

Abstract
Background and aim
Short sleep duration is associated with significant negative consequences, including poor school performance, behavioral problems, obesity, and hypertension. There is prior evidence that there are disparities in sleep duration related to ethnicity; however, there are no specific data on Hispanic children. We aimed to test the hypothesis that there are ethnic differences in parent-reported sleep duration in a community-based cohort of Hispanic and Caucasian children.
Methods
We examined the parent-reported sleep patterns of a community-based prospective cohort (Tucson Children’s Assessment of Sleep Apnea study (TuCASA)) involving 338 Hispanic and Caucasian children at two time points approximately 5 years apart.
Results
In the initial phase of the TuCASA study with a cohort median age of 8.8 years (interquartile range (IQR), 7.6–10.1 years), parent-reported sleep duration during weekdays was shorter in Hispanic (median, 9.5 h; IQR, 9.0, 10.0 years) than in Caucasian children (10 h; IQR, 9.5, 10.0 h; p < 0.0001); however, this difference was not seen 5 years later when the cohort was older (median age, 13.3 years; IQR, 11.9–14.6 years; p = 0.43). In addition, Hispanic children had a significantly later bedtime at both time points (p < 0.02). In the initial phase, parent-reported sleep duration during weekends tended to be shorter in Hispanic than in Caucasian children (p = 0.06).
Conclusions
Short sleep duration in Hispanic children may contribute to health disparities. Our research suggests that in Hispanic children, behavioral interventions toward improving sleep duration accomplished by earlier bedtimes or delayed school start times and mechanistic studies to unravel any inherent tendency toward a delayed sleep phase are needed.
Keywords: Health status disparities, Sleep, Sleep deprivation, Hispanic americans, Circadian rhythm
Introduction
Insufficient sleep has been identified as a growing problem in children, with an estimated 1 h of sleep time lost over the past century [1]. Up to 63% of adolescents report that they do not get sufficient sleep [2]. Insufficient sleep and short sleep duration have been associated with a variety of negative outcomes. There is significant evidence linking short sleep duration in children to an increased risk of obesity [3–7], increased blood pressure [8], and worse diabetic control [9]. Decreased sleep duration of as little as 30 min has been shown to increase metabolic risk in adolescents [10]. Short sleep duration has also been associated with behavioral and cognitive problems [11], as well as worse performance in school [12–14]. Short sleep duration has also been related to increased risk-taking behaviors [15], accidents [16], and a greater risk of developing depressive symptoms [17], including an increased risk of suicidal ideation [18]. Such supporting data have led to the Healthy People 2020 objective that adolescent children get sufficient sleep [19]. However, social and demographic factors contributing to sleep deficiency in children remain inadequately described [20].
There is limited information related to ethnicity-related differences in sleep duration, particularly in children [20]. Previous adult literature has shown that Black race and Hispanic ethnicity are associated with an increased risk of short sleep duration [21,22], although there is some conflicting evidence, with other studies showing that Hispanic ethnicity is not associated with an increased risk of short sleep duration [23]. Previous studies have shown that minority children (mostly African American) were more likely to have delayed bedtimes [24,25]. Minority boys (mostly African American) have also been shown to have decreased sleep duration relative to nonminority boys [24]. Although there is emerging evidence of such racial disparities in sleep duration in children, there are no specific data on the relationship between Hispanic ethnicity and sleep duration in children.
In adults, there is literature suggesting that ethnicity-related factors in sleep duration may contribute to health disparities. For example, in adults, decreased sleep duration is associated with an increased risk of obesity [26], and such an association is seen in Mexican Americans, but not in Cuban Americans or Puerto Ricans [27]. This association has also been described in Mexican-American children [28]. In our study, we aimed to test the hypothesis that there are ethnic differences in parent-reported sleep duration in a community-based cohort of Hispanic and Caucasian children. Knowledge derived from such a study would allow us to better identify and increase sleep duration in children, and to reduce health disparities that owe their origins to insufficient sleep.
2. Methods
2.1. Study population
This analysis was done on phase 1 and phase 2 of the Tucson Children’s Assessment of Sleep Apnea cohort (TuCASA) study. A detailed description of the TuCASA study and recruitment has been reported elsewhere [29,30]. In brief, a representative sample of 503 elementary school-aged Caucasian and Hispanic children were recruited from the Tucson Unified School District, a large district representative of the Tucson population. Approximately 5 years later (mean, 4.7 years), 348 children participated in phase 2 of the study. The TuCASA study was approved by the University of Arizona Institutional Review Board, and by the Tucson Unified School District Research Committee. Before undergoing study-related procedures, written informed consent and minor’s assent were obtained from the parents and children, respectively. Families completed detailed sleep questionnaires, including socioeconomic information, and children underwent anthropomorphic measurements.
