

Abstract
Small cell lung cancer (SCLC) metastasizes widely, but palatine tonsil is an extremely unusual site for metastasis. Idiopathic pulmonary fibrosis (IPF) is associated with increased risk of lung cancer. However, the most common histological findings among patients of lung cancer with IPF are known as non-SCLC such as adenocarcinoma and squamous cell carcinoma. In addition, the majority of them are located in IPF-associated fibrotic peripheral lesions.
A 77-year-old man visited for 1-month persistent cough and dyspnea, with inspiratory dry crackles on both lower lung fields and a large oval mass in his throat. Chest computed tomography revealed 2 masses in the left lower lobe, 1 mass in the right upper lobe, and multiple enlarged mediastinal lymph nodes of the lung accompanying with IPF, which were diagnosed as SCLC pathologically. Very interestingly, the tonsillar mass was also confirmed as the metastatic lesion of SCLC. Chemotherapy for SCLC and medical treatment for IPF were applied. However, in following-up, he expired due to respiratory failure by an acute exacerbation of IPF 3 months after the diagnosis.
In this current report, we describe, for the first time, a case of tonsillar metastasis of SCLC with IPF detected simultaneously in a 77-year-old man.
INTRODUCTION
Small cell lung cancer (SCLC) is highly malignant neoplasm, derived from neuroendocrine cells. It represents approximately 15% of all bronchial carcinomas, and this percentage is tending to decrease recently. In most cases, SCLC arises in the larger airways and grows rapidly, becoming quite large.1 It also has propensity to metastasize widely throughout the body at an early stage in its clinical course.2 The most common metastatic sites are liver, brain, and adrenal glands. Tonsillar metastasis from SCLC is extremely rare, and clinically apparent cases are even less common.3
Idiopathic pulmonary fibrosis (IPF) is a chronic, progressive form of interstitial lung disease with poor prognosis and is a clinical term of usual interstitial pneumonia of unknown cause. It has been reported to be associated with increased risk of lung cancer.4 In a study, the incidence of lung cancer was increased 7-fold in the IPF group compared with healthy subjects.5 Although the features of the lung cancer with IPF are similar to the general features of lung cancer, SCLC is not common in fibrotic area of IPF.4
The present case report describes SCLC in IPF-associated lesion and its tonsillar metastasis, which is rarely seen.
CASE REPORT
A 77-year-old man admitted to our hospital with 1-month history of cough and dyspnea. He had personal history of pulmonary tuberculosis 1 year ago. On physical examination of the thorax, inspiratory dry crackles were heard on both lower lung fields. In observation of oral cavity, a large oval mass composed of soft tissue was detected in his throat. The mass was arising from the right palatine tonsil and extending across the midline of the oropharynx (Figure 1A).
FIGURE 1.
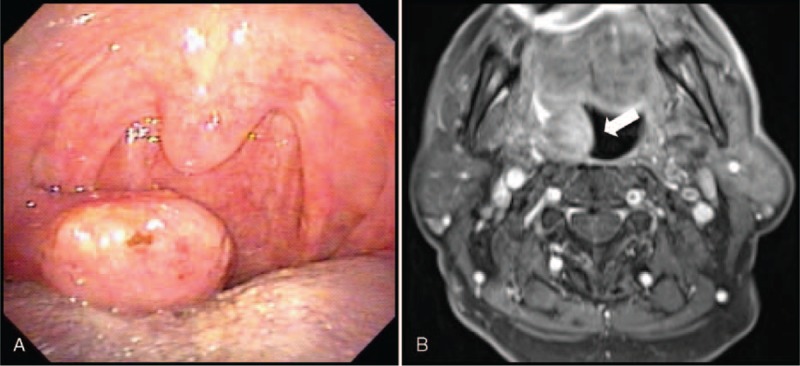
(A) In physical examination, a large oval mass composed of soft tissue arose from the right palatine tonsil and extended across the midline of the oropharynx. (B) Whole-body magnetic resonance revealed intraluminal protruding mass in the right peritonsillar region with heterogeneous enhancement, suggesting malignancy of palatine tonsil.
