

Abstract
Background:
Many risk factors for throwing injuries have been proposed. However, little is known about the risk factors for elbow injuries, particularly on physeal injuries in youth baseball players without prior elbow pain.
Purpose:
To investigate the risk factors for elbow injuries with a focus on physeal injuries that could predispose youth baseball players without elbow pain to elbow injuries.
Study Design:
A prospective epidemiology study.
Methods:
In 2006, 449 players without prior elbow pain were observed prospectively for 1 season to study injury incidence in relation to specific risk factors. The average age was 10.1 years (range, 7-11 years). One year later, all players were examined by administering a questionnaire, physical examination, and radiographic examination. Data for the groups with and without elbow pain were analyzed using multivariate logistic regression models.
Results:
Among the 449 participants, 30.5% reported episodes of elbow pain during the season. Of the players who reported elbow pain, 72.3% presented abnormal findings on physical examination, and of those players, 81.4% had radiographic abnormalities. Multivariate analysis showed that the age of 12 years (at 1-year examination), pitcher and catcher positions, and playing more than 100 games per year were risk factors for elbow pain.
Conclusion:
It is expected that 30% of youth baseball players have elbow pain each year, and nearly 60% of players with elbow pain exhibit radiographic abnormalities. The age of 12 years, pitcher and catcher positions, and playing more than 100 games per year are risk factors for elbow pain.
Keywords: elbow, baseball, youth, risk factors, physeal injury
Baseball is a sport enjoyed by millions of young athletes worldwide. Although baseball is relatively safe, numerous reports suggest a rapid rise in elbow injury rates among youth baseball players. Such injuries that become evident in high school and college are believed to begin at the youth level and are caused by cumulative recurrent microtrauma.1,10,12
Many risk factors for throwing injuries have been proposed and include the immature skeleton, throwing mechanics, glenohumeral internal rotation deficit, pitch type, velocity, and number of throws. However, little evidence is available to support the majority of these factors. Lyman et al10,11 followed youth baseball pitchers and found that the incidence of elbow pain increased in line with age and number of pitches per season. Harada et al6 investigated prospectively pitchers and nonpitchers and showed that pitchers have a 4.5 times higher incidence of elbow injury than nonpitchers. However, their study included players who already had elbow pain at the beginning of the investigation. It is necessary to examine risk factors for elbow injuries in young baseball players without prior elbow pain. Furthermore, in pediatric athletes, injury patterns are influenced by the age-related stage of elbow development.8 Physeal injuries often occur in young throwers in situations that would otherwise lead to ligamentous injuries in adult throwers.7
The aim of this study was to investigate the risk factors that could predispose youth baseball players without prior history of elbow pain to elbow injuries.
Materials and Methods
This study was approved by the Institutional Review Board of Tokushima University Hospital, and all parents and coaches provided informed consent.
A total of 621 players participated in the regional summer championship in July 2006. Of 621 players, 172 had a history of elbow pain. The remaining 449 players (mean age, 10.1 years; range, 7-11 years) belonged to youth baseball teams and were the subjects of this investigation. One year later, in July 2007, subjects were examined by administering a questionnaire, physical examination, and radiographic examination. None of the players in our study had thrown curveballs or sliders; all had thrown fastballs or change-ups.
Questionnaires were distributed to the team coaches, and information was filled out by subjects with the assistance of coaches and/or parents. Subjects were asked whether they had experienced any episodes of elbow pain during the season. The questionnaire was also used to gather data on age, position, number of training days per week, and number of games per year. The first author (T.M.) reviewed the questionnaire with each subject to increase the players’ understanding of the questions and check the accuracy of the information.
Physical examination of the elbow was recommended to players who complained of elbow pain on the questionnaire. Range of motion, tenderness, and the valgus stress test were included in the physical examination. Limitations of range of motion were regarded as positive if the difference between the throwing and nonthrowing arms was more than 5°.
Radiographic examination was recommended to players who had positive findings on physical examination. Anteroposterior radiographs of the elbow in 45° of flexion and lateral were taken. Films were reviewed at the office by 2 authors (T.M. and N.S.) in a blinded fashion.
We investigated the following risk factors for elbow injury: age, position, number of training days per week, and number of games per year. Data were analyzed by multivariate logistic regression models and presented as odds ratio (OR) and profile likelihood 95% confidence interval (CI) values. The likelihood-ratio test was also performed. A 2-tailed P value less than .05 was considered significant. All analysis was done in the SAS software package (version 8.2; SAS Institute, Cary, North Carolina, USA).
Results
Figure 1 summarizes the overall results of the examination. Of the 449 subjects, 137 (30.5%) reported episodes of pain in the throwing elbow during the season. The remaining 312 subjects had no prior elbow pain.