2.2. Questionnaires
Families filled out sleep questionnaires about their child, including questions related to bedtime, wake time, and average sleep duration. This information was obtained for weekdays as well as for weekends. Socioeconomic information was also derived from the questionnaires. This information included family-reported household income, parental education, as well as ethnicity. Household income was obtained on a scale ranging from <$5000 annual income to >$50,000 annual income, in $5000 increments. Parental education (of the caregiver filling out the survey) was assessed using a scale starting at high school education or less to greater than 4 years of college or professional school. The scale was subdivided into 1-year increments for the completion of technical/trade school or college.
2.3. Anthropometry
Anthropometric measurements were completed in the children’s home. Weight was obtained as the average of three measurements, to the nearest of 0.1 kg. Height was measured using a folding ruler on a level surface after the removal of shoes, and the head in the Frankfort plane. The average of three measurements to the nearest of 0.1 cm was used for data analysis. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared. BMI percentiles for age and gender were calculated using Center for Disease Control growth charts [31].
2.4. Data analysis
Statistical analysis was performed using Statistical Package for Social Science (SPSS) Version 22 (IBM, Armonk, NY, USA). Data were assessed for a normal distribution using a one-sample Kolmogorov– Smirnov test. For data analysis, household income was collapsed into a binary value of less than or greater than $40,000 annual income. This threshold income was chosen because it was close to the median annual household income in Tucson, AZ, at the time of data collection ($38,800) [32]. Parental education was converted into a binary value of less than or greater than 4 years of college. Subjects were grouped by ethnicity for data analysis. For demographic factors, χ2 tests were used to determine significant differences for categorical variables (gender, household income, and parental education), and two-sided t-tests were used to determine significance for continuous variables. Measures included weekday and weekend sleep duration, as well as weekday bedtime and awakening time at both phases 1 and 2. Sleep duration was measured as a continuous variable because the two time points examined represent different developmental phases, with different sleep requirements. Ethnicity was used as a fixed factor for modeling. Covariates included age, gender, BMI percentile, household income, and parental education. Analyses of covariance (ANCOVAs) were performed at time points one and two, and a generalized linear model with repeated measures was constructed to evaluate the change in variables over time. A p-value of <0.05 was considered to be significant.
3. Results
Of the 348 children who participated in both phase 1 and phase 2 of the TuCASA study, 338 children provided sufficient information to be included in data analysis. With respect to demographic data, significant differences were seen in BMI, parental education, and household income between Hispanic and Caucasian children (Table 1). During weekdays, Hispanic children slept less than Caucasian children at phase 1 (9.5 h vs. 10 h, p < 0.0001), and they went to bed at a later time (9 pmvs. 8:30 pm, p < 0.0001). At phase 2, however, sleep duration was not significantly different between Hispanic and Caucasian children (8.5 h vs. 9.0 h, p = 0.13). There continued to be, however, a significant difference in bedtime with delayed bedtime in Hispanic than in Caucasian children (Table 1, p = 0.013). A significant difference in unadjusted parent-reported sleep duration on weekends was observed in phase 1, with Hispanic children getting less sleep than Caucasian children (median, 9.5 h compared with 10 h). This was no longer significant at phase 2.
Table 1.
Demographic factors and unadjusted parent-reported sleep habits in Hispanic and Caucasian children.
