

Summary
Satisfaction of patients with their health care is gaining importance as a measure of hospital quality due to public reporting of these values and an increasing connection between hospital reimbursement and scores on the current tool to measure satisfaction, the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey. We found that high hospital and surgical volume and low rates of risk-adjusted mortality are associated with high patient satisfaction. However, other favorable patient outcomes are not consistently associated with positive satisfaction scores on HCAHPS. Contributors to patients' perceptions of their care are likely multifactorial and not related just to outcomes traditionally assessed by surgeons or hospitals. Moving in a direction of patient centered care, with a focus on increased understanding and involvement of patients in the care process, will likely strengthen the relationship between surgical outcomes and patient satisfaction.
Keywords: Patient satisfaction, HCAHPS, outcomes
Introduction
The Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey was developed by the Centers for Medicare & Medicaid Services (CMS) and the Agency for Healthcare Research and Quality (AHRQ). The HCAHPS survey is the first standardized survey of patient satisfaction and is designed to compare hospitals across the nation. The three main goals driving survey development were: 1) to motivate hospitals to improve their quality of care with regard to patient satisfaction, 2) to provide transparent public reporting of survey results, and 3) to allow consumers to objectively compare hospitals.1 The temporal sequence leading to the creation of the HCAHPS survey is outlined in Figure 1. Survey development began in 2002 with an extensive review of the literature, assessment of available survey tools, and cognitive testing.2 Over a 15-month period, the survey was piloted in three states: Maryland, Arizona, and New York. The National Quality Forum (NQF) endorsed the survey in May 2005 and the Office of Management and Budget approved the survey for national use in December of 2005.
Figure 1.
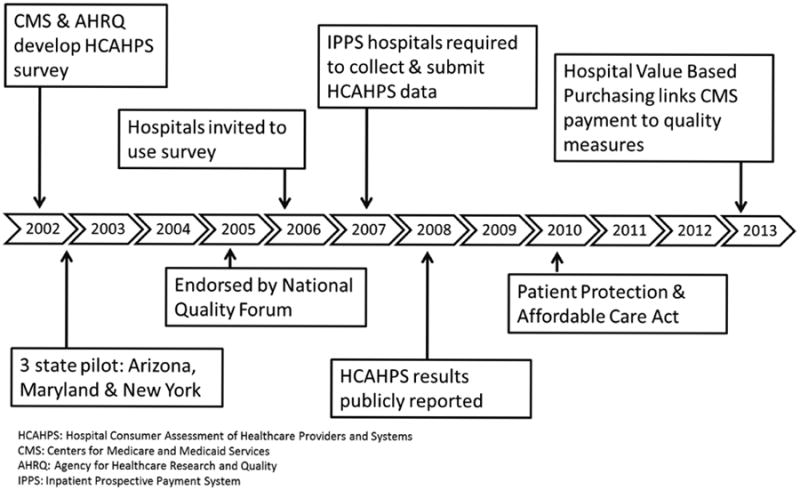
Sequence for the development and implementation of the HCAHPS survey.
(From Tevis ST, Schmocker RK, Kennedy GD. Can patients reliably identify safe, high quality care? Hosp Admin, 2014 (3) 5; 150-160.)
The HCAHPS survey consists of ten measures including six summary measures, two individual items, and two items evaluating overall patient satisfaction.1 There are a total of 32 questions, 25 which assess patients' perception of their care and 7 collect demographic information. Figure 2 demonstrates the HCAHPS questions pertaining to overall patient satisfaction.3 The survey is administered to medical, surgical, and maternity care patients within six weeks of hospital discharge. Hospitals may individually collect data or use approved vendors. Multiple attempts are made to connect with patients using any of four available survey modes: mail, telephone, mail with telephone follow-up, or active interactive voice recognition. Hospitals are required to collect at least 300 surveys annually for the Inpatient Prospective Payment System and surveys must be collected on a monthly basis.1 A case-mix adjustment using the following variables (self-reported health status, educational attainment, service line, age, admission from emergency department, interaction between service line and age, and primary language other than English) is applied to survey scores to allow for reliable comparisons across hospitals with differing patient populations.4-7 In addition, scores are adjusted based on mode of survey. Results of the case-mix adjusted HCAHPS survey scores are publicly reported four times each year on the Hospital Compare website.8 Scores are characterized as “top box” and “bottom box” percentiles for each HCAHPS domain. As demonstrated in Figure 2, top box scores represent the most favorable responses and bottom box scores are the least positive responses.1
Figure 2.