Figure 1.
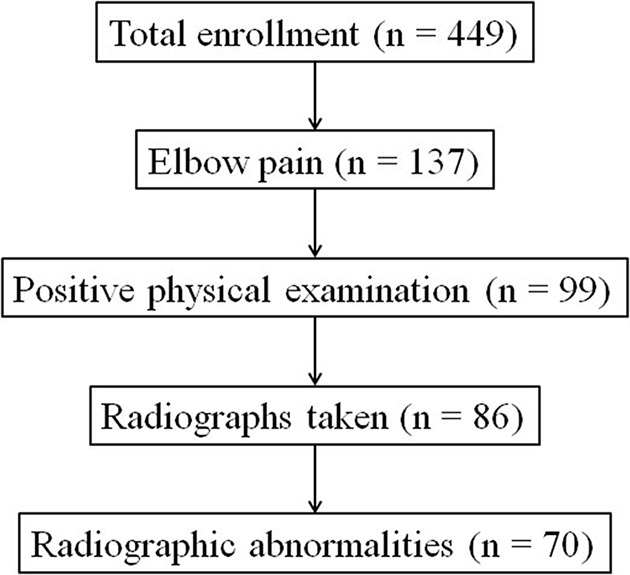
Outcomes of elbow examination.
Of the 137 players who reported elbow pain, 99 (72.3%) presented abnormal findings in the physical examination. A limitation of extension was found in 32 (23.4%) subjects, and a limitation of flexion was found in 46 (33.6%) subjects who reported elbow pain. Tenderness of the elbow was found in 65 subjects (47.4%), and the valgus stress test was positive in 44 subjects (32.1%) who reported elbow pain (Table 1).
TABLE 1.
Outcomes of Physical Examination of Players With Elbow Pain
| n | % | |
|---|---|---|
| Limitation of extension | 32 | 23.4 |
| Limitation of flexion | 46 | 33.6 |
| Positive tenderness | 65 | 47.4 |
| Positive valgus stress test | 44 | 32.1 |
Of the 99 subjects who presented abnormal findings on physical examination, 86 (86.9%) agreed to undergo radiography. Of them, 70 (81.4%) exhibited radiographic abnormalities: medial epicondylar fragmentation in 68 subjects, and osteochondritis dissecans of the capitellum in 2 subjects.
Potential risk factors associated with elbow pain are summarized in Tables 2 and 3. Univariate analysis showed that elbow pain was significantly associated with the age of 12 years (P < .001), pitchers (P < .0001), catchers (P < .001), infielders (P = .05), and playing more than 100 games per year (P < .01) (Table 2). The number of practice days per week was not significantly associated with elbow pain. Multivariate analysis of these 5 variables showed that age of 12 years (OR, 1.91; 95% CI, 1.04-3.63), pitcher (OR, 4.27; 95% CI, 2.16-9.03), catcher (OR, 3.76; 95% CI, 1.62-9.06), and more than 100 games per year (OR, 2.62; 95% CI, 1.30-5.49) were risk factors significantly associated with elbow pain (Table 3). The infielder position was not significantly associated with elbow pain.
TABLE 2.
Univariate Analysis of the Risk Factors for Elbow Pain
| Variable | n (%) | Odds Ratio | 95% Confidence Interval | P Value |
|---|---|---|---|---|
| Age, y | ||||
| ≤10 | 99 (22.0) | 1.00 | ||
| 11 | 152 (33.9) | 1.83 | 1.00-3.47 | .06 |
| 12 | 198 (44.1) | 2.74 | 1.55-5.05 | <.001 |
| Position | ||||
| Pitcher | 149 (33.2) | 5.17 | 2.68-10.71 | <.0001 |
| Catcher | 51 (11.4) | 4.55 | 2.03-10.65 | <.001 |
| Infielder | 159 (35.4) | 2.04 | 1.03-4.30 | .05 |
| Outfielder | 90 (20.0) | 1.00 | ||
| Training days per week | ||||
| ≤3 | 85 (18.9) | 1.00 | ||
| 4-5 | 294 (65.5) | 1.46 | 0.85-2.60 | .19 |
| 6-7 | 70 (15.6) | 1.92 | 0.96-3.89 | .07 |
| No. of games per year | ||||
| ≤50 | 64 (14.2) | 1.00 | ||
| 50-69 | 150 (33.4) | 0.85 | 0.43-1.75 | .65 |
| 70-99 | 113 (25.2) | 1.59 | 0.80-3.27 | .19 |
| ≥100 | 122 (27.2) | 2.59 | 1.34-5.25 | <.01 |
TABLE 3.
