

Abstract
Background and Aim:
Central corneal thickness (CCT) of term and preterm infants in Indian population is not known. We did a prospective noninterventional study to measure the CCT in term and preterm infants.
Materials and Methods:
An ultrasonic pachymeter was used. The data regarding the date of birth, expected date of delivery, birth weight were recorded. The preterm and the term infants were followed up at 8 weeks, 20 weeks and at 1-year.
Results:
A total of 85 (170 eyes) children were included in the study. The mean age was 264.6 ± 21.8 days postconception. The mean birth weight and CCT were 1834.4 ± 512.1 g and 595.8 ± 72.4 μ respectively. A comparison of CCT on the basis postgestational age showed a mean thickness of 620.7 ± 88.8 and 574.4 ± 78.3 μ in the <260 days and >260 days age groups respectively. The difference was statistically significant (Student's test, P = 0.002). The CCT of preterm infants (<260 days) decreased from a mean value of 620.7 ± 88.8 μ to 534.1 ± 57.6 μ at the end of 1-year.
Conclusion:
We present the data of CCT in term and preterm infants in Indian population. We believe that the premature babies have slightly thicker corneas than mature term babies.
Keywords: Central corneal thickness, preterm infants, term infants
Central corneal thickness (CCT) has become an important parameter for diagnosis and treatment of various eye disorders. More and more children are now born at very low gestational age. There is very scant data on the CCT of premature and full-term children during the neonatal period. Autzen and Bjørnstrøm[1] (13 premature infants), Kirwan et al.[2] (35 premature infants) and more recently by De Silva et al.[3] (56 premature infants), Uva et al.[4] (33 premature infants) and Gunay et al.[5] (100 premature infants) have presented their findings on the CCT in premature children. We, therefore, decided to do a prospective noninterventional study to measure the CCT in preterm and term infants in Indian population. This is to the best of our knowledge the first study in Indian population and the only study, which has followed up the same set of neonates for the measurement of CCT.
Materials and Methods
A total of 85 (170 eyes) children were included in the study. The study was done at Krishna Children Critical Care, Vadodara and Synergy NICU, Ahmedabad. Who underwent retinopathy of prematurity screening program and all examinations were performed within first 2 days of birth. Informed consent was obtained from the parents. An ultrasonic pachymeter (300 AP + Pacscan Plus, Sonomed Escalon, Stoneham, MA, USA) used to measure the CCT for both the eyes of all the neonates. Topical anesthesia was achieved by proparacaine eye drops. A total of 5 readings were taken for each eye and the lower and higher readings were excluded. The rest of three readings were averaged and included. No speculum was used during the measurement of the data. The data regarding date of birth expected date of delivery and birth weight were recorded. For the purpose of comparison, we took a postconceptional age (PCA) only. The PCA of each infant was determined based on obstetric history, early obstetric ultrasound and confirmed by clinical examination of the newborn infant. Similar to other studies reported in the literature, exclusion criteria were retinopathy of prematurity Stage II or higher and neurological or syndromic diseases. None of the patients on gross examination seems to have corneal dystrophy. Any cases of trauma to cornea/lid or other structures were excluded. Ocular abnormalities such as corneal and iris alterations, congenital cataract, retinopathy and glaucomatous optic disc changes (CD >0.4) were excluded. Patients with factors possibly affecting intraocular pressure (mechanical ventilation or pulmonary or circulatory complications) also were excluded.
None of the parents had a history of consanguinity. Any baby with a history of forceps delivery or trauma to any ocular structure was excluded from the study. The preterm and term infants were followed up at 8 weeks, 20 weeks and at 1-year and CCT were measured on all follow-up visits. Only children who came to us for the 1-year follow-up were included.
Results
A total of 85 infants (170 eyes) with 43 term infants (86 eyes) and 42 preterm infants (84 eyes) were included in the study. Mean CCT was 595.8 ± 72.4 μ in 170 eyes. For the purpose of calculation, the age at which CCT was measured was divided on the basis of PCA of more than and less than and equal to 260 days postconception.
The mean age of the children in ≤260 days, PCA was 242.4 ± 15.1 days and in the >260 days PCA group was 278.9 ± 9.1 days. The mean birth weight was 1410.5 ± 305.2 g and 2105.1 ± 498.8 g in the ≤260 days PCA and >260 days PCA groups respectively. The P = 0.00002 was highly significant. The mean CCT in the ≤260 days PCA and >260 days PCA was 620.7 ± 88.8 and 574.4 ± 78.3 μ respectively. The P value was 0.002 (Student's t-test) and was highly significant.
