

Abstract
We report on a Saudi infant with Holt-Oram syndrome caused by a de novo missense mutation of the TBX5 gene. The mutation (Thr72Lys) is novel and has not been previously reported. The cardiac and limb defects in our patient were both severe, and the infant also had micrognathia and cleft palate. Previously reported cases of the Holt-Oram syndrome caused by missense mutations were reviewed and their phenotypes were compared with the phenotype of our patient.
Holt-Oram syndrome (MIM 142900) is a rare syndrome and is characterized by congenital heart defects and radial ray deficiency in the upper limbs. The syndrome is caused by mutations of the TBX5 gene.1 Most of the reported mutations in the TBX5 gene are nonsense, frameshift or splice-site mutations, which lead to non-functional protein due to non-sense mediated decay.1 As expected, these mutations will result in severe cardiac and limb phenotypes.1 In contrast, missense mutations of the TBX5 gene are uncommon and the result is a full (non-truncated) protein with a single amino acid substitution.2-15 The phenotypes in patients with missense mutations tend to be of variable severity and frequently include non-classic features. Certain amino acid substitutions affect critical TBX5 protein interactions leading to severe phenotypes.15 Basson et al2 reviewed the phenotypes of several missense mutations of the TBX5 gene and hypothesized that the encoded TBX5 proteins will function differently in the development of the heart and the upper limb. Hence, the hypothesis of Basson et al2 stated that missense mutations of the TBX5 gene will tend to cause a severe cardiac and a concurrent mild limb phenotype or vice versa. However, recent literature3-9 disputed this hypothesis and it is now well established that such a genotype-phenotype relationship does not exist. In this paper, we report on a Saudi infant with Holt-Oram syndrome caused by a missense mutation of the TBX5 gene (c.215C>A, p. Thr72Lys). We believe that our case is important for 3 main reasons. Firstly, the mutation is novel and has not been previously reported. Secondly, our patient had severe cardiac and limb defects and such a combined severe phenotype supports the dispute raised regarding the hypothesis of Basson et al.2 Finally, our case also had micrognathia and cleft palate, which are not known to be among the classic features of Holt- Oram syndrome. The objective of this study is to describe a novel mutation of the TBX5 gene in a Saudi infant with Holt-Oram syndrome and to compare the phenotype to previously reported cases.
Case Report
A 4-month-old female infant presented to us for the treatment of bilateral radial ray deficiency. The infant had a history of complex cardiac anomaly (multiple ventricular septal defects, failure of incorporation of the pulmonary veins, and tricuspid valve insufficiency), which required cardiac surgery soon after birth. Clinical examination and electro-cardiogram showed no evidence of any conduction abnormalities. The bilateral radial ray deficiencies were also severe and were manifested as bilateral short radii with radial deviation of the wrists as well as complete absence of both thumbs (Figures 1A & 1B). The infant also had micrognathia and clefting of the soft palate. Ultrasound of the abdomen did not reveal any renal abnormalities. The parents were normal and unrelated. There was no family history of congenital anomalies of the heart or limbs.
Figure 1.

X ray of the A) left upper limb (volar view) and B) the right upper limb (dorsal view) showing a short radius (arrow) and an absent thumb.
After informed consent, genomic DNA from the parents and infant was polymerase chain reaction-amplified for analysis of the complete coding region of the TBX5 gene and their flanking splice sites. The infant was found to have a novel missense mutation of the TBX5 gene: c.215C>A, p.Thr72Lys (heterozygous). Both biological parents tested negative indicating that the mutation has arisen de novo.
