

Abstract
Page kidney is defined as the external compression of the kidney, typically by a subcapsular hematoma, that leads to hypertension due to hypoperfusion and ischemia. The treatment options include medical anti-hypertensive treatment, percutaneous drainage, surgical decortication and nephrectomy. Laparoscopic decortication of Page kidney is a newly defined minimally invasive management technique. We describe 2 cases of Page kidney that failed to improve with percutaneous drainage but were successfully treated with the laparoscopic approach.
Keywords: Hypertension, laparoscopic treatment, Page kidney
Introduction
Page kidney is defined as the external compression of the kidney, typically by a subcapsular hematoma, that leads to hypertension due to activation of the renin-angiotensinaldosterone (RAA) axis by hypoperfusion and microvascular ischemia of the kidney.[1,2] Tumor, lymphocele, and urinoma are other known causes.[3] The spontaneous formation of a renal subcapsular hematoma has been reported.[4] Management options include medical anti-hypertensive treatment, percutaneous drainage, surgical decortication and nephrectomy.[5] We report 2 cases of Page kidney caused by posttraumatic subcapsular hematoma that failed to improve with percutaneous drainage but resolved following laparoscopic decortication and evacuation. The Institutional Review Board waived the requirement for patient consent owing to the use of only pre-existing data
Case presentations
Case 1
A 25-year-old man with the chief complaint of new-onset hypertension reported a fall while playing ice hockey approximately 8 months prior to his presentation and a subsequent long-standing and large bruise on his right flank. He developed vague abdominal pain and underwent abdominal ultrasonography to evaluate possible cholecystitis. The gallbladder could not be visualized due to a large right renal cyst. Computed tomography revealed significant compression of the renal parenchyma by a 15×16×19 cm right renal cyst with internal debris (Figure 1). This cyst compressed both the right kidney and the pancreas. He underwent image-guided aspiration of the cyst, which collected 2500 mL of bloody fluid without malignant cells. One week later, computed tomography revealed a slight interval decrease in the size to 15×12×14 cm. The new-onset hypertension was being managed with 20 mg of lisinopril once daily. He also presented with new-onset gastro-esophageal reflux, which was managed with 75 mg of ranitidine once daily.
Figure 1.
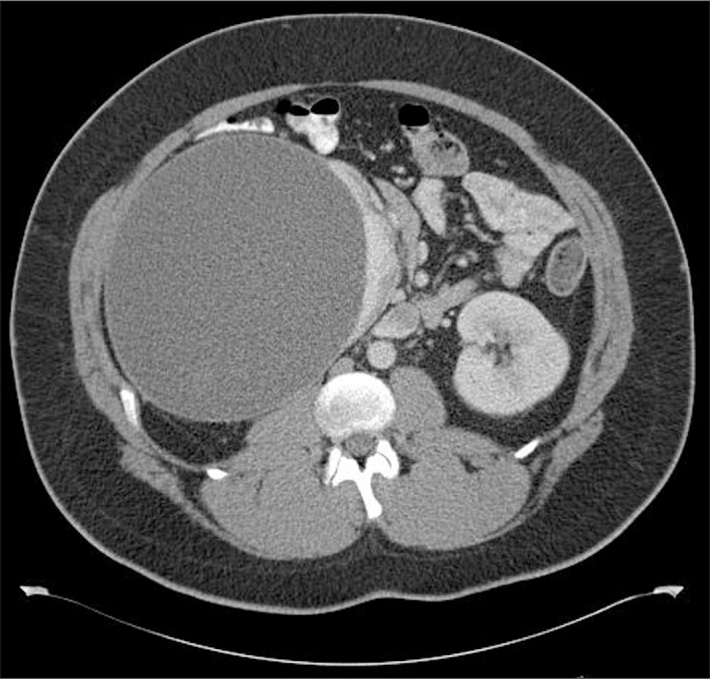
Subcapsular hematoma of the right kidney on computed tomography
At the time of presentation to our clinic, he reported persistent abdominal pain without particular aggravating or alleviating factors. A physical examination revealed systolic and diastolic blood pressures of 110 and 80 mmHg, respectively. Flank ecchymosis and costovertebral angle tenderness were not present. A complete blood count and basic metabolic panel were unremarkable.