| Hispanic (n = 123) | Caucasian (n = 215) | p | |
|---|---|---|---|
| Gender | 0.172 | ||
| Male | 69 (56%) | 104 (48%) | |
| Female | 54 (49%) | 111 (52%) | |
| Phase 1 age (years) | 9.0 (7.6–10.1) | 8.7 (7.5–10.1) | 0.746 |
| Phase 2 age (years) | 13.7 (12.3–14.8) | 13.1 (11.8–14.5)4 | 0.114 |
| Phase 1 BMI percentile | 73.6 (45.0–93.8) | 56.3 (25.9–85.5) | 0.001 |
| Phase 2 BMI percentile | 82.0 (56.4–95.6) | 61.6 (30.9–88.8) | <0.0001 |
| Education | <0.0001 | ||
| <4 years of college | 88 (72%) | 99 (46%) | |
| 4 years of college or professional degree | 35 (28%) | 116 (54%) | |
| Annual Household Income | <0.0001 | ||
| <$40,000 | 65 (53%) | 71 (33%) | |
| >$40,000 | 58 (47%) | 144 (67%) | |
| Phase 1 Weekday Sleep Duration (hours) | 9.5 (9.0–10.0) | 10 (9.5–10) | <0.0001 |
| Phase 2 Weekday Sleep Duration (hours) | 8.5 (8.0–9.0) | 9.0 (8.0–9.0) | 0.13 |
| Phase 1 Weekday Bedtime | 21:00 (20:30–21:30) | 20:30 (20:00–21:00) | <0.0001 |
| Phase 2 Weekday Bedtime | 21:30 (21:00–22:00) | 21:30 (21:00–22:00) | 0.013 |
| Phase 1 Weekday Wake Time | 7:00 (6:30–7:00) | 6:45 (6:30–7:00) | 0.16 |
| Phase 2 Weekday Wake Time | 6:30 (6:00–7:00) | 6:30 (6:00–7:00) | 0.847 |
| Phase 1 Weekend Sleep Duration (hours) | 10.0 (9.0–10.5) | 10.0 (9.5–10.5) | 0.003 |
| Phase 2 Weekend Sleep Duration (hours) | 9.5 (8.5–10.0) | 9.5 (9.0–10.0) | 0.243 |
Data are presented as median (interquartile range). For phase 1 weekday bedtime, a significant difference is seen due to a mean bedtime of 9:40 pm in Hispanic children, compared with a mean bedtime of 9:27 pm in Caucasian children. Similarly, for phase 1 weekend sleep duration, a significant difference is seen due to a mean duration of 9.4 h compared with 9.7 h, and for phase 2 weekday bedtime, a mean of 21:40 compared with 21:27 in Hispanic and Caucasian children, respectively.
To adjust for the significant demographic differences between the two groups, ANCOVAs were performed at phase 1 and phase 2 (Tables 2 and 3). Covariates included age, gender, parental level of education, household income, and BMI at the time of survey. All 338 children were included for analysis at phase 1, and 313 (114 Hispanic and 199 Caucasian) children were included at phase 2, because of some children with missing data for BMI at phase 2 (n = 25). Exclusion of these children from the analysis of phase 1 data did not materially change the results.
Table 2.
Analysis of covariance results comparing weekday and weekend sleep durations of Hispanic and Caucasian children.
| Variable | Phase 1 Weekday Sleep Duration (B/SE) |
Phase 1 Weekend Sleep Duration (B/SE) |
Phase 2 Weekday Sleep Duration (B/SE) |
Phase 2 Weekend Sleep Duration (B/SE) |
|---|---|---|---|---|
| Age | −0.141 (0.270)** | −0.095 (0.033)* | −0.290 (0.028)** | −0.074 (0.042) |
| Female Gender | 0.094 (0.025) | 0.256 (0.108)* | 0.073 (0.096) | 0.460 (0.144)* |
| College Education | 0.061(087) | 0.174 (0.116) | −0.016 (0.104) | 0.022 (0.156) |
| Household Income | <0.0001 (0.086) | 0.095 (0.115) | 0.035 (0.104) | 0.032 (0.155) |
| BMI percentile | −0.005 (0.001)** | −0.003 (0.002) | −0.002 (0.002) | −0.005 (0.002) |
| Hispanic | −0.374 (0.088)** | −0.219 (0.117) | −0.084 (0.430) | −0.042 (0.159) |
Hispanic children obtain significantly less sleep than Caucasian children at phase 1, but this difference is no longer present 5 years later in phase 2. There is no significant difference seen in weekend sleep duration between Hispanic and Caucasian children. Data are presented as B coefficient (standard error (SE)).
Abbreviation: BMI: Body Mass Index.
p < 0.05.
p < 0.0001.
Table 3.
Analysis of covariance results comparing weekday sleep schedules of Hispanic and Caucasian children.
| Variable | Phase 1 Weekday Bedtime (B/SE) |
Phase 1 Weekday Wake Time (B/SE) |
Phase 2 Weekday Bedtime (B/SE) |
Phase 2 Weekday Wake Time (B/SE) |
|---|---|---|---|---|
| Age | 0.118 (0.020)** | −0.009 (0.018) | 0.212(0.023)** | −0.055 (0.021)* |
| Female Gender | −0.029 (0.063) | 0.017 (0.057) | −0.050(0.078) | −0.054 (0.072) |
| College Education | 0.020 (0.068) | −0.030 (0.061) | 0.161 (0.085) | 0.089 (0.078) |
| Household Income | 0.115 (0.068) | −0.004 (0.061) | −0.002(0.084) | −0.074 (0.077) |
| BMI percentile | 0.003 (0.001)* | <0.0001 (0.001) | <0.0001(0.001) | −0.002 (0.001)* |
| Hispanic | 0.453 (0.069)** | 0.080 (0.062) | 0.213(0.086)* | 0.087 (0.079) |
Compared with Caucasian children, Hispanic children maintain a later bedtime at both phase 1 and phase 2. There is no significant difference seen in wake time based on ethnicity. Data are presented as B coefficient (standard error (SE)).
