

Abstract
The Cox-maze procedure for the restoration of normal sinus rhythm, initially developed by Dr. James Cox, underwent several iterations over the years. The main concept consists of creating a series of transmural lesions in the right and left atria that disrupt re-entrant circuits responsible for propagating the abnormal atrial fibrillation rhythm. The left atrial appendage is excluded as a component of the Maze procedure. For the first three iterations of the Cox- maze procedure, these lesions were performed using a surgical cut-and-sew approach that ensured transmurality. The Cox-Maze IV is the most currently accepted iteration. It achieves the same lesion set of the Cox- maze III but uses alternative energy sources to create the transmural lesions, potentially in a minimally invasive approach on the beating heart. High-frequency ultrasound, microwave, and laser energy have all been used with varying success in the past.
Today, bipolar radiofrequency heat or cryotherapy cooling are the most accepted sources for creating linear lesions with consistent safety and transmurality. The robust and reliable nature of these energy delivery methods has yielded a success rate reaching 90% freedom from atrial fibrillation at 12 months. Such approaches offer a significant long-term advantage over catheter-based ablation, especially in patients having longstanding, persistent atrial fibrillation with characteristics such as dilated left atrial dimensions, poor ejection fraction, and failed catheter ablation. Based on these improved results, there currently is significant interest in developing a hybrid ablation strategy that incorporates the superior transmural robust lesions of surgical ablation, the reliable stroke prevention potential of epicardial left atrial appendage exclusion, and sophisticated mapping and confirmatory catheter-based ablation technology. Such a minimally invasive hybrid strategy for ablation may lead to the development of multidisciplinary “Afib teams” to obtain optimal long-term sinus rhythm control. This article provides an overview of current surgical strategies for patients with atrial fibrillation and addresses the two main goals in its management.
Keywords: surgical ablation, atrial fibrillation, maze procedure

Basel Ramlawi, M.D.

Walid K. Abu Saleh, M.D.
History and Evolution of Surgical Atrial Fibrillation Ablation
In addition to alleviating symptoms, management of AF has two primary goals: optimizing cardiac output through rhythm or rate control, and decreasing the risk of cerebral and systemic thromboembolism (STE) with minimal increase in the risk of intra- and extracranial bleeding. Achieving these two goals can be less than straight forward than simply alleviating symptoms. A simplified proposed strategy for managing persistent and paroxysmal atrial fibrillation is illustrated in Figure 1. Unfortunately, several studies have shown that even when resumption of sinus rhythm (SR) is possible, patients are still at an increased risk of stroke and STE.1,2 It is thus currently recommended to prescribe a modality for stroke risk reduction based on stroke risk assessment, commonly via the CHADS2 or CHADS-VASC score, regardless of the rhythm attained.
Figure 1.

Proposed simplified strategy for management of persistent and paroxysmal atrial fibrillation. CHADS2 score of 1 is controversial whether anticoagulation is necessary. The CHA2DS2VASc is used by others. Renal failure not included in either system is also considered a risk factor for stroke and systemic thromboembolism.
**For all atrial fibrillation patients undergoing cardiac surgery. Discontinuation of anticoagulation after LAA exclusion is still controversial, but is reasonable if LAA complete exclusion is confirmed at 3 months after surgery and/or patient is at high-risk for anticoagulation.
***MIS epicardial LAA exclusion preferred when patient can tolerate general surgery, not a redo stemotomy/left thoracotomy and with good pulmonary functions. MIS: minimally invasive surgery; AVN: atrioventricular node; STE: systemic thromboembolism; INR: international normalized ratio; TTR: time in therapeutic range; LAA: left atrial appendage.
The decision whether to control rhythm or rate has been extensively studied. Results show that superiority of either strategy over the other is minimal and inconsistent.1–3 Rhythm control is more difficult to achieve with increasing age and left atrial size.4,5 Also, the duration of AF is directly proportional to the rates of failed cardioversion, suggesting that AF begets AF, probably through structural or conductance alterations of myocardial substrates over time.6 Rate control alone is usually preferred with asymptomatic chronic AF patients, especially those older than 65 years; this is partly to simplify their pharmaceutical management, since antiarrhythmic drugs (AAD) have significant drug interactions and these patients are typically already on a number of other medications.
