

Abstract
Obstructive sleep apnoea (OSA) is a common disorder characterized by repetitive episodes of nocturnal breathing cessation due to upper airway collapse. OSA causes severe symptoms, such as excessive daytime somnolence, and is associated with a significant cardiovascular morbidity and mortality. Different treatment options are now available for an effective management of this disease. After more than three decades from its first use, continuous positive airway pressure (CPAP) is still recognized as the gold standard treatment. Nasal CPAP (nCPAP) is highly effective in controlling symptoms, improving quality of life and reducing the clinical sequelae of sleep apnoea. Other positive airway pressure modalities are available for patients intolerant to CPAP or requiring high levels of positive pressure. Mandibular advancement devices, particularly if custom made, are effective in mild to moderate OSA and provide a viable alternative for patients intolerant to CPAP therapy. The role of surgery remains controversial. Uvulopalatopharyngoplasty is a well established procedure and can be considered when treatment with CPAP has failed, whereas maxillar-mandibular surgery can be suggested to patients with a craniofacial malformation. A number of minimally invasive procedures to treat snoring are currently under evaluation. Weight loss improves symptoms and morbidity in all patients with obesity and bariatric surgery is an option in severe obesity. A multidisciplinary approach is necessary for an accurate management of the disease.
Keywords: continuous positive airway pressure, obstructive sleep apnoea, oral appliance, positional therapy, uvulopalatopharyngoplasty
Introduction
Obstructive sleep apnoea (OSA) is a common chronic disorder affecting about 2–4% of the adult population, with the highest prevalence reported among middle-aged men [Young et al. 1993]. The condition is characterized by repetitive episodes of complete or partial collapse of the upper airway (mainly the oropharyngeal tract) during sleep, with a consequent cessation/reduction of the airflow [Guilleminault et al. 1976; Guilleminault and Quo, 2001]. The obstructive events (apnoeas or hypopnoeas) cause a progressive asphyxia that increasingly stimulates breathing efforts against the collapsed airway, typically until the person is awakened (Figure 1).
Figure 1.
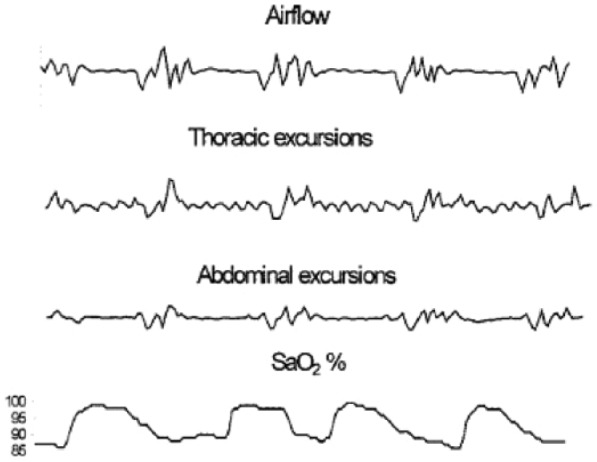
Polygraphic recording of an obstructive apnoea. Interruption of nasal airflow in the presence of thoracic and abdominal movements. Below, oscillations of oxygen saturation (SaO2).
The diagnosis of OSA is made through different levels of nocturnal monitoring of respiratory, sleep and cardiac parameters (polisomnography or nocturnal cardio-respiratory poligraphy), aimed to detect the obstructive events and the following changes in blood oxygen saturation (SaO2) [Berry et al. 2012; American Academy of Sleep Medicine, 2014]. The most commonly used index to define the severity of OSA is the apnoea/hypopnoea index (AHI), calculated as the number of obstructive events per hour of sleep and obtained by nocturnal cardiorespiratory monitoring [Berry et al. 2012] (Table 1). The aetiology of OSA is multifactorial, consisting of a complex interplay between anatomic, neuromuscular factors and an underlying genetic predisposition toward the disease [Guilleminault and Quo, 2001; Dempsey et al. 2010]. Risk factors include snoring, male gender, middle age, menopause in women, obesity and a variety of craniofacial and oropharyngeal features such as a large neck circumference, retro- or micrognazia, nasal obstruction, enlarged tonsils/adenoids, macroglossia and low-lying soft palate [Guilleminault and Quo, 2001; Dempsey et al. 2010]. Over the years, recurrent episodes of apnoeas, intermittent hypoxia and sleep fragmentation affect the function of different organs and systems, mainly the brain and the cardiovascular system, and alter the body metabolic balance [Guilleminault and Quo, 2001; Bradley et al. 2009]. This leads to a variety of clinical sequelae accepted as the OSA syndrome. Daytime sleepiness, due to nocturnal sleep fragmentation, is a key symptom of OSA, being present in more than 80% of the patients. As the disorder progresses, the sleepiness becomes increasingly dangerous, causing impaired performance at work and major work-related and road accidents [Guilleminault and Quo, 2001; Jordan et al. 2014]. Moreover, many patients can develop cognitive and neurobehavioral dysfunction, inability to concentrate, memory impairment and mood changes such as irritability and depression. This further impairs performance at work with a remarkable effect on the quality of life [Vaessen et al. 2014] (Table 2). It is now well established that, if untreated, OSA is a major determinant of cardiovascular morbidity and mortality [Bradley et al. 2009; Young et al. 2008]. The main cardiovascular disorders described include drug-resistant systemic hypertension (>50% of the patients), ischemic heart disease, cardiac arrhythmias and stroke [Bradley et al. 2008]. Recently, sleep-related hypoxia has also been associated with a low-grade systemic inflammation, which in turn may contribute to initiate or accelerate the process of atherogenesis [Jordan et al. 2014]. In addition, an important metabolic impairment occurs in OSA independently from the body weight. Insulin resistance, type II diabetes and altered serum lipid profile, widely described in patients with OSA, can represent a further risk of cardiovascular morbidity [Sharma et al. 2011; Jordan et al. 2014]. There is now little doubt that an increased mortality occurs in patients with untreated sleep apnoea compared with healthy controls [Marin et al. 2005; Young et al. 2008; Kendzerska et al. 2014] (Figure 2).
Table 1.
The severity of obstructive sleep apnea (OSA) based on the apnea hypopnoea index (AHI).
| OSA severity | |
|---|---|
| AHI < 5 | Normal or primary snoring |
| 5 < AHI < 20 | Mild |
| 20 < AHI < 40 | Moderate |
| AHI > 40 | Severe |
Table 2.
Most common symptoms associated with obstructive sleep apnea.
| Nocturnal | Diurnal |
|---|---|
| Snoring | Excessive sleepiness |
| Witnessed apnoeas | Morning headaches |
| Choking at night | Depression/irritability |
| Nicturia | Memory loss |
| Insomnia | Decreased libido |
Figure 2.