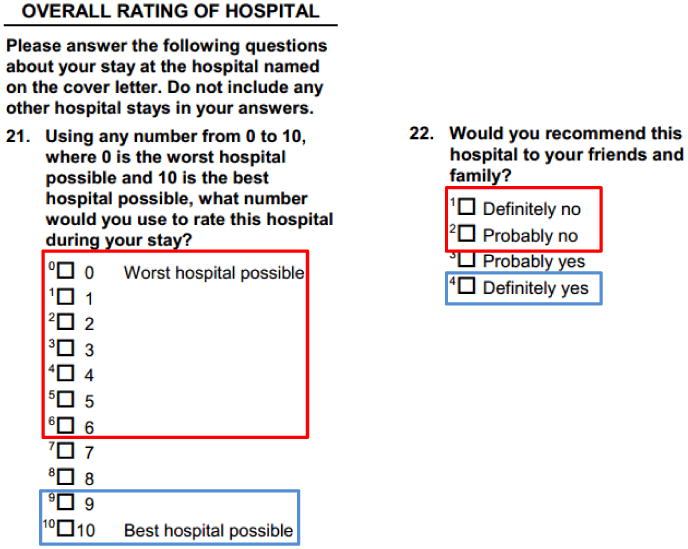
Overall Satisfaction HCAHPS domains. “Top box” responses are outlined in blue, while “bottom box” responses are outlined in red.
From www.hcahpsonline.org/files/HCAHPSV9.0AppendixA-MailSurveyMaterials(English)March2014.pdf.
National Impact of Satisfaction Surveys
The goals for the development of the HCAHPS survey were to motivate hospitals to improve the quality of care and to publicly provide information regarding patient satisfaction. Publicly reported HCAHPS scores are easily accessible to all consumers and are presented in a way that is simple to interpret. It is reasonable to assume that savvy consumers, if given the choice, will choose to have their care at hospitals with higher reported patient satisfaction scores. While narrow networks have limited access to some patients, when choice is possible patients tend to select providers and hospitals with higher ratings, including HCAHPS satisfaction scores.9,10 In addition, Medicare reimbursement has been linked to performance on the HCAHPS surveys. This began in 2005 when the Deficit Reduction Act mandated public reporting of HCAHPS scores in order for hospitals to receive full Medicare payment.1 The recent enactment of the Patient Protection and Affordable Care Act in 2010 includes HCAHPS measures in the Value Based Purchasing (VBP) program. The VBP program ties the hospital payments to clinical processes of care and patient experience. Top box HCAHPS scores are used to determine the patient experience domain of VBP, comparing hospitals to the national median and assessing the improvement of individual hospitals in each domain. HCAHPS scores encompass 30% of VBP performance (which by 2017 will account for 2% of overall Medicare reimbursement).1
Correlating Hospital Characteristics and Surgical Outcome Measures with Patient Satisfaction
With increasing pressure on hospitals and providers to improve performance on HCAHPS surveys, we thought it important within the surgical realm, to identify those variables that influence patient satisfaction. Surgeons for years have focused on outcomes such as mortality, rate of complication or specific assessments of surgical success (such as pain relief or bypass patency). Whether achievement of favorable surgical outcomes is at all correlative with satisfied patients is not clear. Currently there are few studies in the literature assessing predictors of patient satisfaction. To this end, we recently evaluated patient satisfaction as determined by HCAHPS and correlated this to hospital characteristics and as well as more traditional surgical outcomes derived from the University Health Systems Consortium (UHC) database. Our findings were surprising and provocative and overall suggest very little correlation between “traditional” surgical outcomes and patient satisfaction. The only factors that correlated with enhanced patient satisfaction were high hospital and surgical volume and low risk-adjusted mortality. Multiple other outcomes including rate of surgical complications, readmissions, process measures, etc., did not correlate. These relationships are demonstrated in figures 3 and 4 and are summarized in the paragraphs that follow.