The benchmark surgery for AF is the Cox-maze (CM) procedure, serially published by Cox and colleagues during the late 1980s and early 1990s.7,8 By cutting and sewing, the procedure interrupts all potential myocardial substrates for re-entrance and AF signal propagation while creating a “maze” of functioning atrial myocardium, through which normal impulses can travel from the SAN to the AVN. The initial procedure was effective, with freedom from AF greater than 94% at 12 months, but was associated with significant chronotropic incompetence and high rates of pacemaker implantations.9 Serial modifications to address these issues and to technically simplify the procedure have been developed, culminating in the CM-III procedure.10
A major criticism of the CM-III that hindered its widespread use was its complexity and technical difficulty. Alternating bradyarrythmias and tachyarrhythmias are other problems that have been described, especially with exercise and other forms of stress. These symptoms, however, improve with autonomic reinnervation over time.20 Moreover, with extensive atrial scarring, restoration of synchronized atrial contraction does not necessarily lead to restoration of atrial functional contraction and may not help much in patients with ventricular diastolic dysfunction.12 These issues seem to be true for most cut-and-sew techniques in general, and thus are less commonly adopted in recent years. Another criticism of all ablation strategies on an arrested heart is the inability to identify the exact propagation pathways in specific patients, which necessitates a rather extensive set of empiric lesions to ensure interruption of any potential substrate.
The advent of energy-based ablation devices to replace the original cut-and-sew technique lead to development of the CM-IV.13,14 In this CM adaptation, myocardial ablation is most commonly done using a combination of bipolar radiofrequency epicardially and cryoablation endocardially. Cryoablation is generally less deforming to the cardiac fibrous skeleton and is thus used near valvular annuli and trigones. Cryoablation is performed using cardiopulmonary bypass (CPB) for concomitant surgery because the immense heat sink of circulating intracavitary blood can absorb the energy, making it difficult or even impossible to render a complete freeze of the endocardial tissue. The CM-IV procedure lesions are similar to those of the CM-III, but the use of these alternative energy sources allows for minimally invasive lesions to be performed on a beating heart without the use of CPB.
Surgical Technique
The CM-IV procedure can be divided into right atrial and left atrial lesions. The left atrial lesions include circular lesions around the antrum of the pulmonary veins to complete pulmonary vein isolation, usually with bipolar radiofrequency lamps. Left atrial floor and roof ablation lines are then performed to link the pulmonary vein lesions, which is generally done with cryoablation. Other ablation lines are then created to link those lesions to the mitral valve annulus and the left atrial appendage (LAA). Exclusion of the LAA can be performed surgically or via a reliable device (e.g., the AtriClip®, AtriCure, Inc., West Chester, OH), leading to complete vascular and electrical LAA isolation. Right atrial lesions are then performed including lines to the right atrial appendage, tricuspid valve annulus, and the superior and inferior vena cava. A major advantage of surgical cryoablation and radiofrequency lines is the robust and continuous nature of these lesions compared to catheter-based ablation. Ultimately, regardless of the approach, reliable transmural lesions are the backbone of any successful AF ablation strategy.
For lone AF, the CM-IV procedure can be performed through bilateral mini-thoracotomy incisions or via a video-assisted thoracoscopic approach. Ultimately, regardless of the approach, reliable trans-mural lesions are the backbone of any successful AF ablation strategy.
The CM-IV procedure is simpler, and clamp times for concomitant surgeries were reduced from a mean of 122 minutes with CM-III to 92 minutes with CM-IV, and for lone AF from a mean of 93 minutes with CM-III to 41 minutes with CM-IV.22–24 The CM-IV proved to be successful in regaining SR but not as efficacious as CM-III. A study of 100 patients undergoing CM-IV for lone persistent AF reported an 84% freedom of AF and AAD at 2 years.15 Another study of 282 AF patients undergoing CM-IV with concomitant cardiac surgery reported a 78% freedom of AF and AAD at 1 year.5 Although these numbers seem to be lower than those reported for CM-III at longer follow-ups, one can argue that patients were significantly different, and definitions for success of rhythm control were not standardized in most of the CM-III reports. Propensity score matching comparing the two procedures showed similar rates of freedom from AF at 1 year (Table 1).16 Interestingly, the study did not report any decrease in morbidity with CM-IV compared to CM-III (Figure 2).