Survival curves (unadjusted Kaplan–Meier) by obstructive sleep apnoea severity as expressed by the apnoea hypopnoea index (AHI). The numbers at risk are presented above the x axis. From the study by Kendzerska et al. [2014].
In the last two decades, advances in sleep medicine and the availability of improved diagnostic tools have led to a better recognition and treatment of the disease. The management of patients with OSA requires a multidisciplinary approach and many treatment options are currently available. Positive airway pressure (PAP), available since the beginning of the 1980s, provides the most effective and commonly used treatment. Alternative options include weight control, mandibular advancement devices and a number of upper airway surgical approaches.
In this article, we will review the indication, the efficacy and the role in the clinical practice of each treatment option available for the management of OSA.
Positive airway pressure treatment
The elimination of nocturnal apnoeic events and intermittent hypoxia is a key goal to controlling OSA effectively. PAP devices function as a pneumatic support that allows one to maintain upper airway patency by increasing the upper airway pressure above a ‘critical’ value (pressure value below which the airways collapse). The device is applied to the patient, through a nasal or oronasal mask, overnight or during sleep hours at a set positive pressure. The pressure to apply can vary with the severity of OSA and higher pressures are needed to abolish those apnoeas occurring during rapid eye movement sleep, in the supine position or in the presence of severe obesity. For each patient, the effective pressure is obtained after one or more nights of PAP titration. PAP therapy is indicated in all patients with an AHI greater than 15, independently from the presence of comorbidities, type of work and severity of symptoms; if the AHI is above 5 and below 15, PAP is indicated in the presence of symptoms (i.e. sleepiness, impaired cognition, mood disorders) or in the presence of hypertension, coronary artery disease or previous cerebrovascular accidents [Epstein et al. 2009] (Figure 3). As PAP therapy is, in most cases, a life-long treatment, in the last 10 years many different models of PAP home ventilators have been commercialized in order to guarantee efficacy and maximal comfort for patients. In addition, different modalities of PAP ventilation are now available to meet patients’ different and specific needs. If interested in more specific and technical details on PAP home ventilators, I suggest to our readers a detailed review from Dr Stasche (2006).
Figure 3.
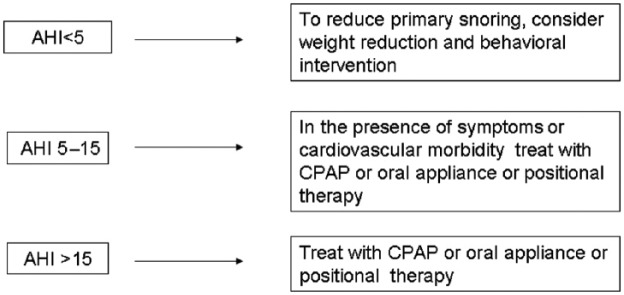
Indications for the management of obstructive sleep apnoea based on the apnoea hypopnoea index (AHI). Continuous positive airway pressure (CPAP) should be considered as the first choice of treatment, whereas positional treatment is indicated only when positional apnoeas have been documented.
Continuous positive airway pressure
Continuous PAP (CPAP), generally administered through the nose (nCPAP), is undoubtedly considered the gold standard treatment for OSA. Since its invention in 1983 by Dr Sullivan, the clinical application of this device has deeply modified the course of the disease over the last three decades, offering to thousands of patients the first noninvasive method to control their disorder [Sullivan et al. 1983]. Worldwide, nCPAP is constantly recommended as the first-choice treatment for patients with moderate to severe OSA [Stasche, 2006; Epstein et al. 2009].
It has been consistently shown that, compared with placebo, CPAP reduces the number of nocturnal obstructive events (decrease in AHI to normal or nearly normal values) and the number of nocturnal arousals, improving sleep parameters and nocturnal SaO2 from the first night of treatment. All daytime symptoms, particularly sleepiness, and nocturnal symptoms are, after a short period of constant use, reversed by CPAP [Patel et al. 2003; Stasche, 2006]. According to some reports, treatment with CPAP can also help patients with neurocognitive impairment. In fact, after 3–6 months of constant treatment, patients experience an improvement in their memory, attention and executive function [Aloia et al. 2003; Zimmerman et al. 2006]. Although the magnitude and the precise timing of neurocognitive changes induced by CPAP still remain controversial [Kielb et al. 2012], there is little doubt that a constant nocturnal treatment (at least 5 h) with CPAP produces a dramatic improvement in the quality of life of the patients and, in many cases, of their bed partners [Patel et al. 2003; Stasche, 2006]. Untreated patients with OSA and daytime somnolence are at increased risk of motor vehicle accidents. Different studies have tried to address the issue of whether or not patients treated with CPAP may drive safely. It has been documented that there is a significant improvement in simulated driving performance of patients within 2–7 days of CPAP use [Antonopoulos et al. 2011]. This effect, documented in a virtual environment, is also observable in real life, as CPAP treatment has a sizeable protective effect on road traffic accidents. A meta-analysis including nine observational studies examining crash risk of drivers with OSA before and after treatment with CPAP found a significant risk reduction following treatment [Tregear et al. 2010]. The need to assess the fitness to drive, particularly in patients operating commercial vehicles, is constantly stressed in guidelines to clinicians dealing with sleep disorders. A constant verification of adherence to treatment is also highly recommended when managing these patients.
Some studies have shown a significant independent association between OSA, hypertension, coronary artery disease and stroke; persuasive data provide evidence that treatment with CPAP has a positive impact on cardiovascular outcomes [Marin et al. 2005; Bradley and Floras, 2009].