Figure 3. Predictors of Overall Patient Satisfaction.

Figure 4. Non-predictors of Overall Patient Satisfaction.

Measures that Correlate with Patient Satisfaction
Hospital and Surgical Volume
Both hospital and surgical volume were found to significantly correlate with high overall patient satisfaction (p<0.001). Tsai and colleagues,11 recently identified a similar association between larger hospitals and the likelihood of recommending a hospital (p<0.001). Alternatively, in another study of medical and surgical patients, small hospitals were most likely to score in the top quartile for patient satisfaction12. The difference in these findings may be related to the HCAHPS domains used for the analysis. The study correlating patient satisfaction with small hospitals used a broader HCAHPS composite score for comparison (including factors such as a clean and quiet room and food service). Smaller hospitals may be more capable of achieving quiet, clean rooms and an attentive nursing staff whereas larger hospitals appear to score better on the summative HCAHPS domain “would you recommend this hospital to friends and family”. When using the summative HCAHPS measures as the sole outcome, there appears to be a clear relationship between large hospital size as well as high surgical volume and patient satisfaction.
Risk-Adjusted Mortality
We were particularly interested in determining if patient satisfaction correlated with hospital mortality. We found that patients at hospitals with low risk-adjusted mortality were significantly more likely on HCAHPS to recommend the hospital (Figure 3, p<0.001). Tsai et al.11 also found an association between low risk-adjusted mortality in surgical patients and high satisfaction scores on HCAHPS. However, Sheetz et al.13 in an evaluation of the Michigan Surgical Quality Collaborative registry did not find a significant difference in risk-adjusted mortality between hospitals with high versus low HCAHPS total performance scores (4% mortality in the lowest quintile vs. 3.3% mortality in the highest quintile). Elliott and colleagues,14 similarly showed no correlation between patient satisfaction and one year mortality. The difference in findings of the various studies may again be related to the variable domains used to measure patient satisfaction and the types of surgical patients evaluated.
Non-Predictors of Patient Satisfaction
Surprisingly, the remainder of the surgical outcomes that we evaluated had no correlation with overall patient satisfaction.
Clinical process measure compliance
Compliance with Surgical Care Improvement Project (SCIP) measures was not significantly associated with higher overall satisfaction (p=0.122, Figure 4). Lyu and colleagues15 also evaluated SCIP process measure compliance and consistent with our findings found no significant association between SCIP compliance and patient satisfaction. In contrast, several additional studies have demonstrated a positive relationship between compliance with SCIP and higher satisfaction scores.11,12,16,17 Thus, the relationship between SCIP compliance and patient satisfaction on HCAHPS is inconsistent. One of the possible reasons for this inconsistency is that over time hospitals have performed increasingly well on SCIP, with the majority achieving near 100% compliance. Therefore differences in SCIP compliance rates nationwide are small making any correlation between process measure compliance and patient satisfaction difficult to establish.
Post-operative Complications
Interestingly, we identified an unexpected trend of higher patient satisfaction in hospitals with higher rates of in hospital complications although this finding was not statistically significant (p = 0.49). Similarly Sheetz et al.13 showed no correlation between risk adjusted complication rates and satisfaction on the HCAHPS survey (25% morbidity in lowest quintile vs 25% morbidity in highest quintile). Gurland and colleagues also found that patients with postoperative complications had no diminution in the overall patient satisfaction ranking domains18. This is a surprising finding; one possible explanation is that surgical patients are forewarned and anticipate complications, and factor these into their overall care process.
Patient Safety Indicators
We also found numerically but not statistically, the greater the number of patient safety events the higher the patient satisfaction. In others studies, Patient Safety Indicators (PSIs) have had a mixed association with patient satisfaction. In an evaluation of hospitals in the National CAHPS Benchmarking Database, Isaac et al.17 found no correlation with overall patient satisfaction for most PSIs. PSIs are rare and as such are unlikely to affect overall patient satisfaction.