The comparison of CCT was also done on the basis of weight of the baby (not the birth weight) at the time of examination. The infants (term and preterm) were divided in three groups <1500 g, 1500–2000 g and >2000 g; the mean CCT was 610.3 ± 88.4, 599.6 ± 93.4 and 578.4 ± 71.8 μ respectively in the three groups. The P value was not significant on inter-group comparison ANOVA though it seems that the higher birth weight had thinner central corneas.
The CCT of preterm infants remained higher compared to term infants but was not statistically significant. The CCT of preterm infants (<260 days) decreased from the mean value of 620.7 ± 88.8 μ to 578.3 ± 79.6 μ at the end of 8 weeks. At the end of 20 weeks, it was 558.4 ± 52.4 μ which further reduced to 534.1 ± 57.6 μ at the end of 1-year. The CCT of the infants (>260 days postconception) decreased from 574.4 μ to 556.6 μ (8 weeks), 544.6 μ (20 weeks) and 530.2 μ (1-year) [Fig. 1].
Figure 1.
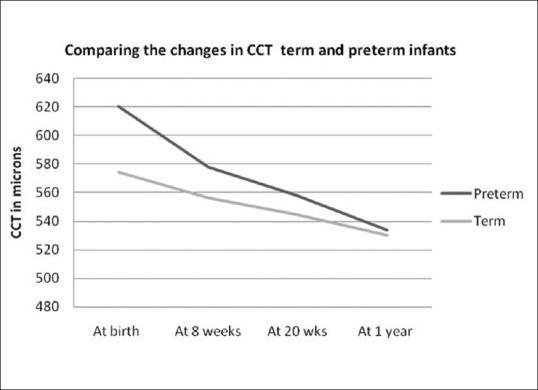
The comparison of central corneal thickness in term and preterm infants and the gradual reduction in the thickness of cornea over a period of 1-year
Discussion
Autzen and Bjørnstrøm[1] reported CCT values of 656 ± 103 μ at 5 days of life, 654 ± 84 μ at 20 days and 566 ± 64 μ at 110 days. They found no difference in CCT at the first and third postnatal week and that at the age of 3 months the thickness decreases to the same level of the full-term newborns. No correlation was found between gestational age and CCT. However, Kirwan et al.[2] studied 35 premature infants (70 eyes), born at a gestational age ranging from 23 to 32 weeks, in four PCA groups: 30–32, 34–35, 37–38, and 39–41 weeks. At these ages, CCT was 691 ± 87, 648 ± 72, 605 ± 59 and 564 ± 34 μ, respectively. De Silva et al.[3] (n = 56) showed a gradual decrease in the CCT from 794 ± 34 μ at 28 weeks PCA to 559 ± 13 μ at 42 weeks PCA. Uva et al.[4] reported a mean CCT of 599 ± 36 μ in premature newborns (n = 33). Our data of 620.7 ± 88.8 μ for children for preterm children is similar to reported by Uva et al.[4] but lower than the studies by Autzen and Bjørnstrøm,[1] Kirwan et al.,[2] De Silva et al.[3] and Gunay et al.[5]
Studies on full-term newborns at birth found CCTs ranging from 573 to 585 μ [Table 1].[6,7,8] Our study shows a CCT of 574.4 ± 78.3 μ for term infants. Ehlers et al.[9] noted that there is a small further reduction in the CCT and reaches the value of the adult cornea at the age of 3 years.[9] CCT values of premature infants at a PCA of 40 weeks are therefore similar to those obtained in newborns of 40 weeks of gestation. De Silva et al.[3] reported a CCT of 546 ± 12 μ at 40 weeks PCA whereas Uva et al.[4] reported a CCT of 576 ± 26 μ in full-term newborns. Our data of 574.4 ± 78.3 μ are very similar to Uva et al.[4] and is in complete agreement with the majority of studies[7,8,10] [Table 2] except for the study by De Silva et al.[3] The reduction in the corneal thickness started within first few weeks in our study. The children in our study had a slightly higher thickness even at the end of 1-year compared to the term infants.
Table 1.
Mean central corneal thickness in preterm and term infants

Table 2.