Abbreviation: BMI: Body mass index.
p < 0.05.
p < 0.0001.
At phase 1, after adjustment for covariates, there continued to be a significant difference in weekday sleep duration between Hispanic and Caucasian children (adjusted mean, 9.4 vs. 9.7 h, p = 0.001). A significant difference in bedtime continued to be seen as well (adjusted mean, 8:58 pm in Hispanic children vs. 8:31 pmin Caucasian children, p < 0.0001). No significant difference was seen in awakening time after adjustment (adjusted mean, 6:48 am vs. 6:43 am, p = 0.20). After adjustment for covariates, a significant difference was no longer seen in weekend sleep duration between the two groups (adjusted mean, 9.4 vs. 9.7 h, p = 0.062).
At phase 2, after adjustment for covariates, no significant differences were seen in weekday sleep duration (8.6 h for both groups, p = 0.43), weekend sleep duration (Hispanic children 9.4 h vs. Caucasian children 9.5 h, p = 0.79), or weekday wake time (6:35 am in Hispanic children vs. 6:30 am in Caucasian children, p = 0.27). A significant difference was seen in weekday bedtime (9:40 pm in Hispanic children vs. 9:28 pm in Caucasian children, p = 0.014).
Finally, to model the difference between Hispanic and Caucasian children over time, a linear model with repeated measures was constructed (Fig. 1). Covariates included age, gender, parental level of education, household income, and BMI. For weekday sleep duration, significant factors included age (p < 0.0001) and ethnicity (p = 0.019). A significant difference was seen between Hispanic and Caucasian children. A similar effect was seen for weekday bedtime, with significant factors including age (p < 0.0001) and ethnicity (p = 0.006). No significant difference was seen for weekday wake time or weekend sleep duration.
Fig. 1.
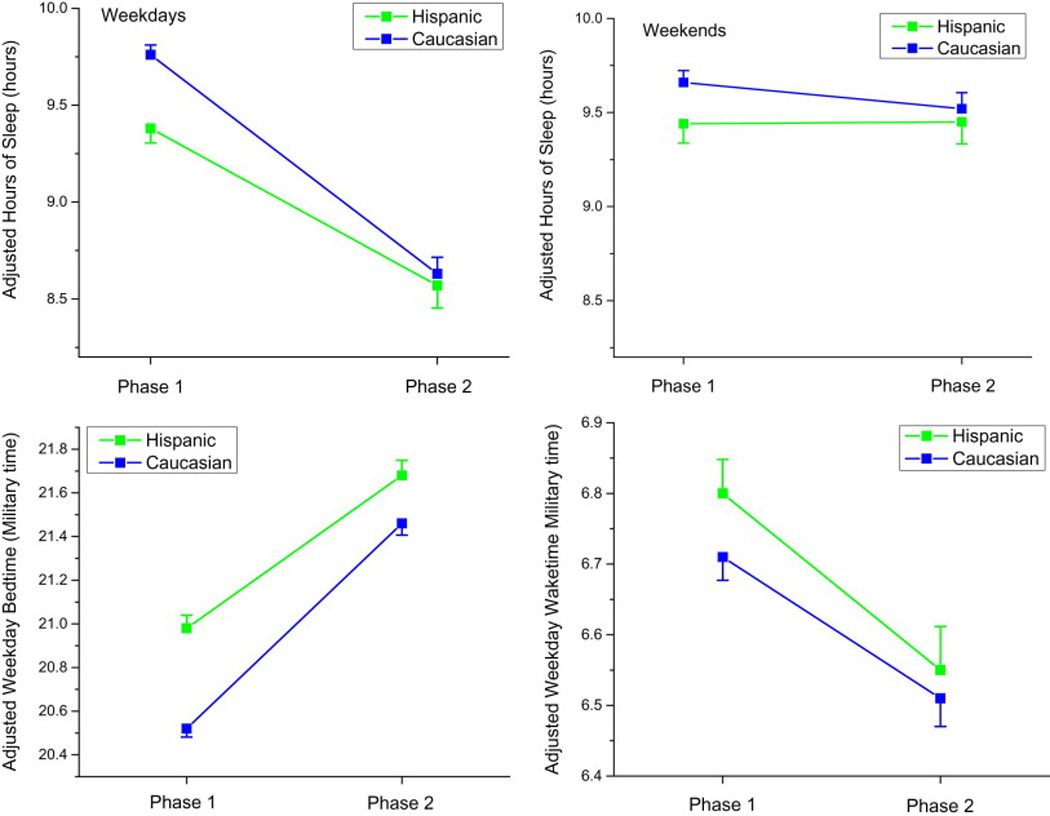
Changes in sleep duration, bedtime, and wake time over time. Left upper panel: weekday sleep duration; right upper panel: weekend sleep duration; left lower panel: weekday bedtime; right lower panel: weekday wake time. All graphs are after adjustment for covariates. Hispanic children slept significantly less than Caucasian children during phase 1, but at phase 2, this difference was no longer significant. Hispanic children also maintained a consistently later bedtime compared with Caucasian children at both time points. There were no significant differences in weekday wake time or weekend sleep duration at either time point.