A large meta-analysis on 32 studies, including a total of 1948 patients, has shown that PAP treatment is associated with a modest but significant reduction in diurnal and nocturnal systolic and diastolic blood pressure [Montesi et al. 2012]. Another recent meta-analysis systematically analyzed six studies addressing the effect of CPAP on diurnal blood pressure in patients with OSA and drug-resistant hypertension and found a favourable reduction after treatment with CPAP [Iftikhar et al. 2014]. In this study the effect sizes were larger compared with those previously reported in patients without resistant hypertension, suggesting a direct effect of the obstructive events in the pathogenesis of hypertension. The protective effect of CPAP on cardiovascular accidents has been largely documented. In the largest observational study available, patients with untreated severe OSA had a higher incidence of fatal and nonfatal cardiovascular events than patients treated with CPAP and healthy participants [Marin et al. 2005]. Another study has shown that in patients with OSA and known coronary artery disease treatment with CPAP protected against new cardiovascular accidents (defined as cardiovascular death, acute coronary syndrome, hospitalization for heart failure or need for coronary revascularization) over a 5-year observational period [Milleron et al. 2004]. Insulin resistance and altered serum lipid profile have been strictly associated with OSA. Although the effect of CPAP on metabolic changes has been widely explored in the last 10 years, results are still inconclusive. While some studies have shown that treatment with CPAP rapidly improves insulin sensitivity [Dorkova et al. 2008; Chen et al. 2014], other authors did not confirm this finding [Sharma et al. 2011; Jullian-Desayes et al. 2014]. It is likely that in patients without obesity OSA is the only cause of insulin resistance that can be rapidly reversed by the treatment; however, in patients with obesity and OSA insulin resistance is more closely associated with obesity and therefore more difficult to reverse simply by CPAP treatment. Indeed, the association of CPAP and weight loss provides the best approach to improve glucose metabolism in patients with obesity and OSA [Chirinos et al. 2014]. A large, authoritative study reported that in patients with moderate to severe OSA, 3 months of treatment with CPAP compared with sham CPAP, produced a significant decrease in serum total cholesterol (non-high-density lipoprotein cholesterol and low-density lipoprotein cholesterol) and triglycerides [Sharma et al. 2011]. The improvement in serum lipid profile by CPAP treatment has been confirmed by two recent extensive meta-analyses [Nadeem et al. 2014]. The OSA syndrome has also been associated with a low-grade systemic inflammation, evidenced by high serum levels of mediators of the systemic and vascular inflammatory response, including cell adhesion molecules, coagulation factors, C-reactive protein (CRP) and inflammatory cytokines. The ongoing inflammatory responses give a substantial contribution to the atherosclerosis process, thus increasing the cardiovascular and cerebrovascular morbidity. Although definitive data are still lacking, a meta-analysis confirmed that treatment with CPAP reduces serum levels of some inflammatory markers such as CRP, tumour necrosis factor α and interleukin 6 [Baessler et al. 2013].
Taken together these data indicate that CPAP is extremely effective in controlling symptoms and consequences of OSA and very few side effects (mainly mask or pressure-related discomfort and nasal congestion) have been reported. However, it is important to note that the efficacy of CPAP strictly depends on its constant use and that a recurrence of symptoms occurs after 1–3 days from treatment interruption. Therefore, in the absence of any other intervention, CPAP will represent a lifetime treatment. In addition, not all patients with OSA tolerate CPAP. Some patients complain about discomfort when breathing through a mask with a positive pressure applied, while other patients do not accept sleeping the whole night attached to a mechanical device. Whatever is the reason for scarce tolerance, adherence to the treatment represents a major issue as compliance with CPAP has been reported to be from 50% to 80% of patients [Jordan et al. 2014].
Other and newer modalities of positive airway pressure ventilation
Some patients have trouble in breathing during the application of positive pressure, particularly in exhaling against a high pressure. For some patients high levels of pressure are required to control apnoeas and it can be difficult to tolerate such high pressures in a continuous mode. Therefore, different modalities of PAP ventilation have been utilized to treat OSA.
Bilevel PAP ventilation provides two different levels of pressure (higher during inhalation and lower during expiration) and can potentially treat OSA at a lower mean pressure than CPAP, at the same time improving lung ventilation via a pressure support. Bilevel PAP, although more expensive than CPAP, is therefore a valid alternative in patients intolerant to CPAP and in patients with associated hypoventilation or chronic obstructive pulmonary disease [Kolla et al. 2014]. In patients with OSA, severe obesity and impaired awake blood gas values are the main factors predicting CPAP failure. In these patients, adequate control of OSA and an improvement in awake blood gas values can be obtained using bilevel PAP [Schäfer et al. 1998]. Treatment with bilevel PAP is also preferred in patients with severe OSA and in those requiring high treatment pressures [Kolla et al. 2014].
Autotitrating CPAP (Auto-CPAP) is a more sophisticated device providing an alternative to traditional CPAP. While CPAP delivers a continuous fixed pressure during the entire treatment session, Auto-CPAP automatically and continuously adjusts the delivered pressure (within a maximal and minimal value, set by the operator) in order to maintain upper airway patency following changes in airflow resistance [Stasche, 2006]. Such changes depend on factors such as the posture, the degree of nasal congestion or the sleep stage. Varying the delivered pressure, using specific algorithms, improves the breathing synchrony with the device and improves the patient’s comfort. Compliance with Auto-CPAP is slightly higher compared with fixed CPAP [Smith and Lasserson, 2009], whereas the two modalities produce similar benefits in terms of diurnal symptoms and sleep measures [Stanley et al. 2012]. Therefore, the prescription of one of these devices will depend on patient’s preference, costs, local reimbursement policy and other practical factors.
Alternatives to PAP
Positional therapy
Due to anatomical and physiological mechanisms, the body position during sleep influences the frequency and the severity of the obstructive events. The supine position, mainly due to the effect of the gravity on tongue and soft palate position, is generally associated with an increased number of apnoeas/hypopnoeas [Bidarian-Moniri et al. 2015]. Postural OSA is diagnosed when the obstructive events take place exclusively or mainly in the supine posture (the AHI in the supine position is at least double with respect to the nonsupine position) and it occurs approximately in 30% of the patients with OSA [Frank et al. 2015]. Retrospective studies indicate that patients with positional OSA have a milder AHI and are generally younger with less obesity [Oksenberg, 2005; Frank et al. 2015]. If postural OSA is diagnosed according to standard criteria, patients can benefit from a positional therapy (PT), which should prevent them from sleeping in the supine posture. Many PT strategies are available. These include the simple ‘tennis ball technique’, consisting of a tennis ball strapped to the back to discourage supine position, supine alarm devices and a number of positional pillows [Oksenberg, 2005; Frank et al. 2015]. All these strategies accurately improve OSA, without any evidence of one being more effective over the others. The therapy is considered successful when the post-treatment AHI is below 10, and this goal is generally achieved when a correct selection of the candidates is done. Although PT is a better accepted therapy, it is important to outline that the clinical benefits of this treatment remain inferior to treatment with CPAP. In addition, studies assessing the long-term effects of PT on important outcomes, such as metabolic and neurocognitive changes, are still lacking [Frank et al. 2015].
