Implementers were encouraged to “use their own language” and style as long as the main idea/task in the script was completed. The visual cue card was present, and the interventionist used this as a teaching strategy, modeling and practicing the target skill during instruction (see Figure 2). This portion of the intervention lasted for approximately 5–7 minutes.
Scripted practice
The scripted practice of the skill lasted for approximately 5 minutes and involved both focus child-adult practice and focus child-peer practice. During focus child-adult practice, the interventionist practiced the skill with the focus child and assisted the focus child in completing the fill-in-the-blank items on the visual cue card. The interventionist prompted the focus child by modeling correct expression of the text cues on the visual cue card (i.e., gaining attention of the child and pointing at words and phrases he could use). Then, the focus child and peers practiced utilizing the game provided. During this time each peer took turns playing with the focus child while the other peer provided prompts as needed to the focus child to use the appropriate words on the cue card. The interventionist provided instruction to the peers on how to prompt the focus child. Prompts included pointing to the cue card, full prompts (i.e., telling the focus child what to say), and physical prompts such as guiding the focus child’s hands to give an object to the other peer.
Peer-mediated free play
Data collection occurred during this 10 to 15-min segment of the intervention. Prior to free play, the interventionist explained to the participants that they were going to “practice using the new skill.” The interventionist showed the participants (peers and the focus children) the reinforcement card and explained they would earn a “smiley face” in an empty square every time someone used the skill. The interventionist then told the participants they could play and she then moved away from the table. Children had access to one to three games and toys during the free play time. During free play the interventionist prompted the peers to prompt the focus child if necessary, approximately once per minute. If the focus child did not respond to the peers, the interventionist provided a prompt.
Review of performance and reinforcement
Following free play, the interventionist returned to the table and displayed the reinforcement card. She pointed out the number of smiley faces earned. Additionally, the interventionist provided specific feedback on the participants’ performance, repeating phrases they had used that matched the target communication skill, or gave ideas for what they could say next time to increase rates of the skill. If all of the squares on the feedback/reinforcement card were filled, the peers and focus child were allowed to choose an item from the treasure box.
Data Analysis
To evaluate the impact of the intervention on increasing communicative acts of the focus child, both visual and statistical analysis of the data was utilized. Visual analysis of the graphically displayed data included evaluation of changes in variability, mean, and trend of the total communicative acts data. In addition, Tau effect size was calculated to quantify the magnitude of change that occurred between baseline and intervention for total communicative acts as well as number of initiations and responses separately. Tau is a “distribution free” effect size measure that is appropriate for time-order data series and is a means for quantifying visual analysis results (Parker & Vannest, 2012). The Tau method is a single subject, non-overlap effect size measure utilized with a known sampling distribution, allowing for calculation of p-values and confidence intervals. Unlike other nonoverlap methods, Tau also considers trend in the intervention phase, making it a more robust statistic than other non-overlap techniques (Parker, Vannest, & Davis, 2011; Parker & Vannest, 2012) such as percentage of non-overlapping data (PND) and improvement rate difference. The interpretation of Tau is the same as improvement rate difference, that is Tau effect sizes equal to or less than .50 are best described as minimal change; Tau = .50 but less than .70 can be described as moderate; and Tau effect sizes greater than .70 are described as large. Tau was calculated based on an AB contrast for each participant and for the overall design utilizing the singlecaseresearch.org Tau calculator.
Results
Total Communicative Acts
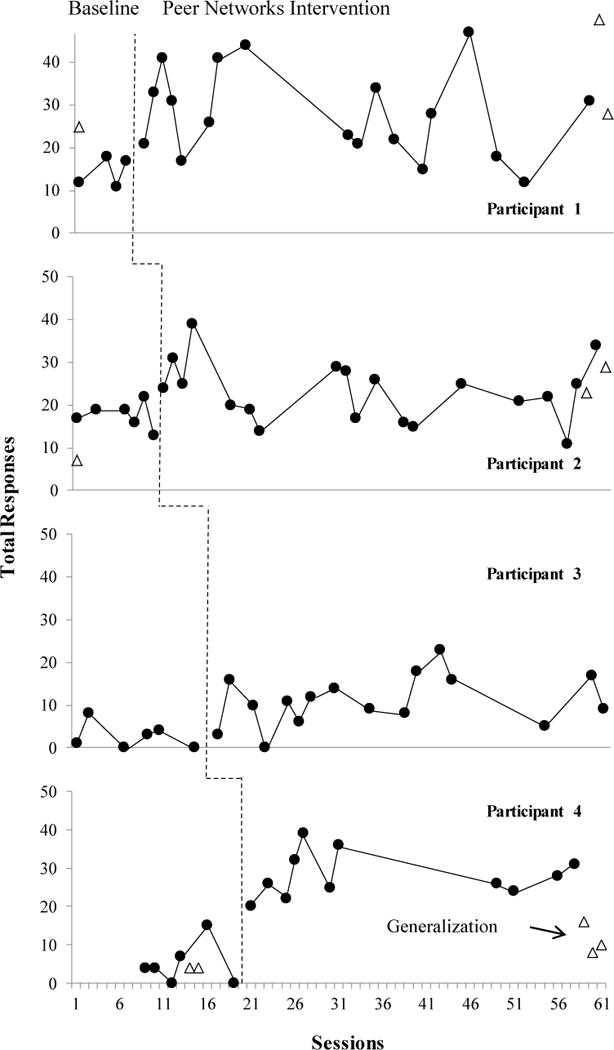
Results for all participants’ total communicative acts are graphically displayed in Figure 3. The x-axis indicates the session and the y-axis indicates the total number of focus child communicative acts (both initiations and responses). As is denoted by the phase change line, introduction of the peer network social skills group was systematically staggered across participants, with four demonstrations of change at different points in time. The change is consistent across participants as the number of communicative acts increases by the second data point. With the exception of the baseline for Participant 1, all phases exceed the suggested 5 data points per phase (Kratochwill et al., 2010).
