

Abstract
Patients with an accessory kidney are characterized by an excessive number of kidneys. The ureter of the accessory kidney either drains separately into the bladder or merges with the ureter of the main kidney. In our case, interestingly, the ureter of the left main kidney drained directly into the accessory kidney and the ureter of the latter was the common drainage route for both. The drainage of a normal kidney via the ureter of an accessory kidney has not been reported in the literature, so far. The aim of this report is to present the case with radiological findings and to emphasize the effects of this situation on planned surgical procedures. A 62-year-old female patient had an interesting abnormality on the left collecting system, which was revealed on excretory urography (EU), retrograde urography (RU) and multidetector computed tomography (MDCT). A kinky left ureter, which formed a U shape, was revealed on EU. On MDCT, an accessory kidney was revealed at the anterior aspect of the middle zone of left main kidney. The ureter of the main left kidney drained directly into the accessory kidney. The course of this drainage was confirmed by retrograde urography. An accessory kidney is a rare entity associated with horseshoe kidney, ectopic ureter draining into the vagina, bifid collecting system and coarctation of the aorta. In our case, an unusual association between the ureters of the main and accessory kidneys was revealed, which may have an impact on planned surgery in the groin and retroperitoneal areas.
Keywords: Accessory kidney, excretory urography, multidetector computerized tomography, retrograde urography
Introduction
Accessory kidney is a rare anomaly of the urinary tract that is characterized by an excessive number of kidneys. It is a parenchymatous structure, which may be completely separated from the ipsilateral normal kidney, or may have loose adhesion with it.[1] Most commonly, an accessory kidney is situated on the left, caudal to the main kidney. Although variable in its dimensions, the accessory kidney tends to be smaller than the main kidney but is often still functional.[2,3] Its incidence is similar in males and females. The ureter of the accessory kidney may reveal positional variations. It may drain directly into the bladder, usually cranial to the ureter of the main kidney, or may merge with the ureter of the main kidney to drain as a single ureter.[3] In our case, an interesting variation was revealed, as the ureter of the left main kidney drained into the accessory kidney. The ureter of the accessory kidney was the sole drainage route for both kidneys. This type of association, which may have an impact on any type of surgery performed in the retroperitoneal area, has not been previously reported in the literature.
Case presentation
A 62-year-old female patient was admitted to the hospital with right groin pain lasting for 3 months. The pain was dull, not reflecting and was not accompanied by any other symptoms. Her medical history was unremarkable, her physical examination and laboratory findings were within normal limits. She had had ultrasound (US) and computed tomography (CT) examinations in another clinic, which were determined to be within normal ranges. A 6 mm radiopacity at the distal part of the left ureter was revealed by direct urinary system imaging. An excretory urography (EU) obtained in our clinic revealed a dilated (1.2 cm maximally) pelvis and delayed function of the left kidney. The ureter of the left kidney was tortuous; specifically, at approximately 5 cm from the ureteropelvic junction. It coursed to the left and then superiorly, forming a U shape. The anatomy and function of the right kidney were unremarkable (Figures 1a, b).
Figure 1.
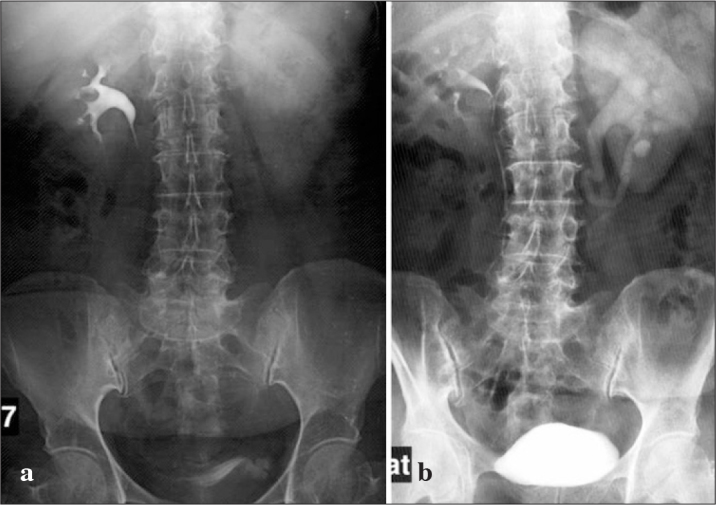
EU: Delayed function of the left kidney (a), Dilated left renal collecting system and the unusual course of the left ureter (b).
Anatomical abnormalities of the left kidney were further investigated by 64-row multidetector computed tomography (MDCT). A cystic lesion of 3.5×2.5 cm adjacent to the anterior middle zone of the left kidney was determined to be an accessory kidney. The ureter of this kidney was also dilated (max. 1 cm). The ureter of the main kidney curled behind the ureter of the accessory kidney and drained directly into the pelvis of that kidney (Figures 2a, b). A retrograde urography was conducted to evaluate the radiopacity at the lower one-third of the ureter and to confirm the data obtained from MDCT. The contrast medium filled the ureter, the accessory kidney and the main kidney, emphasizing that the draining ureter belonged to the accessory kidney (Figure 3). A distal ureteral stone was removed endoscopically. Informed consents were obtained prior to the relevant radiologic interventions.
Figure 2.

Axial MDCT: A cystic accessory kidney adjacent to the anterior aspect of the left kidney (a), Coronal MDCT: The ureter of the main kidney curled behind the ureter of the accessory kidney and drained directly into the pelvis of that kidney. The ureter of the accessory kidney drained into the gall bladder (b).
Figure 3.