Oral appliances
Over the last 10 years, oral appliances have gained increasing recognition as a useful alternative to CPAP for the treatment of patients with mild to moderate OSA and for those patients with severe disease intolerant to CPAP [Ngiam et al. 2013]. The most commonly used oral appliances are mandibular advanced splints (MAS). These devices attach to both the upper and lower dental arches in order to advance and retain the mandible in a forward position. This will relocate laterally the pharyngeal fat pads from the airway and the tongue base will move forward. Consequently, the upper airway will be widened, particularly in its lateral dimension, and the function of upper airway dilator muscles, particularly the genioglossus, will improve [Chan et al. 2010]. As the pharyngeal collapsibility is reduced, the risk of apnoeic events will be lowered. Treatment with MAS is safe, producing common, but transitory and very mild, side effects such as excessive salivation, dry mouth and gingivae irritation. Side effects that are more persistent include arthralgia, teeth pain and occlusal changes [Marklund et al. 2001; Cistulli et al. 2004]. Better outcomes and a better compliance have been obtained with custom-made devices [Vanderveken et al. 2008].
Several randomized trials have evaluated the efficacy of MAS versus either placebo or CPAP. In patients with mild to moderate sleep apnoea, compared with placebo, treatment with MAS significantly reduces the number of apnoeas/hypopnoeas (normalizing nocturnal SaO2), reduces daytime somnolence, and improves neurocognitive impairment and quality of life [Cistulli et al. 2004; Health Quality Ontario, 2009]. Treatment with MAS has a favourable effect on blood pressure control, determining a significant reduction in both the nocturnal and the diurnal blood pressure values [Gotsopoulos et al. 2004; Sutherland et al. 2014]. However, there is general agreement that all these effects are milder compared with treatment with CPAP. In addition, the long-term effect of treatment with oral devices on cardiovascular health and all other health outcomes is still uncertain [Sutherland et al. 2014].
Although MAS have been proposed as a viable alternative to patients with mild to moderate OSA intolerant to CPAP, data on compliance are controversial. Some reports indicate that generally patients prefer MAS to CPAP [Ferguson et al. 2006], while other studies report a similar preference or more preference for CPAP [Sutherland et al. 2014]. The rate of suspension after 1 year fluctuates from 10% to 25% of the patients treated with MAS and data on long-term compliance are still scarce [Dieltjens et al. 2013]. Indeed, as for other treatments, correct selection of patients is also important for MAS in order to achieve success. Although a good success rate has been reported after accurate selection of the candidates, it has to be mentioned that up to one-third of the patients are unresponsive to MAS. Factors predicting the response to treatment are still unclear. Generally, treatment success is achieved in younger, female patients without obesity and in nonpositional and milder OSA [Mehta et al. 2001]. In addition, some cephalometric and physiologic upper airway variables (i.e. low nasal resistance at rhinometry) predict the response to MAS [Liu et al. 2001; Zeng et al. 2008]. Patients requiring high CPAP pressures (>13 cm H2O) to eliminate apnoeas will not respond to MAS. It is noteworthy that one single night of titration is useful to predict the efficacy of MAS [Pételle et al. 2002]. Of course, MAS candidates also require sufficient healthy teeth and alveolar ridge, absence of temporomandibular disorders and a valid mandibular protrusion. Therefore, a multidisciplinary approach is fundamental and, after the diagnosis of OSA is made, a collaboration between dentists and sleep physicians is required in order to establish the indication for MAS, the choice of the best device and the titration procedure.
Another group of oral appliances include the tongue-retaining devices. These are newer devices designed to produce a gentle suction of the tongue into an anterior bulb in order to move the tongue forward and to increase the upper airway dimension during sleep. Overnight application of these devices significantly reduces the AHI and one study has shown similar efficacy compared with MAS. Although promising, there is still insufficient evidence to recommend the use of these oral appliances in clinical practice [Randerath et al. 2011].
Surgical treatment
The role of surgery in management of OSA has been widely explored in an attempt to find a treatment option that could be definitive. However, its role remains extremely controversial. The aim of the surgery is to remove the cause of upper airway obstruction and to widen the airway, after a precise detection of the site where the obstruction occurs. The most common sites of obstruction are the oropharyngeal tract (collapse of the retropalatal and retrolingual regions due to macroglossia, low-lying soft palate or enlarged tonsils) and the nose (congestion, polyposis, chronic rhinitis) [Dempsey et al. 2010]. As airway obstruction can occur at different sites, diverse levels of surgery exist, including minimal invasive techniques (under local anaesthesia as an outpatient procedure) and more invasive procedures. Surgery is currently performed at the level of the nose, oropharynx tract, tongue and craniofacial structures.
Although early reports underlined the relevance of nose obstruction as a cause of obstructive apnoeas, successively it has been clarified that the nose rarely has a major impact on obstructive apnoeas [Michels et al. 2014]. However, if nasal obstruction is documented, surgery (correction of the deviated septum, correction of the inferior turbinate and polypectomy) can be fundamental to help the patient to better tolerate nCPAP. Tonsillectomy and adenoidectomy are the most commonly used surgical procedures to treat OSA in children and are highly effective [Spicuzza et al. 2009].
Patients with OSA generally have excessive tissue in the oropharyngeal tract. Uvulo-palatopharyngoplasty (UPPP), either conventional or laser assisted (LAPP), is a widely established surgical procedure for the treatment of OSA in selected patients. This technique consists of the resection of uvula, part of the soft palate and tissue excess in the oropharynx, and is usually performed with simultaneous tonsillectomy [Aurora et al. 2010; Holty and Guilleminault, 2010]. UPPP significantly improves snoring, AHI, sleep measures and symptoms [Lojander et al. 1996; Verse and Hörmann, 2011]. The success rate for UPPP is highly variable, ranging from 30%, if performed alone, to 60% if performed with tonsillectomy. One major problem is that the efficacy of UPPP significantly decreases over the years; in addition, long-term relevant side effects have been described in 20–30% of patients. The most common long-term complications of UPPP include velopharyngeal insufficiency (up to one-third of patients), dry throat and swallowing difficulty [Verse and Hörmann, 2011]. All patients undergoing UPPP should be warned that the occurrence of these side effects, particularly velopharyngeal insufficiency, might preclude the tolerability and the response to a putative future treatment with CPAP; in fact, in many patients treated with UPPP higher pressure will be necessary to compensate air leakage [Bloch, 2006]. The radiofrequency ablation of the palate (RFA) is a less invasive alternative to UPPP, consisting of submucosal scarring of the soft palate in order to produce its stiffening [Carroll et al. 2012]. This will improve snoring, but still convincing evidence for improving OSA is lacking. Stiffening of the soft palate to reduce snoring and apnoeas can also be obtained by the insertion of polyester implants in the soft palate (pillar palatal implants), but again good evidence for treating patients with OSA is lacking [Gillespie et al. 2011]. The retroglossal region is another common site of obstruction. A small number of studies have shown that procedures on the tongue base, such as partial resection of the tongue and suspension, can improve AHI, symptoms and quality of life in groups of selected patients. As a standalone procedure, its success rate is only 36.6% and the procedure should be included in a multilevel surgical approach for selected patients [Handler et al. 2014].