Comparison of previous studies and our data on central corneal thickness in preterm and term infants

Birth weight was analyzed by Uva et al.[4] and on multivariate analysis they found a significant correlation of CCT with birth weight. Gunay et al.[5] also correlated birth weight and CCT. His study on premature children suggested that the birth weight was negatively correlated with CCT. Though in our study it was obvious that birth weight would be an important factor, we believe that since birth weight was significantly lower in the premature infants, a correlation of thicker corneas with lower birth weight was likely and therefore we took into consideration the actual weight at the time of examination (not the birth weight) and found no significant difference. It could have still been possible that all low birth weight babies were premature ones as their weights would have improved at a slower rate compared to the term infants. However, the data does suggest that an infant with lower weight has a thicker cornea.
This reduction in cornea thickness has been correlated with the increased transparency of the infant corneas secondary to evaporation, corneal remodeling as they grow.[4] The experimental evidence that the corneal hydration is the cause for the reduced transparency has also been linked with the increased thickness of the cornea in younger infants.[3] Since we did not measure other ocular parameters of the eye, we cannot attribute the reason for thinning of the cornea to the reduction of corneal edema, it could be because of increase in corneal diameter. This would, however, require further studies in the light of present finding that the cornea is thin in older neonates.
Conclusion
Central corneal thickness is higher in the preterm infants (related to PCA and weight) than in the term infants in Indian population. The lower birth weight seems to be an independent factor for CCT. The corneal thickness reduces with age and is almost similar to term infants by 20 weeks of age. The values should be kept in mind while dealing with corneal problems in preterm and term infants in Indian population.
Acknowledgment
The authors thank Krishna Children Critical Care, Vadodara, Synergy children critical care, Ahmedabad and NICU, Civil hospital, Ahmedabad for their cooperation and support.
Footnotes
Source of Support: Nil.
Conflicts of Interest: None declared.
References
- 1.Autzen T, Bjørnstrøm L. Central corneal thickness in premature babies. Acta Ophthalmol (Copenh) 1991;69:251–2. doi: 10.1111/j.1755-3768.1991.tb02720.x. [DOI] [PubMed] [Google Scholar]
- 2.Kirwan C, O’Keefe M, Fitzsimon S. Central corneal thickness and corneal diameter in premature infants. Acta Ophthalmol Scand. 2005;83:751–3. doi: 10.1111/j.1600-0420.2005.00559.x. [DOI] [PubMed] [Google Scholar]
- 3.De Silva S, Parentin F, Michieletto P, Pensiero S. Corneal curvature and thickness development in premature infants. J Pediatr Ophthalmol Strabismus. 2011;48:25–9. doi: 10.3928/01913913-20100318-02. [DOI] [PubMed] [Google Scholar]
- 4.Uva MG, Reibaldi M, Longo A, Avitabile T, Gagliano C, Scollo D, et al. Intraocular pressure and central corneal thickness in premature and full-term newborns. J AAPOS. 2011;15:367–9. doi: 10.1016/j.jaapos.2011.04.004. [DOI] [PubMed] [Google Scholar]
- 5.Gunay M, Celik G, Gunay BO, Dogru M, Gursoy T, Ovali HF. Central corneal thickness measurements in premature infants. Int J Ophthalmol. 2014;7:496–500. doi: 10.3980/j.issn.2222-3959.2014.03.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Autzen T, Bjørnstrøm L. Central corneal thickness in full-term newborns. Acta Ophthalmol (Copenh) 1989;67:719–20. doi: 10.1111/j.1755-3768.1989.tb04409.x. [DOI] [PubMed] [Google Scholar]
- 7.Portellinha W, Belfort R Jr. Central and peripheral corneal thickness in newborns. Acta Ophthalmol (Copenh) 1991;69:247–50. doi: 10.1111/j.1755-3768.1991.tb02719.x. [DOI] [PubMed] [Google Scholar]
- 8.Remón L, Cristóbal JA, Castillo J, Palomar T, Palomar A, Pérez J. Central and peripheral corneal thickness in full-term newborns by ultrasonic pachymetry. Invest Ophthalmol Vis Sci. 1992;33:3080–3. [PubMed] [Google Scholar]
- 9.Ehlers N, Sorensen T, Bramsen T, Poulsen EH. Central corneal thickness in newborns and children. Acta Ophthalmol (Copenh) 1976;54:285–90. doi: 10.1111/j.1755-3768.1976.tb01257.x. [DOI] [PubMed] [Google Scholar]
- 10.Muslubas IB, Oral AY, Cabi C, Caliskan S. Assessment of the central corneal thickness and intraocular pressure in premature and full-term newborns. Indian J Ophthalmol. 2014;62:561–4. doi: 10.4103/0301-4738.133486. [DOI] [PMC free article] [PubMed] [Google Scholar]