High-resolution computed tomography of chest showed 2 masses in the left lower lobe, 1 mass in the right upper lobe, and multiple enlarged mediastinal lymph nodes of the lung (Figure 2). One of the left lower lobe masses was 4.4 × 4.0 cm sized in superior and lateral segments, and the other was 5.7 × 3.7 cm sized with fibrosis in subpleural region. A right upper lobe mass was 2.1 × 1.5 cm sized. Also, there was typical honeycomb appearance with traction bronchiectasis and ground-glass opacity pattern, predominantly in subpleural areas of both lower lobes. Under suspicion of lung cancer and usual interstitial pneumonia that is pathological equivalent to IPF, further workup was started to confirm the diagnosis.
FIGURE 2.
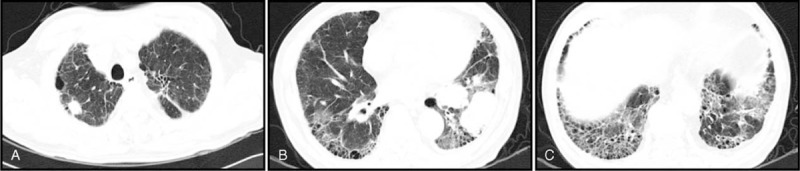
High-resolution computed tomography showed 1 mass in the right upper lobe (A), 2 masses in the left lower lobe (B), and honeycomb appearance in subpleural area of both lower lobe (C).
Percutaneous transthoracic needle biopsy for lung mass and punch biopsy for tonsillar lesion were performed. Both tumors were composed of nests of small, round, or oval cells with little cytoplasm and hyperchromatic nuclei. They also showed molding and crushing artifact. In immunohistochemical staining, the cells from both tumors were positive for CD56, a glycoprotein expressed on the surface of neurons and neuroendocrine tumors as well known that it is the neural cell adhesion molecule (NCAM). In addition, the cells showed positive staining for synaptophysin and chromogranin A, although the intensity was weaker than CD56, and it was more distinct in lung mass than that in tonsillar mass. Based on these pathologic findings and the known fact that SCLC belongs to the neuroendocrine lineage of lung cancer, the masses were diagnosed as SCLC and tonsillar metastasis (Figure 3).
FIGURE 3.

Representative H&E sections of lung mass (A) and tonsillar mass (B) revealed nests of small, round, or oval cells with little cytoplasm and hyperchromatic nuclei in both lesions. In immunohistochemical staining for CD 56 of lung mass (C) and tonsillar mass (D), the cells were positive for CD56 presenting for SCLC. CD = cluster of differentiation, SCLC = small cell lung cancer.
We performed systemic evaluation using whole-body magnetic resonance imaging, which showed a mass indicating brain metastasis in body portion of the right corpus callosum and a 2 × 2.8 cm-sized, intraluminal protruding mass in the right peritonsillar region with heterogeneous enhancement, suggesting malignancy of palatine tonsil (Figure 1B).
We suspected that the patient has IPF based on the clinical findings and radiological patterns. There was no history of exposure to any toxic materials and no clinical symptoms of connective tissue diseases. Bronchioloalveolar lavage fluid analysis exhibited the percentage of alveolar macrophage, lymphocytes, neutrophil, and eosinophil was 77%, 3%, 15%, and 5%, respectively. T-cell helper/suppressor ratio was 0.97. The analysis of bronchioalveolar lavage did not show any other abnormal cells or components. Pulmonary function test revealed restrictive pattern of ventilation. With all these findings, we diagnosed that the patient had IPF.
Chemotherapy with irinotecan and carboplatin for SCLC and a standard medication of steroid and acetylcysteine for IPF were applied. He received gamma-knife surgery for metastatic brain cancer 2 weeks later. However, in following-up, he expired due to respiratory failure by an acute exacerbation of IPF 3 months after the diagnosis.