Length of Stay
We found no significant correlation between hospital length of stay (observed p = 0.819, risk adjusted p = 0.939) and patients' perceptions of their care. Our findings do conflict with a previous study where shorter risk adjusted length of hospital stay was associated with improved performance on the “recommendation of hospital” HCAHPS domain (7.1 days in high satisfaction group vs 7.7 days in low satisfaction group).11 The difference in findings may be related to differences in the surgical populations studied. We evaluated all patients discharged by general surgery, while Tsai et al.11 only evaluated patients undergoing the following 6 procedures: coronary artery bypass grafting, pulmonary lobectomy, endovascular aneurysm repair, open abdominal aortic aneurysm repair, colectomy, and hip replacement.
Post-operative Readmissions
Given the increasing emphasis on readmission reduction, we wished to evaluate whether readmission might produce a negative impact on patient satisfaction. While one might assume that hospitals with higher rates of readmission would have lower patient satisfaction, we actually found the opposite trend (p = 0.252). This contrasts with previous studies in medical patients, where investigators found low readmission rates to be associated with higher overall patient satisfaction. An evaluation of 30-day readmission rates in patients with myocardial infarction, congestive heart failure, and pneumonia revealed an association between higher overall satisfaction. Thus in chronic medical conditions readmission leads to diminished patient satisfaction but not the case, at least in our analysis, for surgical patients.
Correlation between patient outcomes and provider, hospital systems and environmental HCAHPS domains
We evaluated 8 HCAHPS domains that addressed provider services as well as hospital systems and environment and attempted to correlate these to patient outcomes. The relationship was essentially random (Table 1). The two HCAHPS domains that best correlated with patient outcomes were a clean room and pain control. These findings underscore the complexity of comparing multiple patient satisfaction domains to multiple quality outcome measures. The overall conclusion from our evaluation, however, is that there is essentially no meaningful correlation between traditional surgical outcomes and patient satisfaction.
Table 1. Correlation between Patient Satisfaction in the Provider, Hospital System, and Environmental Domains with Surgical Outcomes.
| Nursing Communication |
Physician Communication |
Received Help | Pain Controlled | Medications Explained |
Cleanliness of Room |
Quietness of Room |
Discharge Instructions |
|
|---|---|---|---|---|---|---|---|---|
| Hospital size | ||||||||
| Surgical volume | ||||||||
| SCIP compliance | 0.039 | 0.01 | 0.022 | |||||
| Complications | ||||||||
| PSIs | 0.018 | 0.03 | <0.001 | |||||
| LOS (observed) | 0.005 | 0.001 | ||||||
| LOS (risk adjusted) | 0.007 | 0.011 | <0.001 | 0.012 | ||||
| Readmission | 0.016 | |||||||
| Mortality (observed) | 0.002 | 0.012 | <0.001 | 0.005 | 0.002 | |||
| Mortality (risk adjusted) | 0.012 | 0.027 | 0.005 | 0.001 | 0.027 | <0.001 | 0.003 |
SCIP: Surgical Care Improvement Project
PSIs: Patient Safety Indicators
LOS: length of stay
P values denote significant relationships, while blanks represent lack of significance.
(Adapted from Kennedy GD, Tevis ST, Kent KC. Is there a relationship between patient satisfaction and favorable outcomes? Ann Surg. 2014 Oct;260(4):592-8; with permission.)
Additional Patient and Hospital Factors that Influence Patient Satisfaction
Proxy and Nonresponse Bias
The methods used to survey patients have been shown to affect patient satisfaction scores. Although survey scores are adjusted for mode of administration, other variables such as proxy response and assistance of a proxy in preparing the response have been found to influence satisfaction scores.19 Twenty percent of HCAHPS surveys are completed by or with the assistance of a proxy. While life partners or spouses usually respond in a manner similar to patients, other family members and non-family members often provide a less favorable response. Non-responders have also been evaluated and are more likely to be racial minorities, patients leaving against medical advice, or obstetric or medical patients (versus surgical patients).20-22
Healthcare Utilization
With increasing pressure to provide high quality and efficient care, studies have assessed healthcare utilization and patient satisfaction. Patients who are less likely to utilize the emergency department are more satisfied 23. Alternatively, there is a positive relationship between satisfied patients and those more likely to accrue higher total health expenditures.