Table 1.
Early and late outcomes of the propensity matched cut-and-sew (CM III) versus ablation-assisted (CM IV) groups

Figure 2.
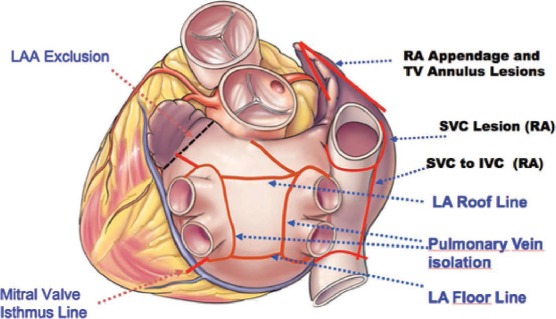
Complete set of atrial lesions as done in the Cox-maze IV procedure.
Effectiveness of the Hybrid Approach
A recent advance in AF rhythm control has been the use of a hybrid ablation strategy that capitalizes on advantages of existing methods. The staged hybrid ablation procedure allows for the completion of a full CM-IV procedure through a minimally invasive approach followed by radiofrequency catheter-based mapping and “touch-up” ablation of any residual gaps 6 to 8 weeks later (Figure 3). Initial results of such a strategy have been encouraging, showing greater than 85% sinus rhythm at 1 year in patients with long-standing persistent AF, reduced LV function or multiple comorbidities who have failed catheter-based ablation.
Figure 3.

Schematic drawing of ablation lines performed in the LA during a hybrid approach. Epicardial lines: 1, pulmonary vein isolation; 2, roof line; 3, inferior line; 4, line between the superior line and the left fibrous trigone; 5, connecting the line from the superior PV and the LAA; 6, line from the right inferior PV to the CS; 7, superior vena cava isolation; 8, intercaval line. Endocardial lines: a, mitral isthmus line; b, cavotricuspid line; *, ablation of complex fractionated atrial electrogram (CFAE). LA, left atrial; PV, pulmonary vein; LAA, LA appendage; CS, coronary sinus; MV, mitral valve. (Reproduced with permission from Gelsomino S, Van Breugel HN, Pison L, et al. Hybrid thoracoscopic and transvenous catheter ablation of atrial fibrillation. Eur J Cardiothorac Surg 2014; 45:401–7).
A recent meta-analysis by Gelsomino et al reported that bipolar radiofrequency energy yields better results in AF.17 Published results range from 85.7% to 92% in studies employing bipolar radiofrequency and from 36.8% to 88.9% in those using monopolar radiofrequency. However, studies published to date on the hybrid approach using bipolar radiofrequency energy have included rather diverse patient groups, small samples, and extremely heterogeneous methodologies.17
Hybrid thoracoscopic and transvenous catheter ablation of long-standing persistent AF shows extremely encouraging midterm results, which may represent an important and possibly more effective alternative to repeated radiofrequency catheter ablation therapy. Such “AF team” multidisciplinary collaboration may prove to be the strategy required to achieve optimal results in a complex condition such as longstanding AF. Advantages of the hybrid AF approach are summarized in Table 2.
Table 2.
Advantages of the hybrid AF approach

Complications during the surgical part of the procedure are mostly related to the learning curve and probably should be expected on introduction of the surgical component during development of, and transition to, a hybrid AF treatment protocol. Of the two hybrid approaches, the staged hybrid approach offers several advantages over the simultaneous hybrid procedure.18 Randomized multicenter clinical trials with long-term follow-up are needed to confirm the likely superiority of staged hybrid procedures over simultaneous procedures and over repeated catheter ablations using currently available novel technologies. A list of completed studies of hybrid AF ablation is shown in Table 3.