4. Discussion
Our results show that Hispanic children obtain approximately 20 min less sleep per night during the school week than Caucasian children at elementary school age, but that this difference attenuates over the course of 5 years as they enter adolescence. The primary cause of this difference in sleep duration is that Hispanic children have a delayed bedtime compared with Caucasian children. Although in phase 2 of the TuCASA study, there was no longer a significant difference in weekday sleep duration, there was still a small but significant difference between bedtimes, with Hispanic children going to bed 12 min later. In both groups, a substantial decrease in weekday sleep duration was seen over time, with Hispanic children obtaining an adjusted mean of 48 min less sleep and Caucasian children obtaining an adjusted mean of 66 min less sleep per night 5 years after their initial survey.
Although 20 min may be considered to be a small amount of time, previous research in children has shown that sleep restriction of 30 min per night over a 5-day period decreases performance on neurocognitive testing, whereas sleep extension of 30 min has been shown to improve performance [33]. In addition, a delayed school start intervention in children showed that an increased sleep duration of only 16–22 min resulted in improved school performance and decreased daytime sleepiness [34]. Targeting this difference could potentially improve neurobehavioral outcomes. Of interest, the Hispanic children maintained a consistently later bedtime and wake time over the study compared with Caucasian children. Such a finding suggests that Hispanic children had an inherent preference for a relatively delayed sleep phase compared with Caucasian children. The delayed bedtime may either represent a cultural effect, or possibly a genetic effect because recent research has shown that circadian rhythm may vary with ethnicity [35]. Given that the American Academy of Pediatrics has recently issued a statement encouraging a delayed start time for high schools and junior highs [36], it is possible that this may be of particular benefit to Hispanic children.
Our results are congruent with previous studies, which have shown that minority children tend to obtain less sleep and have delayed bedtimes compared with Caucasian children [24,25]. However, to our knowledge, our study is the first to report a significant difference in sleep duration between Hispanic and Caucasian children, which is independent of socioeconomic class, age of child, parental educational level, and other potential confounders. We had previously compared self-reported versus recorded sleep time, and we had noticed differences by ethnicity [37]. However, we had not adjusted for potential confounders or recognized that delayed bedtimes were primarily responsible for such observed differences because ethnicity effect on sleep duration was not the primary focus. In addition, this analysis was done only at phase 1, and it was not longitudinal. Given that research has shown that health disparities may be due to differences in race, ethnicity, or socioeconomic strata [27], it is important to investigate if these factors contribute to health disparities independently of each other.
Although a difference in sleep duration was noted between the two ethnic groups at phase 1, there was no such difference in phase 2. While the unadjusted difference in sleep duration between Hispanic and Caucasian children trended toward significance (Table 1, p = 0.13), this effect did not persist after adjustment for covariates (Table 2, p = 0.43). The ethnic difference in sleep duration attenuated primarily due to the greater decline of sleep duration with age in Caucasian children when compared with Hispanic children. Conceivably, increased school and extracurricular activities may have uniformly imposed restrictions across both Caucasians and Hispanic school-going children. Alternatively, the ubiquitous poor sleep habits in both groups may have contributed to the loss of difference in sleep duration as the cohort aged. However, such assumptions are purely speculative on our part, and further investigation is needed to determine the cause of the lack of difference in sleep duration between Hispanic and Caucasian children as they age. It is interesting to note that prior research has shown no difference in the likelihood of short sleep duration between Hispanic and Caucasian adults [23], whereas the observed difference in sleep duration across ethnicities in early childhood may have developmental implications.