Maxillomandibular advancement (MMA) is obtained by osteotomy of the maxilla and mandibular. The advancement of the skeleton structures passively induces an anterior displacement of the soft palate and the tongue with a simultaneous widening of the pharyngeal space [Prinsell, 2002]. MMS is indeed a highly effective treatment. Overall, after MMS, a mean reduction in AHI of 87% has been reported and there is general consensus that this represents the most effective surgical approach after tracheotomy [Prinsell, 2002; Randerath et al. 2011]. However, it is noteworthy that MMS is an extremely invasive treatment, often associated with complications and aesthetic sequelae. Therefore, the treatment should be reserved for selected patients when all other approaches and first-level surgery have failed or patients with established craniofacial malformations [Epstein et al. 2009]. Finally, tracheotomy is the most effective surgical treatment for OSA and must be reserved exclusively for patients with severe OSA whose life is at risk and for whom all other treatment approaches have failed [Epstein et al. 2009]. It is important to note that after all surgical treatments, short- and long-term follow-up is mandatory. In fact, the efficacy of most treatments decreases with age and with weight gain. This represents a major factor determining the recurrence of OSA after surgery.
Weight control and bariatric surgery
Obesity is an important risk factor for OSA and over 70% of patients with OSA have obesity; a strict correlation has been documented between body mass index (BMI) and AHI. Weight loss is therefore a main goal in the management OSA and all patients should be encouraged to control their weight [Tuomilehto et al. 2013]. Unfortunately, most of the diet programs often fail, also because OSA per se determines some metabolic changes that can preclude weight loss. In patients with severe obesity (BMI > 40) bariatric surgery, including gastric bypass and bandage, is a modality of weight reduction when conservative treatments have failed [Sarkhosh et al. 2013]. Bariatric surgery can resolve or improve OSA. A recent meta-analysis concluded that both bariatric surgery and nonsurgical weight loss have significant beneficial effects on OSA, through a reduction in BMI and AHI; however, bariatric surgery offers a significantly greater improvement than nonsurgical alternatives [Ashrafian et al. 2015]
Educational and behavioural intervention
Educational and behavioural interventions represent the first step in approaching patients with OSA, independently from the treatment chosen. Patients should be instructed to avoid risk factors such as smoking, drinking alcohol (particularly in the evening), using sedatives and hypnotics. For the physician it is a priority to explain to patients the role that obesity plays in their disorder, and to provide advice in order to maintain an optimal weight. Intensive lifestyle interventions are effective in the management of OSA, resulting in significant weight loss and a reduction in sleep apnoea severity [Mitchell et al. 2014]. Another goal of the educational approach is to help each patient to recognize the need for regular use of nocturnal CPAP. Recent data suggest that a supportive intervention can significantly increase compliance in patients with moderate to severe OSA [Wozniak et al. 2014].
Emerging therapeutic options
A number of novel treatment alternatives to nCPAP are now under evaluation for the management of patients with OSA. Although none of these can currently be recommended for clinical use, some appear promising.
The stimulation of upper airway muscles has been considered over the years as a potential approach to prevent obstructive apnoeas [Dedhia et al. 2014]. Animal and human studies have shown that the electrical stimulation of the hypoglossal nerve, activating the genioglossus muscle, increases upper airway patency [Kezirian et al. 2010]. While this physiological concept has been known for a long time, only in recent years have some stimulation devices, suitable for clinical use, been developed. The stimulator device is implanted under the chest skin with an electrode placed on the hypoglossal nerve and is activated during sleep time. The Inspire Upper Airway Stimulation (Inspire Medical Systems Inc. Maple Grove, USA) is the first system recently approved by the US Food and Drug Administration for a subset of patients with moderate to severe OSA, who are unable to use CPAP.In a large multicentre trial conducted on 126 patients with moderate to severe OSA intolerant to CPAP, overnight treatment with the stimulator produced a 68% reduction in the median AHI score with a subjective improvement in daytime sleepiness and quality of life over a period of 12 months [Strollo et al. 2014]. The treatment was well tolerated and associated with few adverse events (mainly tongue weakness and soreness). While this is an extremely promising approach which combines a surgical technique with a medical device, more evidence on long-term outcomes is still required [Dedhia et al. 2014].
Other emerging treatment options are intended for patients with mild disease or as a remedy for simple snoring. Among these options nasal expiratory PAP (nEPAP) has recently gained attention [Freedman, 2014]. The nEPAP is a disposable adhesive device placed over each nostril in order to increase the airflow resistance during the exhalation with a consequent improvement in the upper airway patency. In patients with mild to moderate OSA, nEPAP (Provent, Theravent Inc., San Jose, USA) significantly reduces snoring and the AHI score and improves subjective daytime sleepiness with an excellent adherence after 12 months of treatment [Kryger et al. 2011]. Although this is a very well tolerated treatment, the efficacy in patients with moderate to severe OSA is controversial [Rossi et al. 2013], and not enough data are currently available to include nEPAP among recommended treatment options [Freedman, 2014].
Oral negative pressure is another novel treatment modality alternative to positive pressure. The most studied negative pressure system (Winx Sleep Therapy System, ApniCure, Redwood City, USA) consists of an oral interface, a vacuum pump and a connection tube. The application of a negative pressure by the vacuum pump produces a displacement of the tongue and the soft palate in a more anterior position, thus stabilizing the upper airway. The application of this device is well tolerated and significantly reduces the number of nocturnal apnoeas. However, a multicentre study has shown that a reduction in the AHI score below 10 (which should be the goal of the treatment) is achieved only in one-third of patients [Freedman, 2014]. Therefore further research is necessary to assess the potential benefits of this evolving technology.
Conclusion
The aetiology of OSA is multifactorial, consisting of a complex interplay between anatomic and neuromuscular factors, causing upper airway collapsibility. More recently it has been pointed out that there are other physiological factors (i.e. the respiratory arousal threshold, the loop gain, the effect of aging on airway collapsibility) ultimately determining the occurrence of the disease. Therefore new subgroups of patients with different phenotypes are now defined based on several pathophysiologic traits and this may be an important step in order to choose a precise management approach.