Figure 3.
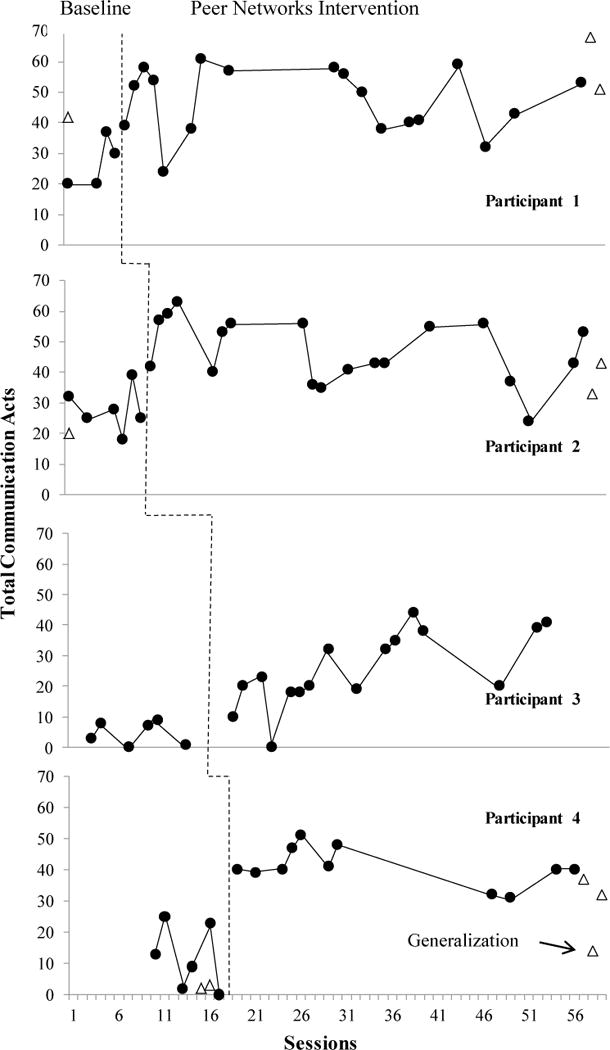
Total Communication Acts Across Participants
The intervention was first implemented with Participant 1, and his data is presented in the top panel of Figure 3. The mean number of his communicative acts rose from 27, with a range of 20–37 in baseline to 47, with a range of 24–61, during intervention. Although the data is somewhat variable, during both intervention and baseline, visual analysis indicates minimal overlap between phases and a clear positive mean shift with the introduction of the intervention. Statistical analysis indicates a large, statistically significant increase in communicative acts (see Table 3).
Table 3.
Participants Tau Effect Size and Relevant Confidence Intervals for Total Communications
| Participant | Tau Effect Size | P-value | 90% CI | |
|---|---|---|---|---|
|
| ||||
| Lower Limit | Upper Limit | |||
|
|
||||
| 1 | .92 | <.00 | .34 | 1.41 |
| 2 | .84 | <.00 | .38 | 1.30 |
| 3 | .88 | <.00 | .40 | 1.34 |
| 4 | 1.00 | <.00 | .50 | 1.50 |
| Weighted Average | .90 | <.00 | .58 | 1.57 |
The intervention was introduced for Participant 2 when baseline was stable and Participant 1 demonstrated a clear increase in communicative acts. Visual analysis of the graphical display (Figure 3, 2nd panel) indicates an intercept gap and a positive mean shift from baseline with the introduction of the intervention. Although the number of communicative acts varied from session to session, overlap of intervention with baseline is minimal (4 data points) and the mean (46.9, range = 24–63) was well above baseline (M = 27.8, range = 18–32). Again, the resulting Tau (see Table 3) indicates a large, statistically significant, positive magnitude of change with the implementation of the peer networks social group intervention.
Once data for Participant 2 indicated stable responding above baseline, the intervention began for Participant 3. As can be seen by review of Figure 3 (3rd panel), he demonstrated few communicative acts prior to the intervention (baseline M = 4.7, range = 0–9). Introduction of the intervention resulted in an increase in communicative acts (M = 25.6, range = 0–44) with only one data point overlapping with baseline. Again, a large, statistically significant increase in communicative acts between baseline and intervention occurred.
As is demonstrated in Figure 3, Participant 4 also demonstrated an increase in communicative acts during the intervention phase of the study. Visual analysis of his baseline data (bottom panel) indicates variable but low rates of communicative acts (M = 12, range = 0–25). The intercept gap upon introduction of the intervention is visually evident, with higher rates of communicative acts (M = 40.8, range = 31–51) for all intervention sessions when compared to baseline. The large Tau effect size (Table 3) indicates a statistically significant increase in the number of communicative acts from baseline to intervention.
Initiations and Responses
Although evidence of experimental control was based on total communicative acts, and not initiations and responses separately, the data were further desegregated and analyzed to provide a more thorough description of changes in these two social communication behaviors between baseline and intervention. The number of initiations and responses is depicted in Figures 4 and 5 respectively.
Figure 4.