There are several limitations to our study. First, sleep duration was obtained through parental report. However, previous research has shown that parental report does correlate with actigraphic sleep monitoring, and it may be a sufficient measure [38]. In addition, a previous analysis completed in phase 1 of this cohort showed that although parents were likely to report longer sleep duration than polysomnography demonstrated, there was no systematic difference in such an overestimation across Hispanic and Caucasian families [37]. Second, Hispanic ethnicity in our cohort was likely almost exclusively of Mexican-American origin. The predominant Hispanic ethnic background in Tucson, AZ, is of Mexican-American descent, although detailed information regarding ethnic background beyond Hispanic or Caucasian was not obtained. Our findings may not be generalizable to other Hispanic children such as Puerto Rican or Cuban-American children. Third, it is possible that acculturation in the Hispanic children over time between phase 1 and phase 2 may have explained the lack of difference in sleep duration seen at phase 2. The cohort was selected to include only children who participated in both phases 1 and 2; therefore, selective attrition or consequent loss of statistical power is unlikely to explain this change. Future studies could examine factors related to acculturation, such as the language of preference at home and time in the United States to answer this question. Nevertheless, our study did have multiple strengths. First, it is a community-based cohort that was specifically designed to study healthy Hispanic and Caucasian children. Second, we were able to use multiple measures of socioeconomic status as covariates to allow us to examine ethnicity-specific differences in sleep that are not linked to family income or parental education level.
5. Conclusions
In this study, we report significant differences in sleep duration and patterns in Hispanic children compared with Caucasian children. There is a significant difference in sleep duration between elementary school-aged Hispanic and Caucasian children; however, this difference fades over time, and it is not present at adolescence. In addition, Hispanic children tend to have a consistently later bedtime than Caucasian children. These differences may have an impact in contributing to health disparities, and they may represent a modifiable target for future behavioral interventions.
Supplementary Material
Highlights.
• Short sleep duration is associated with multiple adverse health effects in children. • Hispanic children had a shorter sleep duration than Caucasian children at a young age. • Five years later, there was no longer a difference in sleep duration between the groups. • Hispanic children maintained a later bedtime at both time points.
Acknowledgments
This work was supported by the National Institutes of Health Grants (HL062373 to S.Q. and HL095748, HL095799 to S.P.); PCORI contract (IHS-1306-2505 to S.P); and salary support for D.C. from the Arizona Respiratory Center, University of Arizona, Tucson, AZ. The funding institutions did not have any role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of this manuscript; and decision to submit this manuscript for publication. The authors would also like to thank the families who participated in the TuCASA study. The authors would also like to thank the families who participated in the TuCASA study.
Abbreviations
- ANCOVA
Analysis of Covariance
- BMI
Body Mass Index
- TuCASA
Tucson Children’s Assessment of Sleep Apnea study
Footnotes
This work was conducted at the University of Arizona, Tucson, AZ, USA.
Conflict of interest
Dr. Parthasarathy reports grants from NIH/NHLBI, grants from the Patient-Centered Outcomes Research Institute, grants from the US Department of Defense, grants from NIH (National Cancer Institute) NCI, grants from the US Department of Army, grants from the Johrei Institute, personal fees from the American Academy of Sleep Medicine, personal fees from the American College of Chest Physicians, nonfinancial support from the National Center for Sleep Disorders Research of the NIH (NHLBI), personal fees from UpToDate Inc., personal fees from Philips Respironics, Inc., grants from Younes Sleep Technologies, Ltd., grants from Niveus Medical Inc., grants from Philips Respironics, Inc., outside the submitted work; In addition, Dr. Parthasarathy has a patent UA 14-018 U.S.S.N. 61/884,654; PTAS 502570970 (home-breathing device) pending. The abovementioned conflicts including the patent are unrelated to the topic of this paper. Drs. Daniel Combs and James Goodwin do not have any conflicts of interest to disclose. Dr. Wayne Morgan has received grant funding from NIH and the Cystic Fibrosis Foundation, and he is a consultant to the Cystic Fibrosis Foundation and Genentech. These are all unrelated to the topic of this paper. Dr. Stuart F. Quan reports grants from the NIH/NIA, the American Diabetes Association, and the National Science Foundation, and he consults for the Global Corporate Challenge and the American Board of Internal Medicine.
The ICMJE Uniform Disclosure Form for Potential Conflicts of Interest associated with this article can be viewed by clicking on the following link: http://dx.doi.org/10.1016/j.sleep.2015.06.008.
