

Abstract
Metastatic masses in the kidney are rare, and metastasis of pancreatic adenocarcinoma to the kidney is even rarer. A 58-year-old male patient with macroscopic hematuria presented to the emergency department. Abdominopelvic computed tomography revealed a lesion that was not visualized as a complete mass but instead appeared as a patch extending from the pelvis to the parenchyma. Biopsy indicated metastasis of pancreatic adenocarcinoma to the right kidney. These findings indicate that metastatic pancreatic adenocarcinoma should be considered in patients presenting with hematuria and findings of patch-like suspicious masses in the right kidney. After diagnosis is confirmed by prompt biopsy, chemotherapy should be initiated to prolong the patient’s life. To the best of our knowledge, the present case is the first report of renal metastasis from pancreatic adenocarcinoma in a living patient.
Keywords: Hematuria, metastasis of pancreatic adenocarcinoma, metastatic kidney tumors, renal metastasis from pancreatic adenocarcinoma
Introduction
Metastatic renal masses are rare. While the primary organs causing renal metastases are lungs and breasts, gastrointestinal tumors, malignant melanoma, and gynecologic and hematologic malignancies are also known to cause metastases.[1] Although these metastases generally occur hematogenously, some metastases are believed to spread to the adjacent organs from the colon, adrenal gland, and rarely, the pancreas. In a series of 5000 autopsies, Klinger et al. found 17 cases of renal metastasis from lung cancer, 11 from stomach cancer, 9 from breast cancer, 7 from pancreatic cancer, 4 from esophageal cancer, 7 from other gastrointestinal malignancies, and 1 from malignant melanoma.[2] However, it is not clear in this autopsy series whether metastasis occurred from the pancreas or as an adjacent invasion.
Although renal metastases are generally clinically silent, some patients may develop flank pain or hematuria. Renal metastases are commonly multifocused and smaller than 3 cm in diameter and are known to occur with non-renal metastases.[1] Computed tomography (CT) is the primary diagnostic tool for renal metastases, revealing isodense masses that range from 5 to 30 Hounsfield units (HU).[3] Percutaneous renal biopsy performed on these masses provides pathological confirmation,[4] and these patients are usually treated with systemic treatment. In detected metastatic pancreatic cancer, survival can be prolonged up to 11.1 months by use of various chemotherapeutic agents.[5] In this report, we present a very rare case of metastasis of pancreatic adenocarcinoma to the right kidney in a living patient.
Case presentation
A 58-year-old male patient presented to the emergency department with hematuria. The patient had undergone coronary bypass 6 years ago and splenectomy (on account of a car accident) 9 years ago. Physical examination revealed no pathology except the scars of the previous surgeries. Complete blood count and routine blood tests were normal; abundant erythrocytes were detected in urine analysis by the dipstick test. The patient’s direct urinary tract radiography was normal. Complete abdominal ultrasonography revealed 2–3 g hydronephrosis in the right kidney. Abdominal CT showed increased kidney dimensions, particularly in the right renal midsection; decreased cortex-medulla distinction; thinning at the middle and inferior part of the cortex; and a patch-like lesion lacking a clear image extending from the renal pelvis to the cortex (Figure 1a, b). Other organs and tissues were reported as normal. Further examination was planned but the patient did not return on the scheduled date.
Figure 1. a, b.
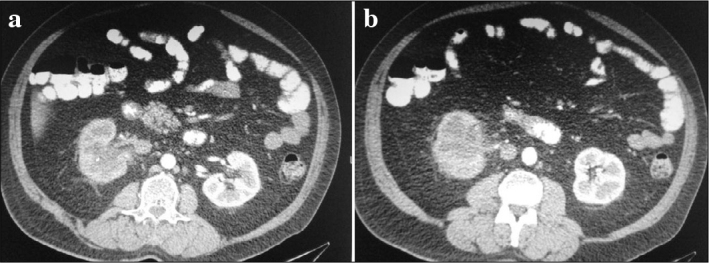
Axial CT. Image of an unclear patch-like extending from the renal pelvis to the cortex
CT: computed tomography
Three months after the initial presentation, the patient was hospitalized in the chest diseases department on account of pulmonary embolism. Magnetic resonance imaging (MRI) was performed after the embolism resolved, and a 3 × 2 cm mass covering most of the right kidney was observed in the pancreatic uncinate process adjacent to the duodenum in the axial plane (Figure 2). Tumor thrombus was detected in the right renal vein and vena cava. In addition, a few 3 × 2.5 cm masses were observed in the right surrenal gland, a 2.5 × 1.5 cm mass was noted in the left surrenal gland in the axial plane, and 2 × 1.5 cm masses were identified at the liver segment 6–7 junction; all masses were identified as metastatic lesions. Before deciding on a treatment regimen, Tru-cut biopsy of the right kidney and fine-needle aspiration biopsy of the pancreas were performed to determine the stage of the disease. Aspiration biopsy performed at the top of the pancreas was positive for malignancy and cytological findings were reported to be compatible with ductal adenocarcinoma. Histopathological examination of renal biopsy revealed tumoral infiltration in the renal parenchyma. The tumor consisted of atypical epithelial cells making tubular structures. Glomeruli were preserved (Figure 3). Immunohistochemical examination showed cytokeratin (CK) 18 and 19 expression in the tumor cells; cluster of differentiation (CD) 10 and renal cell carcinoma marker were negative (Figure 4). Shortly after diagnosis, the patient’s overall condition deteriorated and he eventually died of multiple organ failure.
Figure 2. a–d.