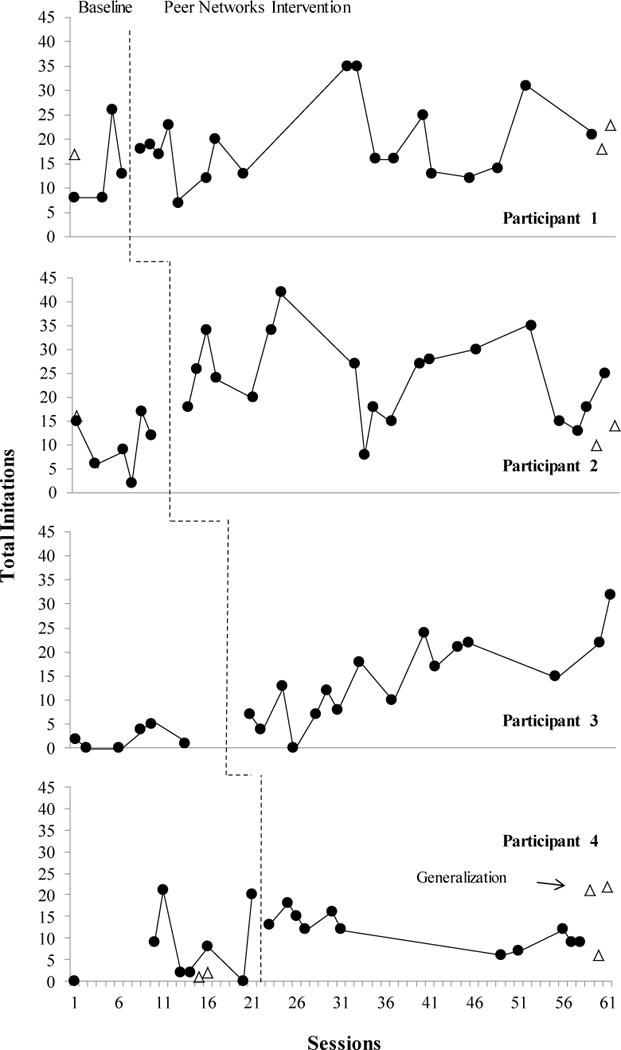
Total Initiations Across Participants
Figure 5.
Total Responses Across Participants
Figure 4 depicts the number of initiations during baseline and the peer networks conditions for all participants. Visual inspection indicates that initiations increased for all participants but less so for Participant 4, and not to the extent that total communications changed. Participant 1 averaged 13.7 (range 8–26) initiations to peers during baseline, with a slight increase to 19.3 (range 7–35) during the social groups. Participant 2 averaged 10.1 (range 2–17) initiations in baseline and doubled to a M of 23.7 (range 8–42) during social networks. Participant 3 showed a low rate of initiations in baseline (M = 2, range = 0–5) with an increase to a mean of 14.5 (range 0–24). Initiations for Participant 4 increased slightly from baseline (M = 7, range = 0–21) to intervention (M= 12.7, range = 7–20).
In order to obtain a quantitative measure of the degree of change that occurred in the number of initiations and responses between baseline and intervention, Tau was calculated for each participant and then aggregated to obtain an overall Tau effect size. Results for initiations are displayed in Table 4. Statistical analysis indicates small to large changes across participants with an overall large effect size (see Table 4). Although only 2 of the four participants yielded statistically significant increases in the number of initiations following implementation of the intervention, the overall changes across all four participants yielded statistically significant (p <.00) increases in initiations.
Table 4.
Participants Tau Effect Size and Relevant Confidence Intervals for Initiations
| Participant | Tau Effect Size | P-value | 90% CI | |
|---|---|---|---|---|
|
| ||||
| Lower Limit | Upper Limit | |||
|
|
||||
| 1 | .42 | .25 | −.16 | .91 |
| 2 | .82 | <.01 | .35 | 1.27 |
| 3 | .85 | <.01 | .34 | 1.28 |
| 4 | .53 | .07 | .03 | 1.03 |
| Weighted Average | .66 | <.00 | .42 | .91 |
Figure 5 depicts the number of responses to peers by the children with autism during baseline and the peer networks conditions for all participants. Visual inspection indicates that responses increased during the peer networks intervention. Participant 1 averaged 14.5 (range of 11–18) responses to peers during baseline, with an increase to 28.1 (range 12–44) during the social groups. Participant 2 averaged 17.6 (range 13–22) responses in baseline and a mean of 23.2 (range 11–39) during social networks. Participant 3 showed a low rate of responses in baseline (M = 2.6, range = 0–8) with an increase to a mean of 11.1 (range 0–23). Participant 4 increased from baseline (M = 5.0, range = 0–15) to intervention as well (M= 28.1, range = 20–39).
Table 5 displays Tau effect size and relevant confidence intervals for increases in number of responses between baseline and intervention conditions for each participant. All participants, with the exception of Participant 2, demonstrated large, statistically significant increases in the number of responses between baseline and intervention. Additionally the overall Tau effect size for increases in the number of responses indicates a large, statistically significant, magnitude of change in number of responses (see Table 5).
Table 5.
Participants Tau Effect Size and Relevant Confidence Intervals for Responses
| Participant | Tau Effect Size | P-value | 90% CI | |
|---|---|---|---|---|
|
| ||||
| Lower Limit | Upper Limit | |||
|
|
||||
| 1 | .82 | .01 | .28 | 1.36 |
| 2 | .44 | .11 | −.02 | .90 |
| 3 | .78 | <.00 | .31 | 1.24 |
| 4 | 1 | <.00 | .49 | 1.48 |
| Weighted Average | .74 | <.00 | .50 | .99 |
Generalization probes
Generalization probes in centers in the general education classrooms are depicted in Figures 3–5 using triangles as data points representing total communication acts (initiations and responses). For Participant 1, probes showed a high level of communication in the one baseline probe, 42, with an increase to 68 and 51 following intervention. Participant 2 increased from baseline (20) to follow-up, 33 and 43. Participant 4 increased from baseline PE probes of 2–3 communications to 37 and 14 in centers and 32 in PE following interventions. The majority of communications for Participants 1 and 2 were responses to peers, while the majority of communications for Participant 4 were initiations.