Different treatment options are now available for effective management of OSA (Figure 4). CPAP is highly effective in controlling symptoms, improving quality of life and reducing the clinical consequences of sleep apnoea and we must consider it as a first-line option. Bilevel PAP and Auto-CPAP can be used in those patients intolerant to CPAP or when high treatment pressures are necessary. Mandibular advancement devices can be offered as a viable alternative to patients with mild to moderate OSA, intolerant to PAP. The role of surgery remains controversial. Tonsillectomy and adenoidectomy are useful in children and in adults with enlarged tonsils. Uvulopalatopharyngoplasty is a well established procedure to be considered as a second-line option when PAP has failed. Maxillar mandibular surgery is extremely effective and can be suggested to patients with craniofacial malformations. All patients with obesity should be encouraged to lose weight and bariatric surgery can be considered in patients with BMI over 40. A multidisciplinary approach and the implementation of educational programs will significantly improve the management of the disease.
Figure 4.

Treatment options for obstructive sleep apnoea. Reproduced with kind permission of Bloch [2006].
Footnotes
Funding: There was no financial support to this publication.
Conflict of interest statement: The authors have no conflict of interest to disclose
Contributor Information
Lucia Spicuzza, UO Pneumologia, Azienda Policlinico, Via Santa Sofia 187, 95123 Catania, Italy.
Daniela Caruso, Respiratory Unit, AOU Policlinico, University of Catania, Catania, Italy.
Giuseppe Di Maria, Respiratory Unit, AOU Policlinico, University of Catania, Catania, Italy.
References
- Aloia M., Ilniczky N., Di Dio P., Perlis M., Greenblatt D., Giles D. (2003) Neuropsychological change and treatment compliance in older adults with sleep apnea. J Psychosom Res 54: 71–76. [DOI] [PubMed] [Google Scholar]
- American Academy of Sleep Medicine (2014) International Classification of Sleep Disorders, 3rd edition. Darien, IL: American Academy of Sleep Medicine. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Antonopoulos C., Sergentanis T., Daskalopoulou S., Petridou E. (2011) Nasal continuous positive airway pressure (nCPAP) treatment for obstructive sleep apnea, road traffic accidents and driving simulator performance: a meta-analysis. Sleep Med Rev 15: 301–310. [DOI] [PubMed] [Google Scholar]
- Ashrafian H., Toma T., Rowland S., Harling L., Tan A., Efthimiou E., et al. (2015) Bariatric surgery or non-surgical weight loss for obstructive sleep apnoea? A systematic review and comparison of meta-analyses. Obes Surg 25: 1239–50. Available at: http://www.ncbi.nlm.nih.gov/pubmed/25537297 [DOI] [PubMed] [Google Scholar]
- Aurora R., Casey K., Kristo D., Auerbach S., Bista S., Chowdhuri S., et al. (2010) Practice parameters for the surgical modifications of the upper airway for obstructive sleep apnea in adults. Sleep 33: 1408–1413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baessler A., Nadeem R., Harvey M., Madbouly E., Younus A., Sajid H., et al. (2013) Treatment for sleep apnea by continuous positive airway pressure improves levels of inflammatory markers – a meta-analysis. J Inflamm (Lond) 10: 13–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berry R., Budhiraja R., Gottlieb D., Gozal D., Iber C., Kapur V., et al. (2012) Rules for scoring respiratory events in sleep: update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. J Clin Sleep Med 8: 597–619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bidarian-Moniri A., Nilsson M., Rasmusson L., Attia J., Ejnell H. (2015) The effect of the prone sleeping position on obstructive sleep apnoea. Acta Otolaryngol 135: 79–84. [DOI] [PubMed] [Google Scholar]
- Bloch K. (2006) Alternatives to CPAP in the treatment of the obstructive sleep apnea syndrome. Swiss Med Wkly 136: 261–267. [DOI] [PubMed] [Google Scholar]
- Bradley T., Floras J. (2009) Obstructive sleep apnoea and its cardiovascular consequences. Lancet 373: 82–93. [DOI] [PubMed] [Google Scholar]
- Carroll W., Wilhoit C., Intaphan J., Nguyen S., Gillespie M. (2012) Snoring management with nasal surgery and upper airway radiofrequency ablation. Otolaryngol Head Neck Surg 146: 1023–1027. [DOI] [PubMed] [Google Scholar]
- Chan A., Sutherland K., Schwab R., Zeng B., Petocz P., Lee R., et al. (2010) The effect of mandibular advancement on upper airway structure in obstructive sleep apnoea. Thorax 65: 726–732. [DOI] [PubMed] [Google Scholar]
- Chen L., Pei J., Chen H. (2014) Effects of continuous positive airway pressure treatment on glycaemic control and insulin sensitivity in patients with obstructive sleep apnoea and type 2 diabetes: a meta-analysis. Arch Med Sci 10: 637–642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chirinos J., Gurubhagavatula I., Teff K., Rader D., Wadden T., Townsend R., et al. (2014) CPAP, weight loss, or both for obstructive sleep apnea. N Engl J Med 370: 2265–2275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cistulli P., Gotsopoulos H., Marklund M., Lowe A. (2004) Treatment of snoring and obstructive sleep apnea with mandibular repositioning appliances. Sleep Med Rev 8: 443–446. [DOI] [PubMed] [Google Scholar]
- Dedhia R., Strollo P., Jr, Soose R. (2014) Upper airway stimulation for obstructive sleep apnea: past, present, and future. Sleep 38: 899–906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dempsey J., Veasey S., Morgan B., O’Donnel C. (2010) Pathophysiology of sleep apnea. Physiol Rev 90: 47–112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dieltjens M., Braem M., Vroegop A., Wouters K., Verbraecken J., De Backer W., et al. (2013) Objectively measured vs self-reported compliance during oral appliance therapy for sleep-disordered breathing. Chest 144: 1495–1502. [DOI] [PubMed] [Google Scholar]
- Dorkova Z., Petrasova D., Molcanyiova A., Popovnakova M., Tkacova R. (2008) Effects of continuous positive airway pressure on cardiovascular risk profile in patients with severe obstructive sleep apnea and metabolic syndrome. Chest 134: 686–92. [DOI] [PubMed] [Google Scholar]