An axial contrast-enhanced T1-weighted MR image shows an enhanced lesion in the pancreatic uncinate process (curved arrow), with metastases to the right kidney (arrow) adjacent to the right renal vein and inferior vena cava tumor thrombus (double arrows) (a). Contrast-enhanced coronal T1-weighted MR image shows in the right kidney (arrow), right adrenal gland (star), liver (arrowhead) metastases (b). Diffusion weighted and (c) Apparent diffusion coefficient map image restricted diffusion throughout right kidney (arrow) (d)
MR: magnetic resonance
Figure 3. a, b.
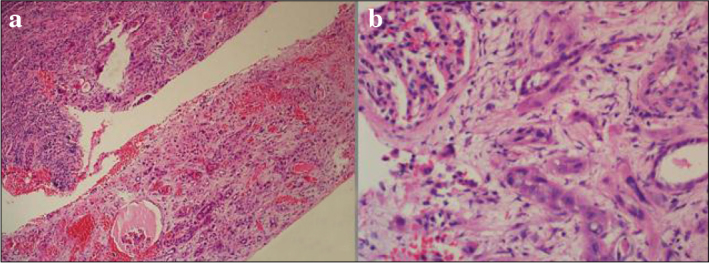
Histopatholological examination (a). A tumoral lesion infiltrating the renal parenchyma without a capsule (hematoxylin & eosin, ×40) (b). Tumor-making tubular structures in the desmoplastic stroma (hematoxylin & eosin, ×200). An intact glomerulus is also discernable
Figure 4. a–c.
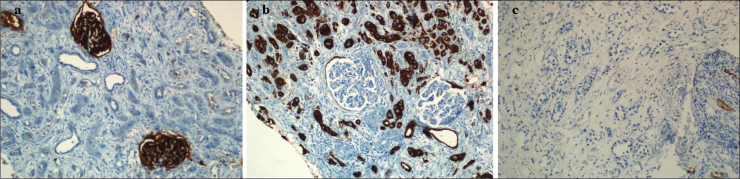
Immunohistochemical staining (a). CD10 expression in glomeruli. The tumor is negative (×100) (b). CK18 expression in the tumor; it is negative in glomeruli (×200) (c). Negative renal cell carcinoma marker
CD: cluster of differentiation, CK: cytokeratin
Discussion
Although pancreatic cancer rarely results in renal metastasis, renal involvement may occur in the form of invasion to the adjacent left kidney. In the present case, pancreatic cancer metastasis to the right kidney in the form of a single lesion was identified after the patient presented to the hospital for hematuria. Complaints of hematuria are rare in this patient population. Furthermore, renal metastases are multifocused, with lesions smaller than 3 cm, and do not cause deterioration of renal contours.[1]
Renal biopsy is commonly used to confirm the diagnosis of small renal tumors and when renal metastasis from other organs is suspected. Even if pancreatic cancer is undetected by imaging techniques, it should be considered in the differential diagnosis of an unclear patch-like lesion in the kidney, and renal biopsy should be performed without delay in such cases. In the present case, the patient did not return for the scheduled examination, leading to a delay in diagnosis, and he eventually died 3 months later. Nevertheless, it is known that with early diagnosis of metastatic pancreatic cancer, a patient’s life can be prolonged by chemotherapy.[5]
In conclusion, the first symptom for pancreatic cancer may be hematuria due to renal metastases. Pancreatic metastases should be considered in the differential diagnosis of suspicious masses determined in the right kidney. Early diagnosis of pancreatic cancer can prolong patients’ lives.
Footnotes
Peer-review: Externally peer-reviewed.
Author Contributions: Concept - E.M., Z.A.; Design - E.M., Z.A.; Supervision - E.M., Z.A.; Funding - E.M., Z.A.; Materials - K.K., A.H.; Data Collection and/or Processing - E.M., Z.A.; Analysis and/ or Interpretation - E.M., Z.A.; Literature Review - E.M., Z.A.; Writer - E.M., Z.A.; Critical Review - E.M., Z.A.; Other - E.M., Z.A., K.K., A.H.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study has received no financial support.
References
- 1.Pollack HM, Banner MP, Amendola MA. Other malignant neoplasms of the renal parenchyma. Semin Roentgenol. 1987;22:260–74. doi: 10.1016/0037-198x(87)90052-6. http://dx.doi.org/10.1016/0037-198X(87)90052-6. [DOI] [PubMed] [Google Scholar]
- 2.Klinger ME. Secondary tumors of the genito-urinary tract. J Urol. 1951;65:144–53. doi: 10.1016/S0022-5347(17)68470-2. [DOI] [PubMed] [Google Scholar]
- 3.Ferrozzi F, Bova D, Campodonico F. Computed tomography of renal metastases. Semin Ultrasound CT MR. 1997;18:115–21. doi: 10.1016/s0887-2171(97)90055-x. http://dx.doi.org/10.1016/S0887-2171(97)90055-X. [DOI] [PubMed] [Google Scholar]
- 4.Sánchez-Ortiz RF, Madsen LT, Bermejo CE, Wen S, Shen Y, Swanson DA, et al. A renal mass in the setting of a nonrenal malignancy: When is a renal tumor biopsy appropriate? Cancer. 2004;101:2195–201. doi: 10.1002/cncr.20638. http://dx.doi.org/10.1002/cncr.20638. [DOI] [PubMed] [Google Scholar]
- 5.Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011;364:1817–25. doi: 10.1056/NEJMoa1011923. http://dx.doi.org/10.1056/NEJMoa1011923. [DOI] [PubMed] [Google Scholar]