References
- 1.Matricciani L, Olds T, Petkov J. In search of lost sleep: secular trends in the sleep time of school-aged children and adolescents. Sleep Med Rev. 2012;16:203–211. doi: 10.1016/j.smrv.2011.03.005. [DOI] [PubMed] [Google Scholar]
- 2.Mercer PW, Merritt SL, Cowell JM. Differences in reported sleep need among adolescents. J Adolesc Health. 1998;23:259–263. doi: 10.1016/s1054-139x(98)00037-8. [DOI] [PubMed] [Google Scholar]
- 3.Reilly JJ, Armstrong J, Dorosty AR, et al. Early life risk factors for obesity in childhood: cohort study. BMJ. 2005;330:1357. doi: 10.1136/bmj.38470.670903.E0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Snell EK, Adam EK, Duncan GJ. Sleep and the body mass index and overweight status of children and adolescents. Child Dev. 2007;78:309–323. doi: 10.1111/j.1467-8624.2007.00999.x. [DOI] [PubMed] [Google Scholar]
- 5.Pileggi C, Lotito F, Bianco A, Nobile CG, Pavia M. Relationship between chronic short sleep duration and childhood body mass index: a school-based cross-sectional study. PLoS ONE. 2013;8:e66680. doi: 10.1371/journal.pone.0066680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Seegers V, Petit D, Falissard B, et al. Short sleep duration and body mass index: a prospective longitudinal study in preadolescence. Am J Epidemiol. 2011;173:621–629. doi: 10.1093/aje/kwq389. [DOI] [PubMed] [Google Scholar]
- 7.Silva GE, Goodwin JL, Parthasarathy S, et al. Longitudinal association between short sleep, body weight, and emotional and learning problems in Hispanic and Caucasian children. Sleep. 2011;34:1197–1205. doi: 10.5665/SLEEP.1238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Archbold KH, Vasquez MM, Goodwin JL, Quan SF. Effects of sleep patterns and obesity on increases in blood pressure in a 5-year period: report from the Tucson Children’s Assessment of Sleep Apnea Study. J Pediatr. 2012;161:26–30. doi: 10.1016/j.jpeds.2011.12.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Perfect MM, Patel PG, Scott RE, et al. Sleep, glucose, and daytime functioning in youth with type 1 diabetes. Sleep. 2012;35:81–88. doi: 10.5665/sleep.1590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Iglayreger HB, Peterson MD, Liu D, et al. Sleep duration predicts cardiometabolic risk in obese adolescents. J Pediatr. 2014;164:1085–1090. e1. doi: 10.1016/j.jpeds.2014.01.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Beebe DW. Cognitive, behavioral, and functional consequences of inadequate sleep in children and adolescents. Pediatr Clin North Am. 2011;58:649–665. doi: 10.1016/j.pcl.2011.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Roberts RE, Roberts CR, Duong HT. Sleepless in adolescence: prospective data on sleep deprivation, health and functioning. J Adolesc. 2009;32:1045–1057. doi: 10.1016/j.adolescence.2009.03.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Titova OE, Hogenkamp PS, Jacobsson JA, Feldman I, Schioth HB, Benedict C. Associations of self-reported sleep disturbance and duration with academic failure in community-dwelling Swedish adolescents: sleep and academic performance at school. Sleep Med. 2015;16:87–93. doi: 10.1016/j.sleep.2014.09.004. [DOI] [PubMed] [Google Scholar]
- 14.Wolfson AR, Carskadon MA. Sleep schedules and daytime functioning in adolescents. Child Dev. 1998;69:875–887. [PubMed] [Google Scholar]
- 15.Pasch KE, Latimer LA, Cance JD, Moe SG, Lytle LA. Longitudinal bi-directional relationships between sleep and youth substance use. J Youth Adolesc. 2012;41:1184–1196. doi: 10.1007/s10964-012-9784-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Koulouglioti C, Cole R, Kitzman H. Inadequate sleep and unintentional injuries in young children. Public Health Nurs. 2008;25:106–114. doi: 10.1111/j.1525-1446.2008.00687.x. [DOI] [PubMed] [Google Scholar]
- 17.Fredriksen K, Rhodes J, Reddy R, Way N. Sleepless in Chicago: tracking the effects of adolescent sleep loss during the middle school years. Child Dev. 2004;75:84–95. doi: 10.1111/j.1467-8624.2004.00655.x. [DOI] [PubMed] [Google Scholar]
- 18.Sarchiapone M, Mandelli L, Carli V, et al. Hours of sleep in adolescents and its association with anxiety, emotional concerns, and suicidal ideation. Sleep Med. 2014;15:248–254. doi: 10.1016/j.sleep.2013.11.780. [DOI] [PubMed] [Google Scholar]
- 19.Services UDoHaH. Healthy people 2020 objective topic areas. Washington, DC: 2011. [Google Scholar]