Hospital Characteristics
Various hospital factors have been identified as predictors of patient satisfaction, including staffing, teaching status, and use of health information technology. Higher nurse to patient ratios are more likely to produce higher overall satisfaction (66% top box scores in high nurse to patient day ratio hospitals vs 61% in low nurse to patient day ratio hospitals).11,16 Mixed results have been reported regarding the relationship between hospital teaching status and patient satisfaction on HCAHPS with some studies reporting no difference16 while others found teaching hospitals were associated with higher satisfaction scores.11,12 With healthcare evolving to greater use of the electronic medical record (EMR), little is known about the effect of the EMR on patient satisfaction. One study assessed the relationship between health information technology (HIT) and patient satisfaction scores in groups of patients seeing specialists and primary care providers.24 Four factors were found to be highly associated with favorable scores on the physician communication domain: ability to have questions answered in a timely manner through email, ability to an make appointments by email, physician use of a computer, and a provider website.
The Value of Feedback in Improving Patient Satisfaction Scores
A study by Elliott and colleagues,25 demonstrated statistically significant improvement in patient satisfaction scores (8 out of 9 satisfaction domains) in the first year after survey results were publicly reported. It appears that hospitals have embraced these surveys as well as their findings and are identifying ways to change culture and improve systems to enhance patient satisfaction. Many quality improvement projects have been implemented in an effort to improve patient satisfaction scores. Projects have focused on pain management, communication, or provider incentives, however the modest success of these individual initiatives suggests that tackling patient satisfaction is a complex undertaking.
Pain Management
A study of the rating of the pain intensity for surgical, trauma, and oncology patients revealed no association between pain and satisfaction scores.26 While these authors did identify a trend between higher pain scores and decreased satisfaction, this difference did not reach statistical significance.
Communication Training
Given the increasing emphasis on improving HCAHPS scores, improving provider communication has become an area of interest. One group implemented a communication skills training program on a nonteaching hospitalist service. The program consisted of three 90-minute sessions and provided education about patient satisfaction and communication skills, a simulation based communication exercise, and coaching sessions during clinical encounters. Only 40% of physicians completed all three training sessions and following training there were no significant differences in overall or physician communication satisfaction scores. The findings were similar when a relationship based care (RBC) model was implemented for nursing at a single institution.27 RBC models focused on collaboration and patient centered care. Average nursing satisfaction scores were unchanged (91% vs 91%) following the implementation of this model. Thus, efforts to enhance physician and staff communication have not yet yielded positive results.
Provider Incentives
The effect of monetary incentives to enhance patient satisfaction has been investigated. It would seem that incentivizing providers with monetary rewards might have a positive effect on their efforts toward patient satisfaction. In one study, emergency department residents could earn discount cards for espressos or a monetary bonus as patient satisfaction scores increased (i.e. $50 for the 50th percentile and $200 for the 80th percentile). Unfortunately, these monetary incentives had no overall effect on resident performance in the realm of patient satisfaction.
Patient and Team Communication
Several studies have demonstrated success in improving patient satisfaction by addressing communication and rewarding compassion. In one study physicians with high communication scores were interviewed to determine what common practices they employed when providing patient care.28 Participating physicians stressed the importance of hiring staff with excellent people skills and involving office staff in patient visits. High scoring physicians also valued the use of non-verbal communication, providing clear explanations for patients, asking patients personal questions and recalling the information later, and developing an agreed upon plan at the end of each interaction. In depth interviews with thirty patients on a hospitalist service revealed additional insight with regard to patient satisfaction. Areas that were emphasized by these patients were physician behavior, team communication, and systems issues.29 Patients valued interactions where physicians displayed a caring attitude and allowed patients to participate in medical decision-making. Satisfaction with specialists was based on perceived competence and continuity of care. Major themes of dissatisfied patients included the perception that physicians were not communicating with each other, or lacked understanding of the responsibility of each of the individual members of the team. Any disorganized care, inclusive of food services or housekeeping, produced a decrement in physician HCAHPS scores.