Multivariate Analysis of the Risk Factors for Elbow Pain
| Variable | Odds Ratio | 95% Confidence Interval | P Value |
|---|---|---|---|
| Age, y | |||
| ≤10 | 1.00 | ||
| 11 | 1.29 | 0.68-2.53 | .44 |
| 12 | 1.91 | 1.04-3.63 | .04 |
| Position | |||
| Pitcher | 4.27 | 2.16-9.03 | <.0001 |
| Catcher | 3.76 | 1.62-9.06 | <.01 |
| Infielder | 1.85 | 0.91-3.95 | .10 |
| Outfielder | 1.00 | ||
| Training days per week | |||
| ≤3 | 1.00 | ||
| 4-5 | 1.33 | 0.74-2.46 | .36 |
| 6-7 | 1.62 | 0.78-3.43 | .20 |
| No. of games per year | |||
| <50 | 1.00 | ||
| 50-69 | 0.95 | 0.46-2.01 | .89 |
| 70-99 | 1.44 | 0.70-3.06 | .33 |
| ≥100 | 2.62 | 1.30-5.49 | <.01 |
Discussion
A total of 30.5% of youth baseball players had elbow pain. Of them, 72.3% were positive on physical examination. Furthermore, 81.4% of subjects who were positive on physical examination showed radiographic abnormalities. On the basis of these results, it is expected that approximately 30% of youth baseball players with no history of elbow pain will experience elbow pain, and that nearly 60% (72% of 81%) of players with elbow pain will show radiographic abnormalities. To our knowledge, no other surveys of this nature have been performed among youth baseball players.
The immature skeleton of a young player responds differently to the stresses of throwing than a mature skeleton. One hypothesis focuses on the secondary ossification centers.14 At the elbow, 6 ossification centers appear between the age of 2 and 11 years. The epiphysis and apophyses close slowly by ossification as the elbow becomes skeletally more mature, and ossification is complete by the mid-teen years in most children.2 It is possible for as many as 6 secondary ossification centers to be present in the elbows of 11- to 12-year-old boys. These centers are the most vulnerable points in the young elbow and can become inflamed and irritated by the throwing motion. In a study of 49 adolescent pitchers, Torg and Moyer15 found that 70% of players had soreness when pitching, but only 2 subjects presented with significant abnormal roentgenological findings. Larson et al,9 in their study of 120 Little League pitchers, found medial epicondylar changes in 23% of subjects. Furthermore, Hang et al5 found that separation or fragmentation of the medial epicondyle was present in 76% of Little Leaguers. The finding that nearly 60% of players with elbow pain in the present study exhibited radiographic abnormalities is consistent with this hypothesis.
Elbow injuries result from cumulative microtrauma from the repetitive, dynamic, overhead motion used in throwing.1,3 The slow development of these injuries makes it difficult to demonstrate cause and effect. A general perception has been that elbow injury occurs because of musculoskeletal intrinsic factors, such as the skeletal immaturity of this group and weak muscles around the elbow. Extrinsic factors, such as the level of competition, intensity of play, duration, and frequency of play, as well as the biomechanical and physiological demands of throwing, also affect the durability of young players and may increase the risk of injury.11,13
Multivariable logistic regression revealed that elbow pain was associated with age of 12 years (age of subjects taken at 1-year examination), pitcher, catcher, and more than 100 games per year.
The risk factor with the strongest association to injury was pitcher. Previous studies have confirmed that pitching is a strong risk factor for elbow pain.4,6,9 A topic of significant debate is the influence of pitch type. None of the players in our study had thrown curveballs or sliders; all had thrown fastballs or change-ups. Lyman et al10,11 showed that the use of fastball or change-up pitches is associated with a reduced risk of elbow pain, whereas the use of curveballs or sliders is associated with an increase in such risk.
In our study, catching was found to be a risk factor for elbow pain. Hang et al5 demonstrated comparatively high rates of elbow pain in youth catchers in their retrospective study, which might be explained by the fact that the number of throws made by a catcher is probably as high as that of pitchers and more than fielders.
The association with age has been well established. Older players consistently have higher rates of elbow pain than younger players.3,4 Because this increase was found for 2 to 3 years between the ages of 9 and 12 years, it may have important implications. The finding that the 12-year-olds in this study had higher rates of elbow pain than those who were 10 years old or younger supports this hypothesis.
Those who played more than 100 games per year had a notably increased risk of injury. It is not uncommon for youth players to play 70 games or more per year as the climate of the study region is warm and allows year-round baseball activity. With increasing demand on youth athletes to play more, there is less time for repair of bony and soft tissues in the elbow.