Retrograde urography: The contrast medium filled the ureter, the accessory kidney and the main kidney. Note that the draining ureter belonged to the accessory kidney.
Discussion
An accessory kidney is defined as the presence of a third kidney with an independent parenchyma and collecting system. The collecting system of the accessory kidney may drain directly into the bladder, or rarely, to the vagina, or may coalesce with the ureter of the main kidney.[4] Even though it is a congenital abnormality, patients may remain asymptomatic until adolescence.[1] The average age at diagnosis is 36 years, and because 1/3 of the cases remain asymptomatic, they are often diagnosed incidentally.[4] The usual symptoms include fever, pain and a palpable abdominal mass.[1,2,5,6] Hydronephrosis, stones, pyonephrosis, pyelonephritis and malignant changes may accompany the accessory kidney. The most common indications for medical and/or surgical interventions include urinary tract infection and obstruction.[1,5] It can also be associated with congenital anomalies, such as the coarctation of aorta, horseshoe kidney, double collecting system, vaginal atresia and ectopic ureter.[4,7,8] In this case, the patient was admitted with complaints of pain, ureteral stones and hydronephrosis. No accompanying abnormalities were detected.
Although no proven mechanisms exist for the embryological development of the accessory kidney, a number of hypotheses have been proposed. The parenchyma of the accessory kidney may develop as an outcome of the division of either one nephrogenic blastema or two separately blooming nephrogenic blastema. The ureters to these embryonic organs stem from the Wolffian duct and develop by a premature division of either a single ureteric bud or two separately developed buds, resulting in partial or complete duplication anomalies.[1–4]
Accessory kidneys can be diagnosed by EU, US, retrograde urography, nuclear imaging, CT and MRI scans.[2,5,6] The diagnosis may be complicated by the smaller size or reduced function of the accessory kidney and its superimposition on the normal kidney. In our case, three-dimensional imaging was necessary to accurately establish the diagnosis, because of the unusual course of the left ureter and the unique drainage of the left main kidney into the accessory kidney. Confirmation by RU was helpful in evaluating the communications between ureters and kidneys, although the main reason to perform a RU was to diagnose urinary obstruction caused by a stone disease.
The main approach to treat an accessory kidney depends on its function and associated symptoms. Asymptomatic kidneys do not need any treatment, but regular monitoring is recommended to detect any complication. The standard treatment for an accessory kidney is simple nephrectomy if the patient is symptomatic or has complications, or the kidney has a negligible function.[2,4,6] In our case, nephrectomy was contraindicated because the drainage of the main kidney was supported by the accessory kidney. Surgeons must be aware of this variety of developmental anomaly before conducting irreversible surgery, and this awareness depends on reliable imaging.
Footnotes
Informed Consent: Written informed consent was obtained from patient who participated in this case.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept - G.E.; Design - G.E., M.U.; Supervision - G.E., M.U.; Funding - G.E., M.U., S.D.; Materials - G.E., M.U.; Data Collection and/or Processing - G.E., M.U.; Analysis and/ or Interpretation - G.E., M.U., S.D.; Literature Review - G.E., M.D., S.D.; Writer - G.E., M.U., S.D.; Critical Review - G.E., M.U.; Other -G.E., M.U., S.D.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study has received no financial support.
References
- 1.Tada Y, Kokado Y, Hashinaka Y, Kadowaki T, Takasugi Y, Shin T, et al. Free supernumerary kidney: a case report ands review. J Urol. 1981;126:231–2. doi: 10.1016/s0022-5347(17)54457-2. [DOI] [PubMed] [Google Scholar]
- 2.Flyer MA, Haller JO, Feld M, Kantor A. Ectopic supernumerary kidney : another cause of a pelvic mass. Abdom Imaging. 1994;19:374–5. doi: 10.1007/BF00198203. [DOI] [PubMed] [Google Scholar]
- 3.N’Guessan G, Stephens FD. Supernumerary kidney. J Urol. 1983;130:649–53. doi: 10.1016/s0022-5347(17)51385-3. [DOI] [PubMed] [Google Scholar]
- 4.Koureas AP, Panourgias EC, Gouliamos AD, Trakadas SJ, Vlahos LJ. Imaging of a supernumerary kidney. Eur Radiol. 2000;10:1722–3. doi: 10.1007/s003300000439. [DOI] [PubMed] [Google Scholar]
- 5.Oto A, Kerimoglu U, Eskicorapci S, Hazirolan T, Tekgül S. Bilateral supernumerary kidney: imaging findings. JBR-BTR. 2002;85:300–3. [PubMed] [Google Scholar]
- 6.Sudhakar Krishnan MM, Jeya RK, Jayalakshmi P. Supernumerary kidney- a case report and review. Singapore Med J. 1986;27:74–6. [PubMed] [Google Scholar]
- 7.Unal M, Erem C, Serce K, Tuncer C, Bostan M, Gökce M. The presence of both horseshoe and a supernumerary kidney associated with coarctation of aorta. Acta Cardiol. 1995;50:155–60. [PubMed] [Google Scholar]
- 8.Sahinkanat T, Okur N. Supernumerary kidney associated with horseshoe kidney: An unusual presentation. Turkish Journal of Urology. 2007;33:372–4. [Google Scholar]