

Abstract
The accumulation of ureteric stone fragments causing ureteric blockage is known as ‘Steinstrasse’ or ‘Stone Street’ and is usually described as a complication of shock-wave lithotripsy (SWL). We herein present a rare case of massive Steinstrasse in a young male patient with no previous history of urolithiasis or lithotripsy.
Keywords: Shock wave lithotripsy (SWL), steinstrasse, ureteric calculi
Introduction
Steinstrasse, the accumulation of ureteric stone fragments causing a ureteric blockage, mostly occurs after treatment for renal stones (by surgery or shock wave lithotripsy - SWL) and is often transient and asymptomatic. In up to one-third of cases, Steinstrasse may present as a silent obstruction, with the resultant loss of renal function.[1] Depending on the presenting complaint, the treatment of Steinstrasse can include observation, medical expulsion therapy, SWL, nephrostomy insertion and/or ureteroscopy.
Using a plain abdominal radiograph, computed tomography (CT) scan and endoscopic operative images of the urinary tract, we describe the management course of an unusual massive load of ureteric calculi in a lithotripsy-free young male patient.
Case presentation
We present a 34-year-old male with a history of Friedreich’s ataxia who attended our clinic complaining of left renal colic and dysuria. His routine physical examination was unremarkable, but the urine culture confirmed an E. coli-positive urinary tract infection (UTI). A plain abdominal radiography (Fig. 1) and CT scan (Fig. 2) of the urinary tract revealed several calculi in the left kidney, left hydronephrosis and a remarkable aggregation of multiple calculi in the left ureter.
Figure 1.

Plain radiograph of the urinary tract demonstrating several rounded opacities in the left kidney consistent with calculi and an aggregation in the left side of the pelvis that is most likely to be within the ureter (ureteric calculi).
Figure 2.
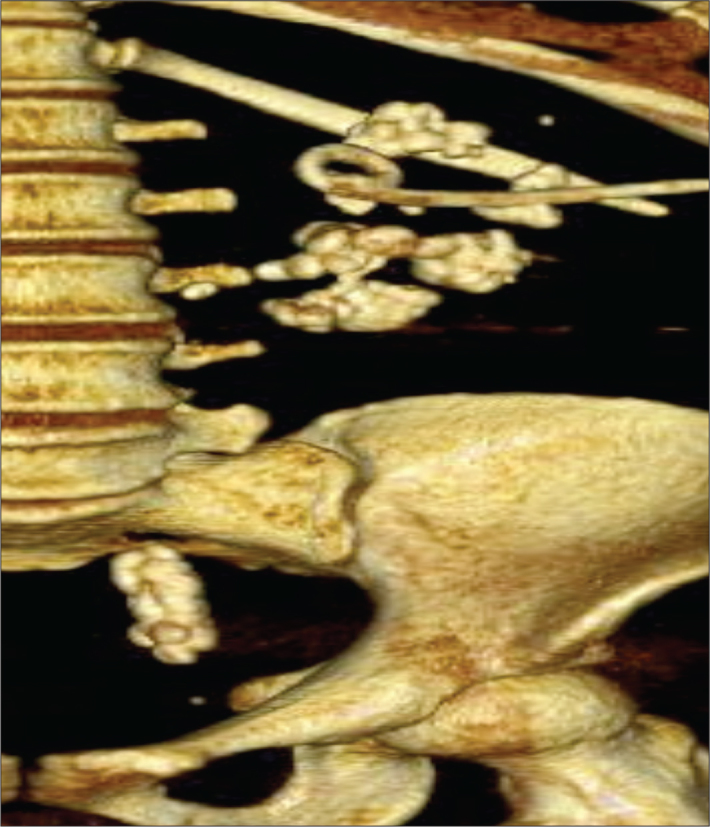
Sagittal view of the 3-D reconstruction CT scan illustrating multiple large calculi in the left kidney, with the largest (on the right) measuring 2 cm. The calculus is similar to a staghorn, and there are numerous stones in the lower left ureter, which is distended. Additionally, the left nephrostomy tube is visible in situ.
After treating the urinary tract infection with intravenous antibiotics and inserting a left nephrostomy tube under ultrasound guidance, a left semi-rigid ureteroscopy for ureteric calculi and percutaneous nephrolithotomy for the renal stones were performed simultaneously (Fig. 3). A pneumatic lithotripter was used to disintegrate and remove the stones. A left double-pigtail ureteric stent (22 cm, 6 Fr) was left in situ at the end of the operation.
Figure 3.