Due to the persistent pain and new-onset hypertension, surgical renal decortication was elected. The patient underwent right hand-assisted transperitoneal laparoscopic renal cyst decortication and evacuation of the cystic structure, which appeared to be a subcapsular hematoma. There were no peri-operative complications, and the patient was discharged home on postoperative day 1. His abdominal pain resolved. Within 3 weeks, the lisinopril was discontinued, and his blood pressure remained normal. Post-procedure ultrasonography confirmed complete drainage (Figure 2), and pathology revealed a benign cyst wall.
Figure 2.

Preoperative (A) and postoperative (B) ultrasonography of the right kidney showing the complete disappearance of the fluid collection
Case 2
An 18-year-old male football player who did not report any remarkable trauma but was involved in high-velocity contact sports on a daily basis presented to his school nurse with significant headaches along with episodic blurry vision and left flank pain. He was found to be hypertensive, with a systolic blood pressure over 200 mmHg. He was hospitalized for 10 days and underwent an evaluation for secondary hypertension. Endocrine testing and laboratory testing were normal, but computed tomography revealed a significant compression of the left renal parenchyma by an 11×9×12 cm subcapsular fluid collection (Figure 3). Despite medical treatment with 10 mg of amlodipine and 0.1 mg of clonidine daily, his systolic blood pressure remained elevated in the range of 180 mmHg.
Figure 3.

Subcapsular hematoma of the left kidney on computed tomography
The patient underwent ultrasound-guided percutaneous drainage of the subcapsular fluid collection. Immediate post-procedure ultrasonography confirmed virtually complete drainage (Figure 4). There was an initial resolution of the hypertension following aspiration, but the collection re-accumulated, and the hypertension recurred. A repeat CT scan confirmed almost complete reconstitution of the left perirenal hematoma.
Figure 4.

Ultrasonography of the left kidney before (A) and after (B) aspiration of the subcapsular fluid collection showing the almost complete disappearance of the fluid collection
The patient underwent left transperitoneal laparoscopic renal decortication and evacuation of the hematoma 2 months after the percutaneous drainage. The thick cyst wall was excised, and the entire hematoma was evacuated (Figures 5, 6). There were no peri-operative complications, and the patient was discharged home on postoperative day 1. Anti-hypertensive therapy was withdrawn, and his blood pressure remained normal. Pathology revealed no evidence of malignancy.
Figure 5.
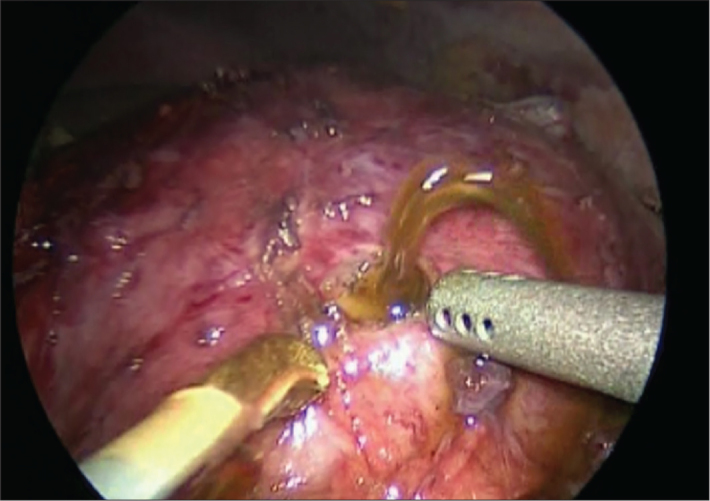
Initial laparoscopic incision into the subcapsular fluid collection
Figure 6.