Devotion of Additional Hospital Resources
Bastani et al.30 were able to improve patient satisfaction in the emergency department by utilizing a scribe in the setting of an electronic medical record to improve efficiency of care and physician communication. The authors found an improvement in overall emergency department satisfaction (58% to 75%) and physician satisfaction (62% to 92%) after implementation of a scribe program. Similarly, the addition of a Physician Partner, who acted as a scribe and performed administrative duties in a medical clinic led patients to report high satisfaction by increasing the amount physician contact.31 Guss and colleagues32 implemented a telephone call to patients after discharge from the emergency department in an effort to improve patient satisfaction. Patients who received a post-discharge phone call were more likely to recommend the hospital compared with those who did not receive a phone call (89% vs 56%). Of note the cost associated with these interventions can be substantial and may limit broad implementation. These successes aside, programs aimed at changing only one aspect of patient care have had variable results in improving patient satisfaction scores. It has become clear that increased patient satisfaction requires simultaneously changing multiple variables or a significant cultural change.
Surgeons as Leaders in Patient Satisfaction
To consistently provide high quality patient centered care, a patient centered multi-disciplinary team approach is required. This team should include physicians, nurses, residents, pharmacists, students, patients and families. Expansion of the “health care team” to include staff from other areas including environmental services, information technology, food service, facilities, and administrative personnel is essential. Given the dominant role that surgeons play in the care of their patients, it is incumbent on surgeons to take the lead in organizing and supporting this caregiver team. High patient satisfaction correlates with effective communication, personalization of care, patient education, and continuity of care. Surgeons are uniquely positioned to lead this complex multi-disciplinary team to provide patient centered care that will result in highly satisfied patients. A previous study by Banki et al.33 demonstrated improved patient satisfaction scores after the development of a multi-disciplinary surgeon led team. This improvement project consisted of staff education and standardization of care in patients who underwent laparoscopic fundoplication and Heller myotomy. The surgeon led team participated in monthly teaching sessions and multi-disciplinary conferences; team leaders attended weekly meetings; and the surgeon led daily multi-disciplinary bedside rounds. An emphasis was also placed on weekly review of issues, concerns, and processes that required improvement. Patients reported higher satisfaction in the following domains after implementation of the surgical team: overall rating, communication with nurses, communication about medications, and discharge instructions. In addition, after the implementation of a surgeon led team, operative times, length of stay, and costs all significantly decreased. An organizational change to a team based, mindful, approach to patient care will result in patients who are highly satisfied with their surgical outcomes and hospital experience.
Summary
Patients' perceptions have become an important measure of hospital care. Patient satisfaction scores are now available publicly and are tied to Medicare reimbursement incentivizing hospitals to improve patients' perceptions of their care. While higher hospital and surgical volumes and low risk adjusted mortality have been found to translate into increased patient satisfaction on HCAHPS, many other variables are likely in play. A collaborative team based approach is needed to continuously improve the quality of care and to improve patients' perceptions of their care. Surgeons are uniquely poised to lead organizational change aimed at providing exceptional team based patient service.
Key Points.
Patient satisfaction continues to gain importance in healthcare with public reporting of scores along with ties between satisfaction scores and Medicare reimbursement.
High hospital and surgical volume and low risk-adjusted mortality rates are associated with high overall patient satisfaction.
More traditional measures of outcome as well as markers of hospital quality and safety are not consistently associated with high patient satisfaction.
The focus on patient satisfaction is here to stay; a multi-disciplinary, surgeon led effort dedicated to improving patient's perceptions of their care is essential.
Acknowledgments
Support for this study was provided by the NIH T32 training grant (CA090217).
Footnotes
The authors have no conflicts of interest to declare.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.HCAHPS Fact Sheet. http://www.hcahpsonline.org/files/August%202013%20HCAHPS%20Fact%20Sheet2.pdf.
- 2.Goldstein E, Farquhar M, Crofton C, Darby C, Garfinkel S. Measuring hospital care from the patients' perspective: an overview of the CAHPS Hospital Survey development process. Health Serv Res. 2005 Dec;40(6 Pt 2):1977–1995. doi: 10.1111/j.1475-6773.2005.00477.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.HCAHPS Survey.