DISCUSSION
Small cell carcinoma is renowned for its tendency to disseminate widely throughout body. Susceptible organs include the liver, abdominal lymph node, bone, brain, adrenal gland, skin, kidney, and pancreas. A few cases of tonsillar metastasis of SCLC have been reported.6–8
The palatine tonsil is a rare site in which metastatic tumor deposit is found. According to a study, only 12 tumors (0.8%) were due to metastasis in a series of 1547 tonsillar tumors.9 The metastatic tumors include carcinoma of the breast, stomach, renal cell carcinoma, seminoma, melanoma, and carcinoma of rectum. Furthermore, in a review of 76 cases of primary neoplasm complicated by tonsillar metastasis, only 12 were found to be due to carcinoma of the bronchus.10 Among these 12 metastatic cases, 2 cases were unilateral and 10 cases were bilateral. Evidence for the metastasis to other tissues was found in 10 of the 12 cases.
In all reported cases of tonsillar metastasis of SCLC, the metastasis developed following presentations3,6,8,11: The mean interval of time between development of the primary bronchogenic cancer and the tonsillar metastasis was 8 months, and the mean time interval between appearance of the tonsillar metastasis and death was 5 months. In our present case, tonsillar metastasis and primary SCLC were diagnosed simultaneously, making the case more interesting. Most patients with tonsillar metastasis are symptomatic, such as difficulty in breathing, sore throat, irritable cough, dysphagia, otalgia, and swallowing pain accompanied by a foreign body-like sensation.6,8,12 However, in our case, the patient with tonsillar metastasis of SCLC did not show any of these symptoms.
Interstitial lung disease and lung cancer are 2 of the most common respiratory diseases. IPF, which is the most frequent type of interstitial lung diseases, has been reported as an independent risk factor for lung cancer by epidemiological studies.13–15 Recent studies have reported that alteration of genes like fragile histidine triad (FHIT) gene is associated with lung cancer and IPF, supporting that lung cancer can be a result of the occurrence of atypical or dysplastic epithelial changes in fibrosis.11,16 In that situation, the cancer would develop in the area of major fibrosis.
IPF is significantly related to the development of lung cancer in peripheral location of the lower lobes.15,17,18 Adenocarcinoma and squamous cell carcinoma are the most common histological findings among lung cancer patients with IPF.17–19 Cancers are mostly located in IPF-associated fibrotic lesions.4,11 However, SCLC, which is a central disease, shows exceptional tendency to occur in the IPF-nonassociated and nonfibrotic lesion.4 Our case is interesting in the point that SCLC has developed from IPF-associated fibrotic lesion of left lower lobe.
Considering our case presented here, physicians should include metastatic SCLC as the differential diagnosis for a single tonsillar mass, although the incidence is very low. In addition, this case shows that SCLC can be developed in IPF-associated fibrotic lesion, indicating that physicians should consider a possible association between SCLC and lung fibrosis such as IPF.
ETHICAL REVIEW AND PATIENT CONSENT
Institutional Review Board of Chonbuk National University Hospital has stated that it is not necessary to achieve IRB approval for this case report, and this report requires obtaining patient consent because this study is dealt with only the patient's medical record and related images, retrospectively. Written informed consent of this case report and accompanying images was obtained from the patient for the publication.
Acknowledgment
We thank Professor Mie-Jae Im (Chonbuk National University Medical School, Jeonju, South Korea) for critical readings of the manuscript.
Footnotes
Abbreviations: FHIT gene = fragile histidine triad gene, IPF = idiopathic pulmonary fibrosis, SCLC = small cell lung cancer.
This work was supported by the Korea Healthcare Technology R&D Project, Ministry for Health and Welfare, Republic of Korea (Grant A121931), by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT and future Planning (NRF-2014R1A2A1A01002823), and by the fund of Biomedical Research Institute, Chonbuk National University Hospital.
The authors have no conflicts of interest to disclose.
SRK and YCL contributed equally to this work.