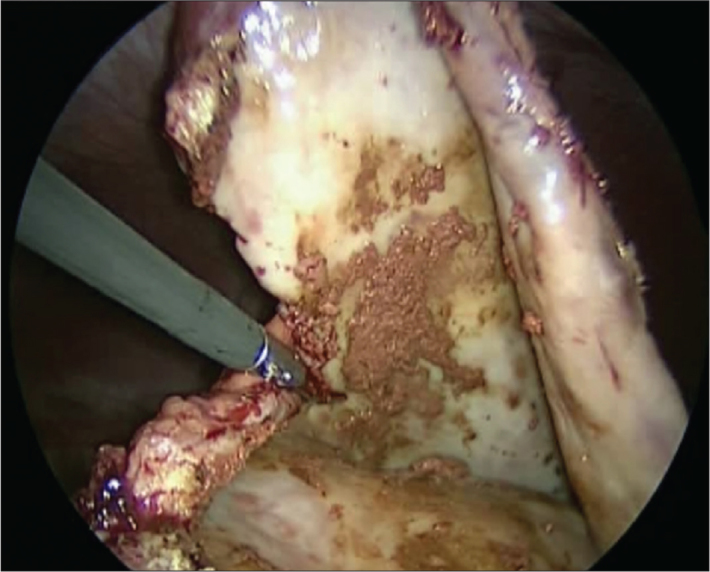
Laparoscopic excision of the subcapsular hematoma wall and evacuation of the contents
Discussion
Page kidney was first defined by Page[6] in 1939 when he wrapped a canine kidney with cellophane and observed the ensuing hypertension, which he proposed to be caused by renal ischemia and hypoperfusion (although others have suggested that the hypertension in this setting may be the result of interstitial nephritis and inflammation due to kidney compression).[7] Clinically, the first case of hypertension due to a subcapsular hematoma was reported in 1955 by Engel et al.,[8] occurring in a young football player who suffered blunt trauma to the kidney.
Because there is a large space between Gerota’s fascia and the kidney, a large hemorrhage is required to compress the kidney. In contrast, even a small hemorrhage can cause significant compression under the renal capsule even if it is not large enough to cause hemostatic instability. Hypertension with a normal serum creatinine level is the classic presentation of Page kidney in the presence of a subcapsular renal hematoma. The onset of hypertension in Page kidney is generally gradual. When the contralateral kidney is functional, the creatinine level is not typically elevated.[4] Both of our patients had normal contralateral kidneys, and their creatinine levels were normal. Diagnosis is confirmed with imaging, and computed tomography provides more information than ultrasonography.[9]
Since 1955, more than 100 cases of Page kidney have been reported. The majority followed an episode of renal trauma, including sports and traffic accidents, extracorporeal shock-wave lithotripsy, and kidney biopsies.[10] Nontraumatic causes have included tumors, urinomas, and lymphoceles.[10] Smyth et al.[11] reported 26 cases of Page kidney that were divided into 2 groups, traumatic and nontraumatic. They found that traumatic patients were younger and that half of the nontraumatic patients had a prior history of hypertension. Furthermore, all patients that required nephrectomy were in the nontraumatic group. Both of our patients were similar, in that they were young and previously normotensive and had Page kidneys related to trauma. In a literature review, Dopson et al.[10] found that external trauma was the primary cause of Page kidney before 1991. After 1991, Page kidneys were more common due to invasive medical procedures such as kidney transplant biopsies.[4,10]
Regardless of the pathogenesis, the aims of treatment are to reduce the blood pressure and prevent the loss of kidney function. The initial management is medical, addressing the hypertension, and angiotensin-converting enzyme inhibitors are particularly useful.[12] Surgical management to remove the offending subcapsular hematoma has historically been performed with open surgery, but recent experience has focused on minimally invasive techniques. Percutaneous drainage is the most successful in cases of newly formed hematomas but is unlikely to resolve older (organized) hematomas.[1] If the blood pressure is not improved despite medical treatment and percutaneous drainage fails (as in our cases), surgical decortication is recommended. Our cases demonstrate that laparoscopic treatment can be successful, with minimal treatment-related morbidity.
We are aware of only 3 prior English-language reports of Page kidney decortication with laparoscopic techniques.[13–15] The first was reported in 1998 by Graham et al.,[13] who performed laparoscopic decompression of a unilateral subcapsular hematoma causing a Page kidney that occurred after shock wave lithotripsy. In 2007, Duchene et al.[14] reported the staged laparoscopic decortication of bilateral subcapsular hematomas causing a Page kidney, also due to shock wave lithotripsy. In 2002, Castle et al.[15] described a retroperitoneoscopic approach to hematoma decompression in a case similar to our cases; the patient was a young male athlete with sports-related trauma requiring surgical decortication following unsuccessful percutaneous drainage.
In conclusion, Page kidney is an uncommon entity that causes secondary hypertension. If medical treatment and percutaneous drainage fail, then laparoscopic decortication can be performed with high effectiveness and low treatment-related morbidity.
Footnotes
Peer-review: Externally peer-reviewed.