Discussion
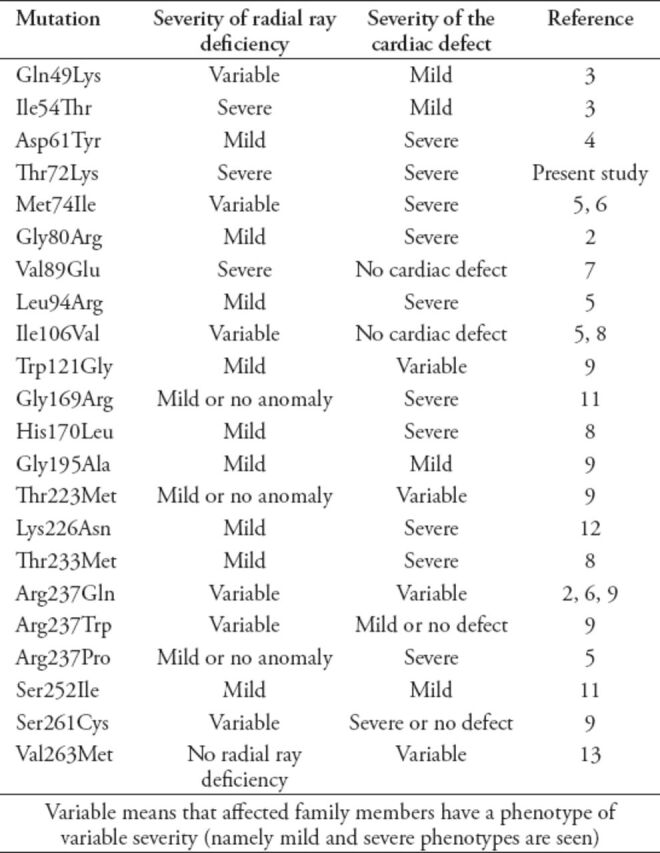
The TBX5 mutation of our patient (Thr72Lys) is novel and has not been previously reported. Although we did not perform functional analysis of the interactions of the mutant protein, this new mutation is believed to be pathogenic for several reasons. Firstly, the Thr72Lys mutation was not observed in over 6000 samples from normal subjects (NHLBI GO Exome Sequencing Project, Seattle, WA; http://evs.gs.washington.edu/EVS/). Secondly, the Thr72Lys change occurs at a highly conserved position within the DNA-binding domain of the TBX5 protein. Thirdly, missense mutations at nearby positions (Met74Ile and Gly80Arg) have been reported in association with Holt-Oram syndrome.2,5,6 Lastly, multiple in-silico analysis models predict that Thr72Lys is damaging to the TBX5 protein (as per Gene Dx, Gaithersburg, MD 20877, USA). The cardiac and limbs phenotypes were both severe. The literature2 defines the mild cardiac phenotype in Holt-Oram syndrome as an isolated septal defect, an isolated conduction defect, or an isolated valve defect. Combined defects and more complex anomalies are considered severe as seen in our patient. Similarly, the literature2 also defines completely absent thumbs (seen in our patient) as severe limb defects. The phenotype in our patient included micrognathia and clefting of the soft palate and these are not known to be among the classic features of Holt-Oram syndrome. We reviewed the literature for all reported missense mutations of the TBX5 gene, and we found 23 mutations.1-14 Two mutations (Gly125Arg and Ser372Leu) were gain-of-function mutations.10,14 The phenotype of the Gly125Arg mutation was unique and almost all affected family members had radial head dislocation and paroxysmal atrial fibrillation.10 This indicated that this gain-of-function of TBX5 activity may lead to specific cardiac and limb phenotypes.10 The second gain-of-function mutation (Ser372Leu) was maternally inherited and both mother and child had cardiac defects with normal upper limbs.14 The remaining 21 mutations were loss-of-function mutations and these are shown in Table 1. Table 1 shows that the cardiac/limb phenotypes in our patient as well as the phenotypes of several other missense mutations do not support the hypothesis of Basson et al.2 In fact, several mutations have resulted in phenotypes of variable severity in different members of the same family. Another observation from Table 1 is the absence of cardiac or limb defects in several missense mutations. This is important to note because it means that screening for TBX5 mutations may be indicated in families with isolated cardiac defects or isolated radial ray deficiency. Finally, our literature review revealed that the Ser261Cys mutation reported by Brassington et al9 was the only mutation that was associated with micrognathia and cleft palate. The phenotype in our case also included micrognathia and cleft palate indicating that these defects may be considered as part of the spectrum of the clinical features of Holt-Oram syndrome. However, our case and the case of Brassington et al9 were not subjected to other tests (such as array comparative genomic hybridization analysis and screening of known genes causing isolated cleft palate). Hence, it remains a possibility that a separate second hit is responsible for the micrognathia/cleft palate phenotype.
Table 1.
Loss-of-function missense mutations of the TBX5 gene among 21 mutations.
In conclusion, missense mutations of the TBX5 gene are uncommon and we add a novel mutation (c.215C>A, p. Thr72Lys) to the literature. After reviewing the phenotype in our patient and other cases in the literature, we also conclude that micrognathia and cleft palate may be features of the Holt-Oram phenotype.