Endoscopic image of multiple ureteric stones in the left renal pelvis after being flushed into the kidney to be removed using a nephroscope.
The urethral catheter and left nephrostomy tube were removed on the third postoperative day (POD), and the patient had an uneventful discharge on the fifth POD. Two months later, his unremarkable outpatient follow-up was followed by the removal of the left ureteric stent using a flexible cystoscope. The subsequent plain abdominal radiograph showed satisfactory results (Fig. 4), and the stone analysis revealed 100% carbonate apatite.
Figure 4.

Plain radiograph of the urinary tract showing significant clearance of both the left renal and ureteric stones
Discussion
Steinstrasse is a known complication of the treatment of large renal calculi and is reported in 2 to 10 per cent of SWL cases.[1, 2]
A major problem of steinstrasse is silent ureteric obstruction, which can occur in 23 per cent of cases and lead to the loss of kidney function.[1, 3] Anuria can also be observed in 5 per cent of steinstrasse cases in solitary kidney patients.[1] In the present case, there was no history of urolithiasis or SWL, and ureteric obstruction and UTI were the presenting complaints.
Conservative treatment is the first line of option if the patient is asymptomatic and willing to remain under close surveillance. Another treatment option is medical expulsion therapy, which increases the stone pass rate and reduces the need for an operative intervention.[4]
The choice of intervention includes SWL, the placement of a percutaneous nephrostomy and endoscopic stone retrieval. SWL is indicated when large stone fragments are present with no evidence of UTI and there is a high chance (at least 80 per cent) of clearing the Steinstrasse.[4, 5] Ureteroscopy is equally as effective as SWL for the treatment of Steinstrasse.[6] The insertion of a percutaneous nephrostomy is also an option in cases of symptomatic ureteric obstruction with or without a UTI.[5] In our patient, conservative treatment and SWL were excluded due to the presence of a UTI and pain secondary to the ureteric obstruction.
In conclusion, we present a case with primary non-SWL-related massive Steinstrasse. To the best of our knowledge, no similar case has been reported to date.
Footnotes
Conflict of interest statement
All authors hereby state that they have no conflicting financial or personal relationships that could inappropriately influence (bias) this work.
Consent
Informed consent was obtained from the patient for the publication of this report and the accompanying images.
References
- 1.Madbouly K, Sheir KZ, Elsobky E, Eraky I, Kenawy M. Risk factor for the formation of a steinstrasse after extracorporeal shock wave lithotripsy: A statistical model. J Urol. 2002;167:1239–42. [PubMed] [Google Scholar]
- 2.Sulaiman MN, Buchholz NP, Clark PB. The role of ureteral stent placement in the prevention of Steinstrasse. J Endourol. 1999;13:151–5. doi: 10.1089/end.1999.13.151. [DOI] [PubMed] [Google Scholar]
- 3.Hardy MR, McLeod DG. Silent renal obstruction with severe functional loss after extracorporeal shock wave lithotripsy: a report of 2 cases. J Urol. 1987;137:91–2. doi: 10.1016/s0022-5347(17)43882-1. [DOI] [PubMed] [Google Scholar]
- 4.Moursy E, Gamal WM, Abuzeid A. Tamsulosin as an expulsive therapy for steinstrasse after extracorporeal shock wave lithotripsy: a randomized controlled study. Scand J Urol Nephrol. 2010;44:315–9. doi: 10.3109/00365599.2010.494616. [DOI] [PubMed] [Google Scholar]
- 5.Sayed MA, el-Taher AM, Aboul-Ella HA, Shaker SE. Steinstrasse after extracorporeal shockwave lithotripsy: aetiology, prevention and management. BJU Int. 2001;88:675–8. doi: 10.1046/j.1464-4096.2001.02435.x. [DOI] [PubMed] [Google Scholar]
- 6.Rabbani SM. Treatment of steinstrasse by transureteral lithotripsy. Urol J. 2008;5:89–93. [PubMed] [Google Scholar]