Author Contributions: Concept - J.S.W., S.Ç.; Design - J.S.W., S.Ç.; Supervision - J.S.W., S.Ç.; Funding - J.S.W., S.Ç.; Materials - J.S.W., S.Ç.; Data Collection and/or Processing - J.S.W., S.Ç.; Analysis and/or Interpretation - J.S.W., S.Ç.; Literature Review - J.S.W., S.Ç.; Writer -J.S.W., S.Ç.; Critical Review - J.S.W., S.Ç.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study has received no financial support.
References
- 1.McCune TR, Stone WJ, Breyer JA. Page kidney: case report and review of the literature. Am J Kidney Dis. 1991;18:593–9. doi: 10.1016/s0272-6386(12)80656-1. [DOI] [PubMed] [Google Scholar]
- 2.Haydar A, Bakri RS, Prime M, Goldsmith DJ. Page kidney-a review of the literature. J Nephrol. 2003;16:329–33. [PubMed] [Google Scholar]
- 3.Posadas MA, Yang V, Ho B, Omer M, Batlle D. Acute renal failure and severe hypertension from a page kidney post-transplant biopsy. ScientificWorldJournal. 2010;10:1539–42. doi: 10.1100/tsw.2010.150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Butt FK, Seawright AH, Kokko KE, Hawxby AM. An unusual presentation of a Page kidney 24 days after transplantation: case report. Transplant Proc. 2010;42:4291–4. doi: 10.1016/j.transproceed.2010.09.042. [DOI] [PubMed] [Google Scholar]
- 5.Davies MC, Perry MJ. Urological management of ‘page kidney’. BJU Int. 2006;98:943–4. doi: 10.1111/j.1464-410X.2006.06432.x. [DOI] [PubMed] [Google Scholar]
- 6.Page I. The production of persistent arterial hypertension by cellophane perinephritis. JAMA. 1939;113:2046–8. [Google Scholar]
- 7.Vanegas V, Ferrebuz A, Quiroz Y, Rodriguez-Iturbe B. Hypertension in Page (cellophane-wrapped) kidney is due to interstitial nephritis. Kidney Int. 2005;68:1161–70. doi: 10.1111/j.1523-1755.2005.00508.x. [DOI] [PubMed] [Google Scholar]
- 8.Engel WJ, Page IH. Hypertension due to renal compression resulting from subcapsular hematoma. J Urol. 1955;73:735–9. doi: 10.1016/S0022-5347(17)67466-4. [DOI] [PubMed] [Google Scholar]
- 9.Yan MT, Lin SH, Wu CC, Chen CC. A hypertensive woman with an abnormal abdominal X-ray. ‘Page kidney’ caused by a chronic subcapsular hematoma. Kidney Int. 2009;76:801–2. doi: 10.1038/ki.2009.290. [DOI] [PubMed] [Google Scholar]
- 10.Dopson SJ, Jayakumar S, Velez JC. Page kidney as a rare cause of hypertension: case report and review of the literature. Am J Kidney Dis. 2009;54:334–9. doi: 10.1053/j.ajkd.2008.11.014. [DOI] [PubMed] [Google Scholar]
- 11.Smyth A, Collins CS, Thorsteinsdottir B, Madsen BE, Oliveira GH, Kane G, et al. Page kidney: etiology, renal function outcomes and risk for future hypertension. J Clin Hypertens (Greenwich) 2012;14:216–21. doi: 10.1111/j.1751-7176.2012.00601.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.John J, Allen S, Perry M, Patel HR, O’Brien T. Page kidney phenomenon presenting as acute renal failure after partial nephrectomy: a case report and review of the literature. Urol Int. 2008;80:440–3. doi: 10.1159/000132705. [DOI] [PubMed] [Google Scholar]
- 13.Graham CW, Lynch SC, Muskat PC, Mokulis JA. Laparoscopic evacuation of a subcapsular renal hematoma causing symptomatic hypertension. J Endourol. 1998;12:551–3. doi: 10.1089/end.1998.12.551. [DOI] [PubMed] [Google Scholar]
- 14.Duchene DA, Williams RD, Winfield HN. Laparoscopic management of bilateral page kidneys. Urology. 2007;69:1208. doi: 10.1016/j.urology.2007.02.040. [DOI] [PubMed] [Google Scholar]
- 15.Castle EP, Herrell SD. Laparoscopic management of page kidney. J Urol. 2002;168:673–4. [PubMed] [Google Scholar]