Social-Communication Descriptors
Table 6 presents the type of social-communication behaviors across conditions for the participants. These data represent both initiation and responses to peers. As previously indicated the total number of communications increased with the implementation of the peer networks condition, and increases are reflected across the different types of communications. The majority of communication types for Participants 1, 3 and 4 were comments in both conditions, with the second most frequent communication being requests. Requests to peers increased 2–10 times for all participants and more so for Participants 1 and 2. Comments and requests increased equally for Participant 3. Comments increased by half for Participants 1 and 2 and occurred twice as often for Participant 4 during peer networks. Turn-taking, helping and play organizing types of remarks occurred at low rates across all conditions.
Table 6.
Communication Descriptors across Conditions and Participants
| Participant | Condition | Requests/Shares | Comments | Niceties | Turns |
|---|---|---|---|---|---|
| 1 | baseline peer networks |
2.0 14.1 |
22.0 29.3 |
0.7 1.3 |
2.7 2.6 |
| 2 | baseline peer networks |
5.3 10.4 |
19.3 27.5 |
0.0 3.2 |
2.7 2.4 |
| 3 | baseline peer networks |
0.8 12.4 |
2.2 12.1 |
0.0 3.4 |
0.0 0.1 |
| 4 | baseline peer networks |
1.7 12.4 |
9.3 15.9 |
0.0 8.4 |
0.0 0.2 |
Note: Play organizer and non-verbal behaviors occurred with low frequency across conditions.
Peer Communications
As depicted in Table 7, peers for Participants 1, 3, and 4 showed increases to the children with ASD during the peer network condition. Peers for Participant 1 increased initiations and responses equally by 12 per session on average. Participant 3’s peers increased initiations to him by 8 and responses by 10 on average per session. Peers for Participant 4 increased the most with 18 more initiations and 20 more responses on average per session. Peers for Participant 2 initiated to him during baseline at levels similar to intervention for the other participants (M= 20) and increased their responses from 13.7 to 18 during intervention.
Table 7.
Peer Initiations, Responses and Total Communications with the Focus Children with ASD
| Peers for Participant # | Condition | Peer Initiations | Peer Responses | Total Communications |
|---|---|---|---|---|
| 1 | baseline peer networks |
9.7 22.2 |
13.3 25.9 |
23 48 |
| 2 | baseline peer networks |
20 21.9 |
13.7 18.3 |
33.7 40.2 |
| 3 | baseline peer networks |
3.8 12.2 |
1.2 10.2 |
5 22.4 |
| 4 | baseline peer networks |
4.0 22.8 |
2.3 22.6 |
6.3 45.4 |
Social Validity
Following completion of the peer networks study, the implementers were given a 15-item Teacher/Implementer Satisfaction Survey in an effort to evaluate the social validity of the intervention. The items evaluated time commitment, adequacy of researcher support, feasibility of implementation, ease of the program, and perceived benefits of the program for both the focus child and peers. The first 12-items required the respondent to rate questions utilizing a 5-point likert scale with 1 meaning strongly disagree and 5 meaning strongly agree. Ninety-percent of the items across respondents were rated as “strongly agree” while the other 10% was rated as agree. Overall, school personnel indicated the intervention was feasible in terms of ease, time, and necessary resources. The respondents indicated that they had observed improvements in the focus child’s interactions with both trained and non-trained peers. Three respondents strongly agreed and the other agreed that they had adequate resources to implement the peer networks intervention within their daily school schedules.
The remaining three items were open answer questions asking for suggestions regarding perceived need for additional resources, materials, and suggestions for enhancing the intervention. Suggestions generally focused on ways to expand the intervention such as collaboration with other teachers, incorporating the intervention into settings throughout the building, and exploring service delivery methods for the intervention throughout elementary and secondary school.
Discussion
Social communication skills are an important area of intervention for young children with ASD. Although a number of positive social outcomes have been reported following peer training interventions for this population, there continues to be a need for evidence-based practices to improve specific communication skills to promote successful interactions with peers in school-based settings. In the current study, four 1st grade aged children with ASD participated in peer networks with a group of typically developing classmates. The networks were implemented three times per week for 25–30 minutes, and children played popular early elementary school games. With implementation of the peer networks and direct teaching of communication skills, all four participants showed significant increases over baseline levels for total communications during treatment sessions. Increases for initiations were notable for two participants whereas improvements in responses were large for three of the participants.
This single-subject design study with four systematic demonstrations of change at different points in time contributes to the evidence of the effectiveness of teaching communication skills with trained peer partners. Results confirmed prior research indicating that social skills interventions for young children with ASD generally improve children’s communicative behaviors (Kamps et al., 2002; Kasari & Lawton, 2010; Reichow & Volkmar, 2010). This study and prior research has demonstrated the effective use of peer models as change agents for improving social behaviors (Bauminger et al., 2008; Kasari et al., 2006; Koegel, Vernon et al., 2012; Odom et al., 1999; Parker & Kamps, 2011; Strain & Bovey, 2011; Thiemann & Goldstein, 2004; Wang, Cui, & Parrila, 2011).
The inclusion of small groups of peers to facilitate participation, and to increase social communicative interactions for children with ASD is highly relevant to settings with large numbers of typically developing peers such as schools. This is important for several reasons. First, typically developing children are the natural community for children with ASD. Improving the ability of children with ASD to learn from their peers, and in turn for peers to learn how to engage in more successful communication with children with ASD is socially valid for all children. In addition, school resources are limited and increasing the number of persons able to assist and enhance social communication opportunities (e.g., facilitating, prompting, reinforcing) takes advantage of peers as a valuable resource. Peers who come in contact with children with ASD in school environments can naturally influence their behaviors. The use of peer networks with the training provided by the school staff is one way to shape and influence positive child-peer interactions (e.g., increased cooperation, sharing, and having conversations). Furthermore, without this training, opportunities for children to practice important social skills in natural settings may be missed – and contribute to an increased gap in social communication competence and performance between children with and without ASD. The data on peers’ behaviors (see Table 6) documented the level of initiations and responsiveness of the peers during free play in baseline and during the peer networks condition. Increases in behaviors for peers of Participants 1, 3 and 4 and slight increases in behaviors for peers of Participant 2 indicated their learning to interact on a more frequent basis with their classmates with ASD. This provides a fidelity measure of peer mediation, that is peer initiations and responses are trained as an important component of the networks.