- 4.Morales LS, Elliott MN, Weech-Maldonado R, Spritzer KL, Hays RD. Differences in CAHPS adult survey reports and ratings by race and ethnicity: an analysis of the National CAHPS benchmarking data 1.0. Health Serv Res. 2001 Jul;36(3):595–617. [PMC free article] [PubMed] [Google Scholar]
- 5.Elliott MN, Swartz R, Adams J, Spritzer KL, Hays RD. Case-mix adjustment of the National CAHPS benchmarking data 1.0: a violation of model assumptions? Health Serv Res. 2001 Jul;36(3):555–573. [PMC free article] [PubMed] [Google Scholar]
- 6.Elliott MN, Zaslavsky AM, Goldstein E, et al. Effects of survey mode, patient mix, and nonresponse on CAHPS hospital survey scores. Health Serv Res. 2009 Apr;44(2 Pt 1):501–518. doi: 10.1111/j.1475-6773.2008.00914.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Weech-Maldonado R, Morales LS, Elliott M, Spritzer K, Marshall G, Hays RD. Race/ethnicity, language, and patients' assessments of care in Medicaid managed care. Health Serv Res. 2003 Jun;38(3):789–808. doi: 10.1111/1475-6773.00147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hospital Compare. www.medicare.gov/hospitalcompare/search.html.
- 9.Faber M, Bosch M, Wollersheim H, Leatherman S, Grol R. Public reporting in health care: how do consumers use quality-of-care information? A systematic review. Med Care. 2009 Jan;47(1):1–8. doi: 10.1097/MLR.0b013e3181808bb5. [DOI] [PubMed] [Google Scholar]
- 10.Kolstad JT, Chernew ME. Quality and consumer decision making in the market for health insurance and health care services. Med Care Res Rev. 2009 Feb;66(1 Suppl):28S–52S. doi: 10.1177/1077558708325887. [DOI] [PubMed] [Google Scholar]
- 11.Tsai TC, Orav EJ, Jha AK. Patient Satisfaction and Quality of Surgical Care in US Hospitals. Ann Surg. 2014 May 30; doi: 10.1097/SLA.0000000000000765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lehrman WG, Elliott MN, Goldstein E, Beckett MK, Klein DJ, Giordano LA. Characteristics of hospitals demonstrating superior performance in patient experience and clinical process measures of care. Med Care Res Rev. 2010 Feb;67(1):38–55. doi: 10.1177/1077558709341323. [DOI] [PubMed] [Google Scholar]
- 13.Sheetz KH, Waits SA, Girotti ME, Campbell DA, Jr, Englesbe MJ. Patients' Perspectives of Care and Surgical Outcomes in Michigan: An Analysis Using the CAHPS Hospital Survey. Ann Surg. 2014 Jul;260(1):5–9. doi: 10.1097/SLA.0000000000000626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Elliott MN, Haviland AM, Cleary PD, et al. Care experiences of managed care Medicare enrollees near the end of life. J Am Geriatr Soc. 2013 Mar;61(3):407–412. doi: 10.1111/jgs.12121. [DOI] [PubMed] [Google Scholar]
- 15.Lyu H, Wick EC, Housman M, Freischlag JA, Makary MA. Patient satisfaction as a possible indicator of quality surgical care. JAMA Surg. 2013 Apr;148(4):362–367. doi: 10.1001/2013.jamasurg.270. [DOI] [PubMed] [Google Scholar]
- 16.Jha AK, Orav EJ, Zheng J, Epstein AM. Patients' perception of hospital care in the United States. N Engl J Med. 2008 Oct 30;359(18):1921–1931. doi: 10.1056/NEJMsa0804116. [DOI] [PubMed] [Google Scholar]
- 17.Isaac T, Zaslavsky AM, Cleary PD, Landon BE. The relationship between patients' perception of care and measures of hospital quality and safety. Health Serv Res. 2010 Aug;45(4):1024–1040. doi: 10.1111/j.1475-6773.2010.01122.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Gurland BH, Merlino J, Sobol T, et al. Surgical complications impact patient perception of hospital care. J Am Coll Surg. 2013 Nov;217(5):843–849. doi: 10.1016/j.jamcollsurg.2013.06.015. [DOI] [PubMed] [Google Scholar]
