

Abstract
Background:
Tunnel enlargement and coalition following double-bundle anterior cruciate ligament (ACL) reconstruction with hamstring tendon autografts has not yet been sufficiently studied.
Hypothesis:
The incidence and the degree of femoral tunnel enlargement will be significantly greater than those for tibial tunnel enlargement after anatomic double-bundle ACL reconstruction using hamstring tendon autografts. There will be no significant correlation between tunnel enlargement and coalition and the postoperative knee laxity.
Study Design:
Case series; Level of evidence, 4.
Methods:
Thirty-nine patients who underwent anatomic double-bundle ACL reconstruction using semitendinosus and gracilis tendon autografts were followed up for 1 year after surgery. The grafts were simultaneously fixed at 10° of knee flexion with EndoButtons and spiked staples. All patients were examined with computed tomography and the standard clinical evaluation methods at 2 weeks and 1 year after surgery.
Results:
The degree of tunnel enlargement of the femoral anteromedial and posterolateral tunnels averaged 10% to 11% and 7% to 9%, respectively, while that of the tibial anteromedial and posterolateral tunnels averaged 3% to 7% and 1% to 6%. The degree and incidence of the anteromedial and posterolateral tunnel enlargement were significantly greater in the femur than in the tibia (P < .0335 and P < .0405, respectively). On the femoral and tibial intra-articular surface, tunnel outlet coalition was found in 5% and 77% of the knees, respectively, at 1 year after surgery. There was no significant correlation between tunnel enlargement and coalition and the clinical outcome.
Conclusion:
The incidence and the degree of each tunnel enlargement in the femur were significantly greater than that in the tibia. However, the incidence of tunnel coalition in the femur was significantly less than that in the tibia after double-bundle ACL reconstruction with a transtibial technique. There was no significant correlation between tunnel enlargement and coalition and the clinical outcome.
Clinical Relevance:
The present study provides orthopaedic surgeons with important information on double-bundle ACL reconstruction with hamstring tendons.
Keywords: anterior cruciate ligament, clinical outcome, coalition, double-bundle reconstruction, hamstring tendon, tunnel enlargement
A number of clinical studies have reported that bone tunnel enlargement frequently occurs following single-bundle anterior cruciate ligament (ACL) reconstruction, independent of graft types and fixation methods.2 , 3 , 7 , 12 , 21 , 28 Although the relationship between tunnel enlargement and clinical results has not yet been clearly shown, the presence of large tunnels severely complicates revision ACL surgery.8 , 29 Therefore, tunnel enlargement is regarded as a significant issue in the field of ACL reconstruction. In single-bundle reconstruction, the incidence of femoral and tibial tunnel enlargement is reported to be 6% to 94% and 0% to 58%, respectively, and the majority of previous studies have reported that the incidence is higher in the femur than in the tibia.2 , 21 , 22 , 28
Recently, the clinical results of anatomic double-bundle ACL reconstruction with hamstring tendon grafts have attracted a great deal of attention13 , 18 , 30 , 32 , 33 because of biomechanical superiority compared to single-bundle reconstruction.16 , 17 , 22 , 31 However, tunnel enlargement following double-bundle ACL reconstruction with a hamstring tendon graft has not been sufficiently studied to date, and the results are inconclusive concerning the frequency of tunnel enlargement. In addition, more attention should be paid to the coalition phenomenon between the anteromedial (AM) and posterolateral (PL) tunnels in double-bundle reconstruction, because this may be one of the causes and/or results of tunnel enlargement in double-bundle ACL reconstruction. Only a few articles in the literature have evaluated tunnel coalition after double-bundle ACL reconstruction.9 , 14 , 23 , 24
Thus, the incidence of tunnel enlargement and coalition is not sufficiently clear in double-bundle ACL reconstruction, particularly when using the transtibial tunnel technique. Therefore, we have conducted a prospective follow-up study using computed tomography (CT) to determine tunnel enlargement and coalition.7 , 25 , 27 , 28 Based on previous studies, we hypothesized that the incidence and the degree of femoral tunnel enlargement will be significantly greater than tibial tunnel enlargement after anatomic double-bundle ACL reconstruction. In addition, we hypothesized that the incidence of tunnel coalition in the femur will be significantly less than that in the tibia. We believed there would be no correlation between tunnel enlargement and coalition and the postoperative knee laxity.