Table 3.
List of reported hybrid AF studies

Conclusion
A major shortcoming of surgical ablation studies is that the literature is heterogeneous with inconsistencies in the types of patients studied, the indications, the lesion sets, the energy devices used, and very importantly, the outcome definitions. This makes results difficult to interpret and comparing different strategies problematic. We generally regard the CM-III to be the gold standard, to which other surgical and catheter-based procedures should be compared. Randomized controlled trials comparing CM-III to other lesion sets and techniques would be optimal. Given the recent interest and improved outcome with hybrid ablation strategies, there is significant need for a randomized trial comparing these multidisciplinary approaches to traditional epicardial (surgery) or endocardial (percutaneous) procedures.
Conflict of Interest Disclosure: Dr. Ramlawi is the national principal investigator of the AtriClip Stroke Study and has industry relationships with AtriCure, Inc., Baxter, REPLICor Inc., and the Sorin group.
Footnotes
CM III, Cox-maze III procedure; CM IV, Cox-maze IV procedure. Reprinted with permission from Lall, S.,. Melby, S., Voeller, R., et al. The effect of ablation technology on surgical outcomes after the Cox-maze procedure: A propensity analysis. J Thorac Cardiovasc Surg. 2007;133:389–396.
AF, atrial fibrillation; LA, left atrial; PVI, pulmonary vein isolation; CS, coronary sinus.
Reprinted with permission from Driver, K. and Mangrum, J. Hybrid approaches in atrial fibrillation ablation: why, where and who? J Thorac Dis. 2015 Feb; 7: 159–164.
References
- 1.Van Gelder IC, Hagens VE, Bosker HA, Kingma JH, Kamp O, Kingma T, Said SA, Darmanata JI, Timmermans AJ, Tijssen JG, Crijns HJ. A comparison of rate control and rhythm control in patients with recurrent persistent atrial fibrillation. N Engl J Med. 2002;347:1834–1840. doi: 10.1056/NEJMoa021375. [DOI] [PubMed] [Google Scholar]
- 2.Wyse DG, Waldo AL, DiMarco JP, Domanski MJ, Rosenberg Y, Schron EB, Kellen JC, Greene HL, Mickel MC, Dalquist JE, Corley SD. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med. 2002;347:1825–1833. doi: 10.1056/NEJMoa021328. [DOI] [PubMed] [Google Scholar]
- 3.Hohnloser SH, Kuck KH, Lilienthal J. Rhythm or rate control in atrial fibrillation--pharmacological intervention in atrial fibrillation (piaf): A randomised trial. Lancet. 2000;356:1789–1794. doi: 10.1016/s0140-6736(00)03230-x. [DOI] [PubMed] [Google Scholar]
- 4.Ad N. The quest to identify predictors for success and failure after the cox-maze procedure for the treatment of atrial fibrillation. J Thorac Cardiovasc Surg. 2010;139:117–118. doi: 10.1016/j.jtcvs.2009.07.054. [DOI] [PubMed] [Google Scholar]
- 5.Damiano RJ, Jr., Schwartz FH, Bailey MS, Maniar HS, Munfakh NA, Moon MR, Schuessler RB. The cox maze IV procedure: Predictors of late recurrence. J Thorac Cardiovasc Surg. 2011;141:113–121. doi: 10.1016/j.jtcvs.2010.08.067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wijffels MC, Kirchhof CJ, Dorland R, Allessie MA. Atrial fibrillation begets atrial fibrillation. A study in awake chronically instrumented goats. Circulation. 1995;92:1954–1968. doi: 10.1161/01.cir.92.7.1954. [DOI] [PubMed] [Google Scholar]