- 19.Elliott MN, Beckett MK, Chong K, Hambarsoomians K, Hays RD. How do proxy responses and proxy-assisted responses differ from what Medicare beneficiaries might have reported about their health care? Health Serv Res. 2008 Jun;43(3):833–848. doi: 10.1111/j.1475-6773.2007.00820.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Elliott MN, Edwards C, Angeles J, Hambarsoomians K, Hays RD. Patterns of unit and item nonresponse in the CAHPS Hospital Survey. Health Serv Res. 2005 Dec;40(6 Pt 2):2096–2119. doi: 10.1111/j.1475-6773.2005.00476.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Klein DJ, Elliott MN, Haviland AM, et al. Understanding nonresponse to the 2007 Medicare CAHPS survey. Gerontologist. 2011 Dec;51(6):843–855. doi: 10.1093/geront/gnr046. [DOI] [PubMed] [Google Scholar]
- 22.Zaslavsky AM, Zaborski LB, Cleary PD. Factors affecting response rates to the Consumer Assessment of Health Plans Study survey. Med Care. 2002 Jun;40(6):485–499. doi: 10.1097/00005650-200206000-00006. [DOI] [PubMed] [Google Scholar]
- 23.Fenton JJ, Jerant AF, Bertakis KD, Franks P. The cost of satisfaction: a national study of patient satisfaction, health care utilization, expenditures, and mortality. Arch Intern Med. 2012 Mar 12;172(5):405–411. doi: 10.1001/archinternmed.2011.1662. [DOI] [PubMed] [Google Scholar]
- 24.McInnes DK, Brown JA, Hays RD, et al. Development and evaluation of CAHPS questions to assess the impact of health information technology on patient experiences with ambulatory care. Med Care. 2012 Nov;50(Suppl 1):S11–19. doi: 10.1097/MLR.0b013e3182610a50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Elliott MN, Lehrman WG, Goldstein EH, et al. Hospital survey shows improvements in patient experience. Health Aff (Millwood) 2010 Nov;29(11):2061–2067. doi: 10.1377/hlthaff.2009.0876. [DOI] [PubMed] [Google Scholar]
- 26.Phillips S, Gift M, Gelot S, Duong M, Tapp H. Assessing the relationship between the level of pain control and patient satisfaction. J Pain Res. 2013;6:683–689. doi: 10.2147/JPR.S42262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Cropley S. The relationship-based care model: evaluation of the impact on patient satisfaction, length of stay, and readmission rates. J Nurs Adm. 2012 Jun;42(6):333–339. doi: 10.1097/NNA.0b013e31825738ed. [DOI] [PubMed] [Google Scholar]
- 28.Quigley DD, Martino SC, Brown JA, Hays RD. Evaluating the content of the communication items in the CAHPS((R)) clinician and group survey and supplemental items with what high-performing physicians say they do. Patient. 2013;6(3):169–177. doi: 10.1007/s40271-013-0016-1. [DOI] [PubMed] [Google Scholar]
- 29.Wild DM, Kwon N, Dutta S, et al. Who's behind an HCAHPS score? Jt Comm J Qual Patient Saf. 2011 Oct;37(10):461–468. doi: 10.1016/s1553-7250(11)37059-6. [DOI] [PubMed] [Google Scholar]
- 30.Bastani A, Shaqiri B, Palomba K, Bananno D, Anderson W. An ED scribe program is able to improve throughput time and patient satisfaction. Am J Emerg Med. 2013 May;32(5):399–402. doi: 10.1016/j.ajem.2013.03.040. [DOI] [PubMed] [Google Scholar]
- 31.Reuben DB, Knudsen J, Senelick W, Glazier E, Koretz BK. The Effect of a Physician Partner Program on Physician Efficiency and Patient Satisfaction. JAMA Intern Med. 2014 May 12; doi: 10.1001/jamainternmed.2014.1315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Guss DA, Gray S, Castillo EM. The impact of patient telephone call after discharge on likelihood to recommend in an academic emergency department. J Emerg Med. 2013 Apr;46(4):560–566. doi: 10.1016/j.jemermed.2013.11.067. [DOI] [PubMed] [Google Scholar]
- 33.Banki F, Ochoa K, Carrillo ME, et al. A surgical team with focus on staff education in a community hospital improves outcomes, costs and patient satisfaction. Am J Surg. 2013 Dec;206(6):1007–1014. doi: 10.1016/j.amjsurg.2013.08.015. discussion 1014-1005. [DOI] [PubMed] [Google Scholar]