- 20.Zee PC, Badr MS, Kushida C, et al. Strategic opportunities in sleep and circadian research: report of the Joint Task Force of the Sleep Research Society and American Academy of Sleep Medicine. Sleep. 2014;37:219–227. doi: 10.5665/sleep.3384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hale L, Do DP. Racial differences in self-reports of sleep duration in a population-based study. Sleep. 2007;30:1096–1103. doi: 10.1093/sleep/30.9.1096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Adenekan B, Pandey A, McKenzie S, Zizi F, Casimir GJ, Jean-Louis G. Sleep in America: role of racial/ethnic differences. Sleep Med Rev. 2013;17:255–262. doi: 10.1016/j.smrv.2012.07.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Whinnery J, Jackson N, Rattanaumpawan P, Grandner MA. Short and long sleep duration associated with race/ethnicity, sociodemographics, and socioeconomic position. Sleep. 2014;37:601–611. doi: 10.5665/sleep.3508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Spilsbury JC, Storfer-Isser A, Drotar D, et al. Sleep behavior in an urban US sample of school-aged children. Arch Pediatr Adolesc Med. 2004;158:988–994. doi: 10.1001/archpedi.158.10.988. [DOI] [PubMed] [Google Scholar]
- 25.McLaughlin Crabtree V, Beal Korhonen J, Montgomery-Downs HE, Faye Jones V, O’Brien LM, Gozal D. Cultural influences on the bedtime behaviors of young children. Sleep Med. 2005;6:319–324. doi: 10.1016/j.sleep.2005.02.001. [DOI] [PubMed] [Google Scholar]
- 26.Wu Y, Zhai L, Zhang D. Sleep duration and obesity among adults: ameta-analysis of prospective studies. Sleep Med. 2014;15:1456–1462. doi: 10.1016/j.sleep.2014.07.018. [DOI] [PubMed] [Google Scholar]
- 27.Knutson KL. Association between sleep duration and body size differs among three Hispanic groups. Am J Hum Biol. 2011;23:138–141. doi: 10.1002/ajhb.21108. [DOI] [PubMed] [Google Scholar]
- 28.Martinez SM, Tschann JM, Greenspan LC, et al. Is it time for bed? Short sleep duration increases risk of obesity in Mexican American children. Sleep Med. 2014;15:1484–1489. doi: 10.1016/j.sleep.2014.09.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Goodwin JL, Enright PL, Kaemingk KL, et al. Feasibility of using unattended polysomnography in children for research – report of the Tucson Children’s Assessment of Sleep Apnea study (TuCASA) Sleep. 2001;24:937–944. doi: 10.1093/sleep/24.8.937. [DOI] [PubMed] [Google Scholar]
- 30.Budhiraja R, Quan SF. Outcomes from the Tucson Children’s Assessment of Sleep Apnea Study (TuCASA) Sleep Med Clin. 2009;4:9–18. doi: 10.1016/j.jsmc.2008.11.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Prevention CfDCa. Clinical growth charts [Google Scholar]
- 32.DiversityData. Median household income. 2004;2004 [Google Scholar]
- 33.Sadeh A, Gruber R, Raviv A. The effects of sleep restriction and extension on school-age children: what a difference an hour makes. Child Dev. 2003;74:444–455. doi: 10.1111/1467-8624.7402008. [DOI] [PubMed] [Google Scholar]
- 34.Li S, Arguelles L, Jiang F, et al. Sleep, school performance, and a school-based intervention among school-aged children: a sleep series study in China. PLoS ONE. 2013;8:e67928. doi: 10.1371/journal.pone.0067928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Smith MR, Burgess HJ, Fogg LF, Eastman CI. Racial differences in the human endogenous circadian period. PLoS ONE. 2009;4:e6014. doi: 10.1371/journal.pone.0006014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Adolescent Sleep Working Group. Committee on Adolescence, Council on School Health. School start times for adolescents. Pediatrics. 2014;134:642–649. doi: 10.1542/peds.2014-1697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Goodwin JL, Silva GE, Kaemingk KL, Sherrill DL, Morgan WJ, Quan SF. Comparison between reported and recorded total sleep time and sleep latency in 6- to 11-year-old children: the Tucson Children’s Assessment of Sleep Apnea Study (TuCASA) Sleep Breath. 2007;11:85–92. doi: 10.1007/s11325-006-0086-6. [DOI] [PubMed] [Google Scholar]
- 38.Martinez SM, Greenspan LC, Butte NF, et al. Mother-reported sleep, accelerometer-estimated sleep and weight status in Mexican American children: sleep duration is associated with increased adiposity and risk for overweight/obese status. J Sleep Res. 2014;23:326–334. doi: 10.1111/jsr.12114. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.