- Epstein L., Kristo D., Strollo P., Friedman N., Malhotra A., Patil S., et al. (2009) Clinical guideline for the evaluation, management, and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med 5: 263–276. [PMC free article] [PubMed] [Google Scholar]
- Ferguson K., Cartwright R., Rogers R., Schmidt-Nowara W. (2006) Oral appliances for snoring and obstructive sleep apnea: a review. Sleep 29: 244–262. [DOI] [PubMed] [Google Scholar]
- Frank M., Ravesloot M., van Maanen J., Verhagen E., de Lange J., de Vries N. (2015) Positional OSA part 1: towards a clinical classification system for position-dependent obstructive sleep apnoea. Sleep Breath 19: 473–480. [DOI] [PubMed] [Google Scholar]
- Freedman N. (2014) Improvements in current treatments and emerging therapies for adult obstructive sleep apnea. F1000Prime Rep 6: 36–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gillespie M., Wylie P., Lee-Chiong T., Rapoport D. (2011) Effect of palatal implants on continuous positive airway pressure and compliance. Otolaryngol Head Neck Surg 144: 230–235. [DOI] [PubMed] [Google Scholar]
- Gotsopoulos H., Kelly J., Cistulli P. (2004) Oral appliance therapy reduces blood pressure in obstructive sleep apnea: a randomized, controlled trial. Sleep 27: 934–938. [DOI] [PubMed] [Google Scholar]
- Guilleminault C., Quo S. (2001) Sleep-disordered breathing. A view at the beginning of the new Millennium. Dent Clin North Am 45: 643–656. [PubMed] [Google Scholar]
- Guilleminault C., Tilkian A., Dement W. (1976) The sleep apnea syndromes. Annu Rev Med 27: 465–484. [DOI] [PubMed] [Google Scholar]
- Handler E., Hamans E., Goldberg A., Mickelson S. (2014) Tongue suspension: an evidence-based review and comparison to hypopharyngeal surgery for OSA. Laryngoscope 124: 329–336. [DOI] [PubMed] [Google Scholar]
- Health Quality Ontario (2009) Oral appliances for obstructive sleep apnea: an evidence-based analysis. Ont Health Technol Assess Ser 9: 1–51. [PMC free article] [PubMed] [Google Scholar]
- Holty J., Guilleminault C. (2010) Surgical options for the treatment of obstructive sleep apnea. Med Clin North Am 94: 479–515. [DOI] [PubMed] [Google Scholar]
- Iftikhar I., Valentine C., Bittencourt L., Cohen D., Fedson A., Gíslason T., et al. (2014) Effects of continuous positive airway pressure on blood pressure in patients with resistant hypertension and obstructive sleep apnea: a meta-,analysis. J Hyperten 32: 2341–2350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jordan A., McSharry D., Malhotra A. (2014) Adult obstructive sleep apnoea. Lancet 22: 736–747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jullian-Desayes I., Joyeux-Faure M., Tamisier R., Launois S., Borel A., Levy P., et al. (2014) Impact of obstructive sleep apnea treatment by continuous positive airway pressure on cardiometabolic biomarkers: a systematic review from sham CPAP randomized controlled trials. Sleep Med Rev 31: S1087–S1092. [DOI] [PubMed] [Google Scholar]
- Kendzerska T., Gershon A., Hawker G., Leung R., Tomlinson G. (2014) Obstructive sleep apnea and risk of cardiovascular events and all-cause mortality: a decade-long historical cohort study. PLoS Medicine 11: 1–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kezirian E., Boudewyns A., Eisele D., Schwartz A., Smith P., Van de Heyning P., et al. (2010) Electrical stimulation of the hypoglossal nerve in the treatment of obstructive sleep apnea. Sleep Med Rev 14: 299–305. [DOI] [PubMed] [Google Scholar]
- Kielb S., Ancoli-Israel S., Rebok G., Spira A. (2012) Cognition in obstructive sleep apnea-hypopnea syndrome (OSAS): current clinical knowledge and the impact of treatment. Neuromolecular Med 14: 180–193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kolla B., Olson E., Ramar K., Morgenthaler T. (2014) Bilevel positive airway pressure for obstructive sleep apnea. Expert Rev Med Devices 11: 283–294. [DOI] [PubMed] [Google Scholar]
- Kryger M., Berry R., Massie C. (2011) Long-term use of a nasal expiratory positive airway pressure (EPAP) device as a treatment for obstructive sleep apnea (OSA). J Clin Sleep Med 7: 449B–453B. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu Y., Lowe A., Fleetham J., Park Y. (2001) Cephalometric and physiologic predictors of the efficacy of an adjustable oral appliance for treating obstructive sleep apnea. Am J Orthod Dentofacial Orthop 120: 639–647. [DOI] [PubMed] [Google Scholar]
- Lojander J., Maasilta P., Partinen M., Brander P., Salmi T., Lehtonen H. (1996) Nasal-CPAP, surgery, and conservative management for treatment of obstructive sleep apnea syndrome. A randomized study. Chest 110: 114–119. [DOI] [PubMed] [Google Scholar]
- Marin J., Carrizo S., Vicente E., Agusti A. (2005) Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet 365: 1046–1053. [DOI] [PubMed] [Google Scholar]
- Marklund M., Sahlin C., Stenlund H., Persson M., Franklin K. (2001) Mandibular advancement device in patients with obstructive sleep apnea: long-term effects on apnea and sleep. Chest 20: 162–169. [DOI] [PubMed] [Google Scholar]
- Mehta A., Qian J., Petocz P., Darendeliler M., Cistulli P. (2001) A randomized, controlled study of a mandibular advancement splint for obstructive sleep apnea. Am J Respir Crit Care Med 163: 1457–1461. [DOI] [PubMed] [Google Scholar]
- Michels D., Rodrigues A., Nakanishi M., Sampaio A., Venosa A. (2014) Nasal involvement in obstructive sleep apnea syndrome. Int J Otolaryngol 2014: 8. doi: 10.1155/2014/717419 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Milleron O., Pilliere R., Foucher A., De Roquefeuil F., Aegerter P., Jondeau G., et al. (2004) Benefits of obstructive sleep apnoea treatment in coronary artery disease: a long-term follow-up study. Eur Heart J 25: 728–734. [DOI] [PubMed] [Google Scholar]
- Mitchell L., Davidson Z., Bonham M., O’Driscoll D., Hamilton G., Truby H. (2014) Weight loss from lifestyle interventions and severity of sleep apnoea: a systematic review and meta-analysis. Sleep Med 15: 1173–1183. [DOI] [PubMed] [Google Scholar]