REFERENCES
- 1.Collins LG, Haines C, Perkel R, et al. Lung cancer: diagnosis and management. Am Fam Physician 2007; 75:56–63. [PubMed] [Google Scholar]
- 2.Hanson HH, Rorth M. Flenley DE, Petty TL. Small cell carcinoma of the lung. Recent advances in respiratory medicine. Edinburgh: Churchill-Livingstone; 1983. 193–202. [Google Scholar]
- 3.Seddon DJ. Tonsillar metastasis at presentation of small cell carcinoma of the lung. J R Soc Med 1989; 82:688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Park J, Kim DS, Shim TS, et al. Lung cancer in patients with idiopathic pulmonary fibrosis. Eur Respir J 2001; 17:1216–1219. [DOI] [PubMed] [Google Scholar]
- 5.Hubbard R, Venn A, Lewis S, et al. Lung cancer and cryptogenic fibrosing alveolitis: a population based cohort study. Am J Respir Crit Care Med 1999; 161:5–8. [DOI] [PubMed] [Google Scholar]
- 6.Arzu Y, Serkan D, Şenay T, et al. Tonsillar metastasis from small cell lung cancer: Rare but occurs. Turk J Cancer 2009; 39:28–30. [Google Scholar]
- 7.Bozza F, Piantanida R, Pellini R, et al. Palatine tonsillar metastasis from small cell carcinoma of the lung. Acta Otorhinolaryngol Ital 2000; 20:281–283. [PubMed] [Google Scholar]
- 8.Hisa Y, Yasuda N, Murakami M. Small cell carcinoma of the lung metastatic to the palatine tonsil. Otolaryngol Head Neck Surg 1997; 116:563–564. [DOI] [PubMed] [Google Scholar]
- 9.Samet JM. Does idiopathic pulmonary fibrosis increase lung cancer risk? Am J Respir Crit Care Med 2000; 161:1–2. [DOI] [PubMed] [Google Scholar]
- 10.Brownson RJ, Jaques WE, Lamonte SE, et al. Hypernephroma metastatic to the palatine tonsils. Ann Oto Rhinol Laryngol 1979; 88:235–240. [DOI] [PubMed] [Google Scholar]
- 11.Elidan J, Brama I, Gay J. A large tonsillolith simulating tumor of the tonsil. Ear Nose Throat J 1980; 59:296–297. [PubMed] [Google Scholar]
- 12.Sezer B, Tugsel Z, Bilgen C. An unusual tonsillolith. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003; 95:471–473. [DOI] [PubMed] [Google Scholar]
- 13.Nagai A, Chiyotani L, Nakadate T, et al. Lung cancers in patients with idiopathic pulmonary fibrosis. Tohoku J Exp Med 1992; 167:231–237. [DOI] [PubMed] [Google Scholar]
- 14.Kawai T, Yakumaru K, Suzukiet M, et al. Diffuse interstitial pulmonary fibrosis and lung caner. Acta Pathol Jpn 1987; 37:11–19. [DOI] [PubMed] [Google Scholar]
- 15.Mizushima Y, Kobayashi M. Clinical characteristics of synchronous multiple lung cancer associated with idiopathic pulmonary fibrosis. Chest 1995; 108:1272–1277. [DOI] [PubMed] [Google Scholar]
- 16.Demopoulos K, Arvanitis DA, Vassilakis DA, et al. MYCL1, FHIT. SPARC, p16(INK4) and TP53 genes associated to lung cancer in idiopathic pulmonary fibrosis. J Cell Mol Med 2002; 6:215–222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Crawford BE, Callihan MD, Corio RL, et al. Oral pathology. Otolaryngol Clin North Am 1979; 12:29–43. [PubMed] [Google Scholar]
- 18.Lee HJ, Im JG, Ahn JM, et al. Lung cancer in patients with idiopathic pulmonary fibrosis: CT findings. J Comput Assist Tomogr 1996; 20:979–982. [DOI] [PubMed] [Google Scholar]
- 19.Kishi K, Homma S, Kurosaki A, et al. High-resolution computed tomography findings of lung cancer associated with idiopathic pulmonary fibrosis. J Comput Assist Tomogr 2006; 30:95–99. [DOI] [PubMed] [Google Scholar]