- 7.Cox JL, Canavan TE, Schuessler RB, Cain ME, Lindsay BD, Stone C, Smith PK, Corr PB, Boineau JP. The surgical treatment of atrial fibrillation. Ii. Intraoperative electrophysiologic mapping and description of the electrophysiologic basis of atrial flutter and atrial fibrillation. J Thorac Cardiovasc Surg. 1991;101:406–426. [PubMed] [Google Scholar]
- 8.Cox JL, Schuessler RB, Boineau JP. The surgical treatment of atrial fibrillation. I. Summary of the current concepts of the mechanisms of atrial flutter and atrial fibrillation. J Thorac Cardiovasc Surg. 1991;101:402–405. [PubMed] [Google Scholar]
- 9.Cox JL, Schuessler RB, Lappas DG, Boineau JP. An 8 1/2-year clinical experience with surgery for atrial fibrillation. Ann Surg. 1996;224:267–273. doi: 10.1097/00000658-199609000-00003. discussion 273–265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cox JL, Jaquiss RD, Schuessler RB, Boineau JP. Modification of the maze procedure for atrial flutter and atrial fibrillation. Ii. Surgical technique of the maze iii procedure. J Thorac Cardiovasc Surg. 1995;110:485–495. doi: 10.1016/S0022-5223(95)70245-8. [DOI] [PubMed] [Google Scholar]
- 11.Pasic M, Musci M, Siniawski H, Edelmann B, Tedoriya T, Hetzer R. Transient sinus node dysfunction after the cox-maze iii procedure in patients with organic heart disease and chronic fixed atrial fibrillation. J Am Coll Cardiol. 1998;32:1040–1047. doi: 10.1016/s0735-1097(98)00358-1. [DOI] [PubMed] [Google Scholar]
- 12.Sandoval N, Velasco VM, Orjuela H, Caicedo V, Santos H, Rosas F, Carrea JR, Melgarejo I, Morillo CA. Concomitant mitral valve or atrial septal defect surgery and the modified cox-maze procedure. Am J Cardiol. 1996;77:591–596. doi: 10.1016/s0002-9149(97)89312-5. [DOI] [PubMed] [Google Scholar]
- 13.Gaynor SL, Diodato MD, Prasad SM, Ishii Y, Schuessler RB, Bailey MS, Damiano NR, Bloch JB, Moon MR, Damiano RJ., Jr. A prospective, single-center clinical trial of a modified cox maze procedure with bipolar radiofrequency ablation. J Thorac Cardiovasc Surg. 2004;128:535–542. doi: 10.1016/j.jtcvs.2004.02.044. [DOI] [PubMed] [Google Scholar]
- 14.Damiano RJ, Jr., Bailey M. The cox-maze IV procedure for lone atrial fibrillation. Multimed Man Cardiothorac Surg. 2007;2007 doi: 10.1510/mmcts.2007.002758. mmcts 2007 002758. [DOI] [PubMed] [Google Scholar]
- 15.Weimar T, Bailey MS, Watanabe Y, Marin D, Maniar HS, Schuessler RB, Damiano RJ., Jr. The cox-maze IV procedure for lone atrial fibrillation: A single center experience in 100 consecutive patients. J Interv Card Electrophysiol. 2011;31:47–54. doi: 10.1007/s10840-011-9547-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Lall SC, Melby SJ, Voeller RK, Zierer A, Bailey MS, Guthrie TJ, Moon MR, Moazami N, Lawton JS, Damiano RJ., Jr. The effect of ablation technology on surgical outcomes after the cox-maze procedure: A propensity analysis. J Thorac Cardiovasc Surg. 2007;133:389–396. doi: 10.1016/j.jtcvs.2006.10.009. [DOI] [PubMed] [Google Scholar]
- 17.Gelsomino S, Van Breugel HN, Pison L, Parise O, Crijns HJ, Wellens F, Maessen JG, La Meir M. Hybrid thoracoscopic and transvenous catheter ablation of atrial fibrillation. Eur J Cardiothorac Surg. 2014;45:401–407. doi: 10.1093/ejcts/ezt385. [DOI] [PubMed] [Google Scholar]
- 18.Bulava A, Mokracek A, Hanis J, Kurfirst V, Eisenberger M, Pesl L. Sequential hybrid procedure for persistent atrial fibrillation. J Am Heart Assoc. 2015 Mar 25;4(3) doi: 10.1161/JAHA.114.001754. [DOI] [PMC free article] [PubMed] [Google Scholar]