Several important features of the intervention are noteworthy. The school staff implemented the social groups, that is, three speech language pathologists and one paraprofessional received in-service training on peer network implementation. In many social skills intervention studies the curricula is implemented in clinical settings and by persons other than those having daily or frequent contact with the children (e.g., Cotugno, 2009). A related finding was the high level of fidelity for implementers, averaging 84% overall. This is desirable in that the intervention is more likely to be replicated in other school settings by different staff members. Several procedures may have contributed to the high rate of implementation fidelity. We found that outlining instructional or teaching steps in a social script to be very helpful in guiding interventionists to facilitate the groups. The scripts gave precise narrative for each section of the group: introducing the skills for the session, role play between the children, free play with prompting through the peers during games and activities, and feedback from the teacher during and at the end of the sessions. Scripts were practiced during the initial three hour school staff training, and the research staff also modeled the first two lessons as each new skill was introduced (approximately every four weeks). Implementers were able to follow the scripts with fidelity. Interventionists also had choices regarding the games to use during the sessions, and what to provide for the reinforcement. Children were also allowed to choose the activity during the free play time. Providing children a choice, especially if preferred activities, has been reported to positively influence successful peer interactions for young children with autism (Wolfberg & Schuler, 1993). Participant 3 was sometimes given a choice, but often the group was provided with one activity during the free play. The speech language pathologist reported this was more desirable for the child as transitions to new activities were sometimes difficult and triggered inappropriate behaviors.
Text cues in the form of pictures and words also seemed to increase children’s acquisition of social communication behaviors as they served as a visual prompt to use the skills during free play with peers. Interventionists referred to the text cues repeatedly during the teaching portion of the group and pointed to them during free play to prompt peers to prompt the children with autism to use the skills. They reported and we anecdotally observed that the majority of the children began to say the words and phrases without referring to the text cues fairly quickly. The interventionists also reported that children began to use the phrases during other times of the day, and they expanded to using novel phrases related to the target communication skills. These findings support and extend prior research demonstrating the effectiveness of visual text cues and scripts for children with ASD (Ganz et al., 2008; MacDuff et al., 2007; Morrison et al., 2002; Thiemann & Goldstein, 2001; 2004). Text and visual cues capitalize on reported cognitive strengths children have in processing visual as opposed to auditory information to teach functional communication skills (Goldstein et al, 2007; Thiemann & Goldstein, 2001). The text cues matched the communicative context, allowed for frequent repetition of targeted skills, and an appropriate ‘script’ for both children with autism and their peers to follow. In addition, attempts at communicating are better understood, especially for children with low intelligibility as was the case for one child. Providing children with repeated practice of functional communication skills in a supportive, adult-guided environment potentially lays a stronger foundation to learn new language that can be then transferred to less structured, peer-led activities across the school day.
Another important component of the intervention was use of feedback to participants during the sessions in the form of stars or smiley faces on a chart, and access to the treasure box at the end of the sessions when children had filled all the boxes. Small prizes (e.g., stickers, small tablets, tops, koosh balls, rings) were rewarding to children over the months of the study. Participant 3 also was able to earn reinforcement 1–2 times during the social group, while the other participants earned access to the treasure box at the end of the session. A more frequent rate of attention to appropriate behaviors was needed to maintain his participation and interactions with peers.
Although the aim of this study was to evaluate changes in total communications with the introduction of the intervention, the breakdown of data based on initiations and responses does contribute additional information. Three of the four participants demonstrated statistically large increases in the production of responses while the other participant’s increases are best described as statistically small. Two of the four participants demonstrated large increases in the production of initiations whereas statistically smaller changes were noted for the other two participants. Production of initiations is inherently more challenging for individuals with ASD thus even small improvements can be meaningful from both a practical and social standpoint.
In addition, changes in trends and means as well as observations indicated clinical significance as well as statistical significance for the total levels of communications, and nice changes for either initiations or responses or both for participants. From a practical standpoint the level of variability and less change in initiations and the continued use of treatment without fading instruction would indicate that there is a continued need for social skills instruction for the participants. The lower rates of communication for Participant 3 would also indicate a need for more continuous intervention and more opportunities and prompting for skill use in general education settings.
Limitations
Findings must be viewed in consideration of several limitations of the study. The small number of participants could be considered a weakness to the study, in relation to generalizing findings to other children with ASD. However, multiple baseline designs are appropriate and recommended in early phases of intervention research with children with autism (Smith et al., 2007), and results can strongly influence the clinical decision making process for applied research (Zhan & Ottenbacher, 2001). In addition, there was a great deal of variability in communicative acts across sessions. This trend in social data is common across intervention studies for children with autism (e.g., Koegel et al., 2009; Thiemann & Goldstein, 2004), and likely due to a number of variables including activities selected during sessions and peers rotating in the network (i.e., peers rotated in pairs across the three weekly sessions, six peers total, but two different ones for each day of the week). The use of the Tau effect sizes were calculated to account for the overlapping nature (variability) of the data, with positive findings indicating significance across conditions for total communication. It is not possible to rule out the impact of time or “increased familiarity” with the peers as another explanation for increased interaction. The multiple baseline design does control for this to a certain extent, however measures of students not participating in peer networks as a comparison group would provide additional support for the intervention effects. In addition, because both peer behaviors (initiations and responses to the children with ASD) as well as the focus children’s behaviors increased during intervention, it is not possible to determine how much change was related to improved peers’ ability to engage the children. However, this reciprocity is a salient feature of peer mediation and again supports the utility of peers as intervention agents for children with ASD.