- Montesi S., Edwards B., Malhotra A., Bakker J. (2012) The effect of continuous positive airway pressure treatment on blood pressure: a systematic review and meta-analysis of randomized controlled trials. J Clin Sleep Med 8: 587–596. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nadeem R., Singh M., Nida M., Kwon S., Sajid H., Witkowski J., et al. (2014) Effect of CPAP treatment for obstructive sleep apnea hypopnea syndrome on lipid profile: a meta-regression analysis. Lancet 383: 736–747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ngiam J., Balasubramaniam R., Darendeliler M., Cheng A., Waters K., Sullivan C. (2013) Clinical guidelines for oral appliance therapy in the treatment of snoring and obstructive sleep apnoea. Aust Dent J 58: 408–419. [DOI] [PubMed] [Google Scholar]
- Oksenberg A. (2005) Positional and non positional obstructive sleep apnea patients. Sleep Med 6: 377–378. [DOI] [PubMed] [Google Scholar]
- Patel S., White D., Malhotra A., Stanchina M., Ayas N. (2003) Continuous positive airway pressure therapy for treating sleepiness in a diverse population with obstructive sleep apnea: results of a meta-analysis. Arch Intern Med 163: 565–571. [DOI] [PubMed] [Google Scholar]
- Pételle B., Vincent G., Gagnadoux F., Rakotonanahary D., Meyer B., Fleury B. (2002) One-night mandibular advancement titration for obstructive sleep apnea syndrome: a pilot study. Am J Respir Crit Care Med 165: 1150–1153. [DOI] [PubMed] [Google Scholar]
- Prinsell J. (2002) Maxillomandibular advancement surgery for obstructive sleep apnea syndrome. J Am Dent Assoc 133: 1489–1497. [DOI] [PubMed] [Google Scholar]
- Randerath W., Verbraecken J., Andreas S., Bettega G., Boudewyns E., Hamans A. (2011) Non-CPAP therapies in obstructive sleep apnoea. Eur Respir J 37: 1000–1001. [DOI] [PubMed] [Google Scholar]
- Rossi V., Winter B., Rahman N., Yu L., Fallon J., Clarenbach C. (2013) The effects of Provent on moderate to severe obstructive sleep apnoea during continuous positive airway pressure therapy withdrawal: a randomised controlled trial. Thorax 68: 854–859. [DOI] [PubMed] [Google Scholar]
- Sarkhosh K., Switzer N., El-Hadi M., Birch D., Shi X., Karmali S. (2013) The impact of bariatric surgery on obstructive sleep apnea: a systematic review. Obes Surg 23: 414–423. [DOI] [PubMed] [Google Scholar]
- Schäfer H., Ewig S., Hasper E., Lüderitz B. (1998) Failure of CPAP therapy in obstructive sleep apnoea syndrome: predictive factors and treatment with bilevel-positive airway pressure. Respir Med 92: 208–215. [DOI] [PubMed] [Google Scholar]
- Sharma S., Agrawal S., Damodaran D., Sreenivas V., Kadhiravan T., Lakshmy R., et al. (2011) CPAP for the metabolic syndrome in patients with obstructive sleep apnea. N Engl J Med 365: 2277–2286. [DOI] [PubMed] [Google Scholar]
- Smith I., Lasserson T. (2009) Pressure modification for improving usage of continuous positive airway pressure machines in adults with obstructive sleep apnoea. Cochrane Database Syst Rev (4): CD003531. [DOI] [PubMed] [Google Scholar]
- Spicuzza L., Leonardi S., La Rosa M. (2009) Pediatric sleep apnea: early onset of the ‘syndrome’? Sleep Med Rev 13: 111–122. [DOI] [PubMed] [Google Scholar]
- Stanley I., D’Ambrosio C., Patel K., Obadan N., Kitsios G., Chung M., et al. (2012) Auto-titrating versus fixed continuous positive airway pressure for the treatment of obstructive sleep apnea: a systematic review with meta-analyses. Syst Rev 8: 20–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stasche N. (2006) Selective indication for positive airway pressure (PAP) in sleep-related breathing disorders with obstruction. GMS Curr Top Otorhinolaryngol Head Neck Surg 5: Doc06. [PMC free article] [PubMed] [Google Scholar]
- Strollo P., Jr, Soose R., Maurer J., de Vries N., Cornelius J., Froymovich O., et al. (2014) Upper-airway stimulation for obstructive sleep apnea. N Engl J Med 370: 139–149. [DOI] [PubMed] [Google Scholar]
- Sullivan C., Berthon-Jones M., Issa F. (1983) Nocturnal nasal-airway pressure for sleep apnea. N Engl J Med 309–112. [DOI] [PubMed] [Google Scholar]
- Sutherland K., Vanderveken O., Tsuda H., Marklund M., Gagnadoux F., Kushida C., et al. (2014) Oral appliance treatment for obstructive sleep apnea: an update. J Clin Sleep Med 10: 215–227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tregear S., Reston J., Schoelles K., Phillips B. (2010) Continuous positive airway pressure reduces risk of motor vehicle crash among drivers with obstructive sleep apnea: systematic review and meta-analysis. Sleep 33: 1373–1380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tuomilehto H., Seppä J., Uusitupa M. (2013) Obesity and obstructive sleep apnea – clinical significance of weight loss. Sleep Med Rev 17: 321–329. [DOI] [PubMed] [Google Scholar]
- Vaessen T., Overeem S., Sitskoorn M. (2014) Cognitive complaints in obstructive sleep apnea. Sleep Med Rev 19: 51–58. [DOI] [PubMed] [Google Scholar]
- Vanderveken O., Devolder A., Marklund M., Boudewyns A., Braem M., Okkerse W., et al. (2008) Comparison of a custom-made and a thermoplastic oral appliance for the treatment of mild sleep apnea. Am J Respir Crit Care Med 178: 178–197. [DOI] [PubMed] [Google Scholar]
- Verse T., Hörmann K. (2011) The surgical treatment of sleep-related upper airway obstruction. Dtsch Arztebl Int 108: 216–221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wozniak D., Lasserson T., Smith I. (2014) Educational, supportive and behavioural interventions to improve usage of continuous positive airway pressure machines in adults with obstructive sleep apnoea. Cochrane Database Syst Rev (1): CD007736. [DOI] [PubMed] [Google Scholar]
- Young T., Finn L., Peppard P., Szklo-Coxe M., Austn D., Nieto F., et al. (2008) Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep 31: 1071–1078. [PMC free article] [PubMed] [Google Scholar]
- Young T., Palta M., Dempsey J., Skatrud J., Weber S., Badr S. (1993) The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med 32: 1230–1235. [DOI] [PubMed] [Google Scholar]
- Zeng B., Ng A., Qian J., Petocz P., Darendeliler M., Cistulli P. (2008) Influence of nasal resistance on oral appliance treatment outcome in obstructive sleep apnea. Sleep 31: 543–547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zimmerman M., Arnedt J., Stanchina M., Millman R., Aloia M. (2006). Normalization of memory performance and positive airway pressure adherence in memory-impaired patients with obstructive sleep apnea. Chest 130: 1772–1778. [DOI] [PubMed] [Google Scholar]