We found no association between the number of practice days per week and elbow pain, although the number of hours per week was not analyzed. Harada et al6 showed that 14 or more hours of training per week tended to be associated with elbow injuries.
This prospective study identified multiple risk factors for throwing injuries in youth baseball players and provides new information by adding to the available data. However, the study has several limitations. One major limitation is that our figures are based on the participants’ recall of practice sessions. Duration, severity, and consequences of elbow pain were not evaluated. Another disadvantage is that only children with elbow pain were evaluated clinically, and that only children with abnormal physical examination were evaluated by radiographic examination. No radiographic examinations were done for children without symptoms to serve as a control group. All players were from 1 geographic region. It is unknown whether the association between risk factors and injury are different in other countries. Finally, we did not study other potential risk factors, such as pitching mechanics and physical conditioning.
Conclusion
It is expected that 30% of youth baseball players will have elbow pain each year, and that nearly 60% of players with elbow pain will show radiographic abnormalities. Age of 12 years, playing pitcher or catcher, and playing more than 100 games per year are risk factors for elbow pain.
Acknowledgment
The authors thank Takenobu Iwase, MD, Department of Orthopaedic Surgery, Tokushima National Hospital, and Toshiyuki Iwame, MD, Department of Orthopaedic Surgery, Tokushima Prefectural Central Hospital, for their assistance in this study.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the Japanese Orthopaedic Society for Sports Medicine.
References
- 1. Andrews JR, Fleisig GS. Preventing throwing injuries. J Orthop Sports Phys Ther. 1998;27:187–188. [DOI] [PubMed] [Google Scholar]
- 2. Benjamin HJ, Briner WW., Jr Little League elbow. Clin J Sport Med. 2005;15:37–40. [DOI] [PubMed] [Google Scholar]
- 3. Grana WA, Rashkin A. Pitcher’s elbow in adolescents. Am J Sports Med. 1980;8:333–336. [DOI] [PubMed] [Google Scholar]
- 4. Gugenheim JJ, Jr, Stanley RF, Woos GW, Tullos HS. Little League survey: the Houston study. Am J Sports Med. 1976;4:189–200. [DOI] [PubMed] [Google Scholar]
- 5. Hang DW, Chao CM, Hang YS. A clinical and roentgenographic study of Little League elbow. Am J Sports Med. 2004;32:79–84. [DOI] [PubMed] [Google Scholar]
- 6. Harada M, Takahara M, Mura N, Sasaki J, Ito T, Ogino T. Risk factors for elbow injuries among young baseball players. J Shoulder Elbow Surg. 2010;19:502–507. [DOI] [PubMed] [Google Scholar]
- 7. Ireland ML, Hutchinson MR. Upper extremity injuries in young athletes. Clin Sports Med. 1995;14:533–569. [PubMed] [Google Scholar]
- 8. Kocher MS, Waters PM, Micheli LJ. Upper extremity injuries in the paediatric athlete. Sports Med. 2000;30:117–135. [DOI] [PubMed] [Google Scholar]
- 9. Larson RL, Singer KM, Bergstrom R, Thomas S. Little League survey: the Eugene study. Am J Sports Med. 1976;4:201–209. [DOI] [PubMed] [Google Scholar]
- 10. Lyman S, Fleisig GS, Andrews JR, Osinski ED. Effect of pitch type, pitch count, and pitching mechanics on risk of elbow and shoulder pain in youth baseball pitchers. Am J Sports Med. 2002;30:463–468. [DOI] [PubMed] [Google Scholar]
- 11. Lyman S, Fleisig GS, Waterbor JW, et al. Longitudinal study of elbow and shoulder pain in youth baseball pitchers. Med Sci Sports Exerc. 2001;33:1803–1810. [DOI] [PubMed] [Google Scholar]
- 12. Oberlander MA, Chisar MA, Campbell B. Epidemiology of shoulder injuries in throwing and overhead athletes. Sports Med Arthrosc Rev. 2000;8:115–123. [Google Scholar]
- 13. Olsen SJ, 2nd, Fleisig GS, Dun S, Loftice J, Andrews JR. Risk factors for shoulder and elbow injuries in adolescent baseball pitchers. Am J Sports Med. 2006;34:905–912. [DOI] [PubMed] [Google Scholar]
- 14. Pappas AM. Elbow problems associated with baseball during childhood and adolescence. Clin Orthop Relat Res. 1982;(164):30–41. [PubMed] [Google Scholar]
- 15. Torg JS, Moyer RA. Non-union of a stress fracture through the olecranon epiphyseal plate observed in an adolescent baseball player: a case report. J Bone Joint Surg Am. 1977;59:264–265. [PubMed] [Google Scholar]