Although experimental control was obtained for total communicative acts (i.e., stable or low communication acts during baseline and clear changes when the intervention was implemented in a staggered manner across participants), the study would be strengthened if this were extended to responses and initiations as well. Consequently, the results for changes in initiations and responses must be viewed with caution. Future studies that specifically focus on the use of peer networks to increase initiations and/or responses separately are suggested. Given the increases in initiations were statistically small for 2 of the 4 participants, the inclusion of more specific initiation strategies as a component of the social skills instruction may be beneficial.
Another limitation includes the lack of component analysis. With use of a package intervention with multiple components (direct skill instruction, feedback, rewards), it is unknown which procedure or combinations are causing the effects. In addition, the study lacked an analysis of the quality of more extended interactions or conversational communication behaviors during free play. Analysis of this nature, such as what could be obtained from transcribing and coding conversations based on the variety and content of different topics discussed, would provide further information regarding the impact of the peer networks intervention on these important social communication variables as the children’s language skills improve. It is possible that the quality as well as quantity of social communication behaviors increased, but data were collected live and only a few sessions were video-taped for later review. This level of analysis in future studies could help guide intervention revisions and communication goal setting for verbal children with ASD.
Limited data were collected for generalization of skill use outside of sessions, and maintenance data over time were not collected. Anecdotal reports were positive, but multiple generalization probes in novel settings with peers are recommended in future social skills intervention studies. Teacher satisfaction ratings of the intervention and its effects were high, but these high ratings could have been influenced by social desirability (e.g., wanting to please the researchers, to indicate positive findings of their efforts with students). High ratings by all four teachers in different schools, however, would not indicate this to be the case.
Conclusion
The study demonstrated positive outcomes following implementation of peer networks and structured social communication skills interventions using visual text cues and feedback for first grade children with autism. Social communication skills improved over baseline levels for all participants. Future research is warranted to further study intervention components to improve qualitative aspects of communication (Jones & Schwartz, 2009); cognitive skills that impact learning new social behaviors such as executive function (Kasari & Lawton, 2010); and programming for generalization to novel settings and peers (Spencer & Higbee, 2012).
Acknowledgments
The research was funded by the Institute of Education Sciences, Department of Education (R324A090091). Opinions expressed herein are those of the authors and do not necessarily reflect the position of the funding agency. We gratefully acknowledge the participating teachers, students, and families for their time and ongoing support.
Contributor Information
Debra Kamps, Email: dkamps@ku.edu, University of Kansas, Juniper Gardens Children’s Project, 444 Minnesota Avenue, Kansas City, KS 66101.
Rose Mason, Email: rmason519@ku.edu, University of Kansas, Juniper Gardens Children’s Project, 444 Minnesota Avenue, Kansas City, KS 66101.
Kathy Thiemann-Bourque, Email: Thiemann@ku.edu, University of Kansas, Juniper Gardens Children’s Project, 444 Minnesota Avenue, Kansas City, KS 66101.
Sarah Feldmiller, Email: sfeldmiller@ku.edu, University of Kansas, Juniper Gardens Children’s Project, 444 Minnesota Avenue, Kansas City, KS 66101.
Amy Turcotte, Email: amyturcotte@ku.edu, University of Kansas, Juniper Gardens Children’s Project, 444 Minnesota Avenue, Kansas City, KS 66101.
Todd Miller, Email: tmiller3@ku.edu, University of Kansas, Juniper Gardens Children’s Project, 444 Minnesota Avenue, Kansas City, KS 66101.
References
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM-5) Washington, DC: Author; 2012. [Google Scholar]
- Bauminger N. Brief report: Group social-multimodal intervention for HFASD. Journal of Autism and Developmental Disorders. 2007;37:1605–1615. doi: 10.1007/s10803-006-0246-3. [DOI] [PubMed] [Google Scholar]
- Bauminger N, Solomon M, Aviezer A, Heung K, Brown J, Rogers S. Friendship in high-functioning children with autism spectrum disorder: Mixed and non-mixed dyads. Journal of Autism and Developmental Disorders. 2008;38:1211–1229. doi: 10.1007/s10803-007-0501-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown J, Krantz P, McClannahan L, Pulson C. Using script fading to promote natural environment stimulus control of verbal interactions among youth wit autism. Research in Autism Spectrum Disorders. 2008;2:480–497. [Google Scholar]
- Bryan L, Gast D. Teaching on-task and on-schedule behaviors to high-functioning children with autism via picture activity schedules. Journal of Autism and Developmental Disorders. 2000;30(6):553–567. doi: 10.1023/a:1005687310346. [DOI] [PubMed] [Google Scholar]
- Cooper JO, Heron TE, Heward WL. Applied Behavior Analysis. 2. Upper Saddle River, NJ: Pearson; 2007. [Google Scholar]
- Cotugno A. Social competence and social skills training and interventin for children with autism spectrum disorders. Journal of Autism and Developmental Disorders. 2009;39:1268–1277. doi: 10.1007/s10803-009-0741-4. [DOI] [PubMed] [Google Scholar]