Footnotes
References
- 1.Basson CT, Bachinsky DR, Lin RC, Levi T, Elkins JA, Soults J, et al. Mutations in human TBX5 cause limb and cadiac malformation in Holt-Oram syndrome. Nat Genet. 1997;15:30–35. doi: 10.1038/ng0197-30. [DOI] [PubMed] [Google Scholar]
- 2.Basson CT, Huang T, Lin RC, Bachinsky DR, Weremowicz S, Vaglio A, et al. Different TBX5 interactions in heart and limb defined by Holt-Oram syndrome mutations. Proc Natl Acad Sci USA. 1999;96:2919–2924. doi: 10.1073/pnas.96.6.2919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Yang J, Hu D, Xia J, Yang Y, Ying B, Hu J, et al. Three novel TBX5 mutations in Chinese patients with Holt-Oram syndrome. Am J Med Genet. 2000;92:237–240. doi: 10.1002/(sici)1096-8628(20000605)92:4<237::aid-ajmg2>3.0.co;2-g. [DOI] [PubMed] [Google Scholar]
- 4.Dias RR, Albuguergue JM, Pereira AC, Stolf NA, Krieger JE, Mady C, et al. Holt-Oram syndrome presenting as agenesis of the left pericardium. Int J Cardiol. 2007;114:98–100. doi: 10.1016/j.ijcard.2005.09.056. [DOI] [PubMed] [Google Scholar]
- 5.Boogerd CJ, Dooijes D, Llgun A, Mathijssen IB, Hordijk R, Van de Laar IM, et al. Functional analysis of novel TBX5 T-box mutations associated with Holt-Oram syndrome. Cardiovasc Res. 2010;88:130–139. doi: 10.1093/cvr/cvq178. [DOI] [PubMed] [Google Scholar]
- 6.Debeer P, Race V, Gewillig M, Devriendt K, Frijns JP. Novel TBX5 mutations in patients with Holt-Oram syndrome. Clin Orthop Relat Res. 2007;462:20–26. doi: 10.1097/BLO.0b013e3181123ffe. [DOI] [PubMed] [Google Scholar]
- 7.Furniss D, Kan SH, Taylor IB, Johnson D, Critchley PS, Giele HP, et al. Genetic screening of 202 individuals with congenital limb malformations and requiring reconstructive surgery. J Med Genet. 2009;46:730–735. doi: 10.1136/jmg.2009.066027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.McDermott DA, Bresson MC, He J, Lee JS, Aftimos S, Brueckner M, et al. TBX5 genetic testing candidates strict clinical criteria for Holt-Oram syndrome. Pediatr Res. 2005;58:981–986. doi: 10.1203/01.PDR.0000182593.95441.64. [DOI] [PubMed] [Google Scholar]
- 9.Brassington AM, Sung SS, Toydemir RM, Le T, Roeder AD, Rutherford AE, et al. Expressivity of Holt-Oram syndrome is not predicted by TBX5 genotype. Am J Hum Genet. 2003;73:74–85. doi: 10.1086/376436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Postma AV, Van de Meerakker JB, Mathijssen IB, Barnett P, Christoffels VM, Llgun A, et al. A gain-of-function TBX5 mutation is associated with atypical Holt-Oram syndrome and paroxysmal atrial fibrillation. Circ Res. 2008;102:1433–1442. doi: 10.1161/CIRCRESAHA.107.168294. [DOI] [PubMed] [Google Scholar]
- 11.Cross SJ, Ching YH, Li QY, Armstrong-Buisseret L, Spranger S, Lyonnet S, et al. The mutation spectrum in Holt-Oram syndrome. J Med Genet. 2000;37:785–787. doi: 10.1136/jmg.37.10.785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Porto MP, Vergani N, Carvalho AC, Cornach MC, Brunoni D, Perez AB. Novel mutations in the TBX5 gene in patients with Holt-Oram syndrome. Genet Mol Biol. 2010;33:232–236. doi: 10.1590/S1415-47572010005000051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Faria MH, Rabenhorst SH, Pereira AC, Krieger JE. A novel TBX5 missense mutation (V263M) in a family with atrial septal defects and postaxial hexadactyly. Int J Cardiol. 2008;130:30–35. doi: 10.1016/j.ijcard.2008.06.090. [DOI] [PubMed] [Google Scholar]
- 14.Baban A, Postma AV, Marini M, Trocchio G, Santilli A, Pelegrini M, et al. Identification of TBX5 mutations in a series of 94 patients with tetralogy of Fallot. Am J Med Genet A. 2014;164:3100–3107. doi: 10.1002/ajmg.a.36783. [DOI] [PubMed] [Google Scholar]
- 15.Barnett P, Postma AV. Molecular genetics of Holt Oram syndrome. [Updated 2014; 2015 March 15]. Available from URL:http://www.els.net . [doi: 10.1002/9780470015902.a0024329]