- English K, Goldstein H, Shafer K, Kaczmarek L. Promoting interactions among preschoolers with and without disabilities: Effects of a buddy skills-training program. Exceptional Children. 1997;63:229–243. [Google Scholar]
- Ganz J, Kaylor M, Bourgeois B, Hadden K. The impact of social scripts and visual cues on verbal communication in three children with autism spectrum disorders. Focus on Autism and Other Developmental Disabilities. 2008;23:79–94. [Google Scholar]
- Garrison-Harrell L, Kamps D, Kravits T. The effects of peer networks on social-communicative behaviors for students with autism. Focus on Autism and Other Developmental Disabilities. 1997;12:241–254. [Google Scholar]
- Goldstein H. Communication intervention for children with autism: A review of treatment efficacy. Journal of Autism and Developmental Disorders. 2002;32(5):373–396. doi: 10.1023/a:1020589821992. [DOI] [PubMed] [Google Scholar]
- Goldstein H, Schneider N, Thiemann K. Peer-mediated social communication intervention: When clinical expertise informs treatment development and evaluation. Topics in Language Disorders. 2007;27:182–199. [Google Scholar]
- Gonzalez-Lopez A, Kamps D. Social skills training to increase social interaction between children with autism and their peers. Focus on Autism and Other Developmental Disabilities. 1997;12:2–14. [Google Scholar]
- Guralnick M. CHDD researchers’ intervention program fosters social competence in young children with developmental delays. Center on Human Development and Disability Newsletter. 1999;12:3–8. [Google Scholar]
- Haring TG, Breen CG. A peer-mediated social network intervention to enhance the social integration of persons with moderate and severe disabilities. Journal of Applied Behavior Analysis. 1992;25(2):319–333. doi: 10.1901/jaba.1992.25-319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harper C, Symon J, Frea W. Recess is time-in: Using peers to improve social skills of children with autism. Journal of Autism and Developmental Disorders. 2008;38:312–323. doi: 10.1007/s10803-007-0449-2. [DOI] [PubMed] [Google Scholar]
- Jones C, Schwartz I. When asking questions is not enough: An observational study of social communication differences in high functioning children with autism. Journal of Autism and Developmental Disorders. 2009;39:432–443. doi: 10.1007/s10803-008-0642-y. [DOI] [PubMed] [Google Scholar]
- Kamps D, Potucek J, Dugan E, Kravits T, Gonzalez-Lopez A, Garcia J, Carnazzo K, Morrison L, Garrison-Kane L. Peer training to facilitate social interaction for students with autism. Exceptional Children. 2002;68:173–187. [Google Scholar]
- Kamps D, Potucek J, Gonzalez-Lopez A, Kravits T, Kemmerer K. The use of peer networks across multiple settings to improve interaction for students with autism. Journal of Behavioral Education. 1997;7:335–357. [Google Scholar]
- Kasari C, Freeman S, Paparella T. Joint attention and symbolic play in young children with autism: A randomized controlled intervention study. Journal of Child Psychology and Psychiatry. 2006;47:611–620. doi: 10.1111/j.1469-7610.2005.01567.x. [DOI] [PubMed] [Google Scholar]
- Kasari C, Lawton K. New directions in behavioral treatment of autism spectrum disorders. Opinions in Neurology. 2010;23(2):137–143. doi: 10.1097/WCO.0b013e32833775cd. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kasari C, Rotheram-Fuller E, Locke J, Gulsrud A. Social networks and friendships at school: Comparing children with and without ASD. Journal of Autism and Developmental Disorders. 2011;41(5):533–544. doi: 10.1007/s10803-010-1076-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koegel L, Koegel R, Fredeen R, Gengoux G. Naturalistic behavioral approaches to treatment. In: Chawarska K, Klin A, Volkmar F, editors. Autism spectrum disorders in infants and toddlers: Diagnosis, assessment, and treatment. New York: Guilford Press; 2008. pp. 207–242. [Google Scholar]
- Koegel L, Kuriakose S, Singh A, Koeel R. Improving generalization of peer socialization gains in inclusive school settings using initiations training. Behavior Modification. 2012;36:361–377. doi: 10.1177/0145445512445609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koegel R, Vernon T, Koegel L. Improving social initiations in young children with autism using reinforcers with embedded social interactions. Journal on Autism and Developmental Disabilities. 2009;39:1240–1251. doi: 10.1007/s10803-009-0732-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koegel LK, Vernon TW, Koegel RL, Koegel BL, Paullin AW. Improving social engagement and initiations between children with autism spectrum disorders and their peers in inclusive settings. Journal of Positive Behavior Interventions. 2012;14(4):220–227. doi: 10.1177/1098300712437042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koenig K, De Los Reyes A, Cicchetti D, Scahill L, Klin A. Group intervention to promote social skills in school-age children with pervasive developmental disorders: Reconsidering efficacy. Journal of Autism and Developmental Disorders. 2009;39:1163–1172. doi: 10.1007/s10803-009-0728-1. [DOI] [PubMed] [Google Scholar]
- Kohler F, Greteman C, Raschke D, Highnam C. Using a buddy skills package to increase the social interactions between a preschooler with autism and her peers. Topics in Early Childhood Special Education. 2007;27:155–163. [Google Scholar]
- Krantz P, McClannahan L. Teaching children with autism to initiate to peers: Effects of a script-fading procedure. Journal of Applied Behavior Analysis. 1993;26:121–132. doi: 10.1901/jaba.1993.26-121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kratochwill TR, Hitchcock J, Horner RH, Levin JR, Odom SL, Rindskopf DM, et al. Single-Case design technical documentation. What Works Clearinghouse. 2010 Retrieved from http://ies.ed.gov/ncee/wwc/pdf/wwc_scd.pdf.
- Kravits T, Kamps D, Carnazzo K, Potucek J. Increasing communication skills for an elementary-aged student with autism using the Picture Exchange Communication System. Journal of Autism and Developmental Disabilities. 2002;32:225–230. doi: 10.1023/a:1015457931788. [DOI] [PubMed] [Google Scholar]
- Lang R, Kuriakose S, Lyons G, Mulloy A, Boutot A, Britt C, Caruthers S, Ortega L, O’Reilly M, Lancioni G. Use of school recess time in the education and treatment of children with autism spectrum disorders: A systematic review. Research in Autism Spectrum Disorders. 2011;5:1296–1305. [Google Scholar]
- Laugeson E, Frankel F, Mogil C. Parent-assisted social skills training to improve friendships in teens with autism spectrum disorders. Journal of Autism and Developmental Disabilities. 2009;39:595–606. doi: 10.1007/s10803-008-0664-5. [DOI] [PubMed] [Google Scholar]
- Lerner M, Mikami A. A preliminary randomized controlled trial of two social skills interventions for youth with high-functioning autism spectrum disorders. Focus on Autism and Developmental Disabilities. 2012;27:147–157. [Google Scholar]
- MacDuff J, Ledo R, McClannahan L, Krantz P. Using scripts and script-fading procedures to promote bids for joint attention by young children with autism. Research in Autism Spectrum Disorders. 2007;I:281–290. [Google Scholar]
- McFadden B, Kamps D, Heitzman-Powell L. Unpublished master’s thesis. University of Kansas; 2012. The Effects of a Peer-mediated socialskills intervention on the social communication behavior of children with autism at recess. [Google Scholar]
- McMahon CM, Vismara LA, Solomon M. Measuring changes in social behavior during a social skills intervention for higher-functioning children and adolescents with autism spectrum disorder. Journal of Autism and Developmental Disorders. 2012 doi: 10.1007/s10803-012-1733-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morrison L, Kamps D, Garcia J, Parker D. Peer mediation and monitoring strategies to improve initiations and social skills for students with autism. Journal of Positive Behavior Interventions. 2001;3:237–250. [Google Scholar]
- Odom S, McConnell S, McEvoy M, Peterson C, Ostrosky M, Chandler L, Spicuzza R, Skellinger A, Creighton M, Favazza P. Relative effects of interventions supporting the social competence of young children with disabilities. Topics in Early Childhood Special Education. 1999;19:75–91. [Google Scholar]
- Parker D, Kamps D. Teaching children with autism to use a task analysis to acquire functional skills in multiple settings. Focus on Autism and Developmental Disorders. 2011;26:131–142. [Google Scholar]
- Parker RI, Vannest KJ. Bottom up analysis of single-case research designs. Journal of Behavioral Education. 2012;21(3):254–265. [Google Scholar]
- Pierce KL, Schriebman L. Using peer trainer to promote social behavior in autism: Are they effective at enhancing multiple social modalities? Focus on Autism and Other Developmental Disabilities. 1997;12:207–218. [Google Scholar]
- Pollard J, Betz A, Higbee T. Script fading to promote unscripted bids for joint attentin in children with atuism. Journal of Applied Behavior Analysis. 2012;45:387–393. doi: 10.1901/jaba.2012.45-387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Quill K. Instrucitonal considerations for youing children with autism: The rationale for visually cued instruction. Journal of Autism and Developemtnal Disorders. 1997;27:697–714. doi: 10.1023/a:1025806900162. [DOI] [PubMed] [Google Scholar]
- Reichow B, Volkmar F. Social skills interventions for individuals with autism: Evaluation for evidence-based practices within a best evidence synthesis framework. Journal of Autism and Developmental Disorders. 2010;40(2):149–166. doi: 10.1007/s10803-009-0842-0. [DOI] [PubMed] [Google Scholar]
- Smith T, Scahill L, Dawson G, Guthrie D, Lord C, Odom S, Rogers S, Wagner A. Designating research studies on psychosocial interventions in autism. Journal of Autism and Developmental Disorders. 2007;37:354–366. doi: 10.1007/s10803-006-0173-3. [DOI] [PubMed] [Google Scholar]
- Strain P, Bovey E. Randomized, controlled trial of the LEAP model of early intervention for young children with autism spectrum disorders. Topics in Early Childhood Special Education. 2011;31:133–154. [Google Scholar]
- Spencer T, Higbee T. Using transfer of stimulus control technology to promote generalization and spontaneity of language. Focus on Autism and Developmental Disabilities. 2012;27:225–236. [Google Scholar]
- Strain P, Schwartz I. Applied behavior analysis and the development of meaningful social relations for young children with autism. Focus on Autism and Developmental Disabilities. 2001;16:120–128. [Google Scholar]
- Thiemann K, Goldstein H. Social stories, written text cues, and video feedback: Effects on social communication of children with autism. Journal of Applied Behavior Analysis. 2001;34:425–446. doi: 10.1901/jaba.2001.34-425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thiemann K, Goldstein H. Effects of peer training and written text cueing on social communication of school-age children with pervasive developmental disorder. Journal of Speech, Language, and Hearing Research. 2004;47:126–144. doi: 10.1044/1092-4388(2004/012). [DOI] [PubMed] [Google Scholar]
- Wang S, Cui Y, Parrila R. Meta-analysis of social skills interventions of single-case research for individuals with autism spectrum disorders: Results from three-level HLM. Journal of Autism and Developmental Disorders. 2012 doi: 10.1007/s10803-012-1726-2. [DOI] [PubMed] [Google Scholar]
- Wolfberg PJ, Schuler AL. Integrated play groups: A model for promoting the social and cognitive dimensions of play in children with autism. Journal of Autism and Developmental Disorders. 1993;23(3):467–489. doi: 10.1007/BF01046051. [DOI] [PubMed] [Google Scholar]
- Woods J, Poulson C. The use of scripts to increase the verbal initiation of children with developmental disabilities to typically developing peers. Education & Treatment of Children. 2006;29:437–457. [Google Scholar]
- Zhan S, Ottenbacher K. Single subject research designs for disability research. Disability Rehabilitation. 2001;23:1–8. doi: 10.1080/09638280150211202. [DOI] [PubMed] [Google Scholar]