MATERIALS AND METHODS
Study Design
A prospective study was conducted in 2009 using patients who underwent ACL reconstruction with a hamstring tendon autograft. From 2009 to 2010, the intent was to perform double-bundle reconstruction using hamstring tendon autografts for all patients who agreed to participate in this study (after obtaining signed informed consent), to examine results with the standard clinical evaluation methods, and to take a CT scan of the knee at 2 weeks and 1 year after surgery. This clinical study design was accepted by the Institutional Review Board Clearance Committee in Hokkaido University Hospital. All patients were informed that if they did not wish to participate in this study, they could choose this procedure or single-bundle bone-patellar tendon-bone reconstruction. The diagnosis of a torn ACL was made based on a detailed history of the knee injury, physical examination, radiographs, magnetic resonance imaging (MRI), and the findings at the time of surgery. The contralateral knee in the patients was healthy and free of previous injury. Four patients with a combined ligament injury in the posterior cruciate ligament, the lateral collateral ligament, the PL corner structures of the knee, and medial collateral ligament (grade 3) were excluded from this study. In addition, patients with any previous operations for ligament injuries, a concurrent fracture, or osteoarthritis were excluded from the study. The time from onset of injury to surgery was 1 month or more.
Patient Demographics
A total of 42 patients were enrolled in this study between June 2009 and July 2010. Three patients were lost to follow-up so the remaining 39 patients (92.9%) were evaluated. There were 19 men and 20 women with a mean age of 26.4 years at the time of surgery (Table 1). The follow-up period ranged from 12 to 25 months. At the time of reconstruction, the medial or lateral meniscus was partially resected in 9 patients and repaired in 7 patients. No treatment was administered for softening or fissuring of the articular cartilage.
Table 1.
Patient Demographics (N = 39)a
| Age, y | 26.4 (12.8) |
| Male: female ratio, n | 19:20 |
| Body height, cm | 165.3 (8.2) |
| Body weight, kg | 64.3 (12.0) |
| Meniscus injury (partial resection: repair), n | 9:7 |
aValues are given as mean (standard deviation) unless otherwise indicated.
Surgical Procedure of Anatomic Double-Bundle ACL Reconstruction
The details of the anatomic procedure have been previously described32 , 33 (Figure 1). In the double-bundle procedure, the AM graft diameter ranged from 6 to 6.5 mm (mean ± standard deviation [SD], 6.3 ± 0.3 mm), and the PL graft diameter ranged from 5.5 to 6 mm (mean ± SD, 5.8 ± 0.2 mm).
Figure 1.

Schematic illustration of anatomic double-bundle anterior cruciate ligament reconstruction using hamstring tendon autografts. AM, anteromedial; PL, posterolateral.
Postoperative Management
Postoperative management was performed according to our original rehabilitation protocol.18 On the basis of the results of our previous biomechanical studies, we encouraged quadriceps and hamstring muscle training immediately after surgery.34 The static squat exercise was started 1 week postoperatively. A postoperative immobilizer was applied for 2 weeks after the operation. Full weightbearing with a hinged brace was then allowed 2 weeks after surgery. Various types of athletic training were gradually allowed after 6 weeks, although no running was allowed until 6 months after surgery. Return to full sports activity was generally permitted at 9 months after surgery.
Computed Tomography Evaluation
All patients underwent CT examination at 2 weeks and 1 year after surgery. The CT scans of the knee were taken in standard axial, sagittal, and coronal views for the purpose of measuring tunnel widening.8 , 10 , 25 The 2-dimensional (2D) and 3-dimensional (3D) CT images were taken using a 64-slice multidetector CT (Aquilion 64; Toshiba Medical Systems, Tochigi, Japan), and the images were processed using a work station (Ziostation 2; Ziosoft, Tokyo, Japan). With the knee in full extension, scanning was performed from proximal to the femoral tunnel to distal to the tibial tunnel to visualize the position of the autograft fixation. The 0.5-mm sections were secondarily reconstructed with a bony algorithm to allow multiplanar reconstructions (1-mm thickness per 1-mm interval) from the axial data set. The minimum change in tunnel diameter that can be detected reliably is 0.35 mm. Coronal reconstructions were performed to a level parallel to a line joining the posterior femoral condyles, and sagittal reconstructions were performed to a level parallel to the outer rim of the lateral femoral condyle (Figures 2 and 3). The 3D images were also reconstructed with a soft tissue algorithm using the volume-rendering technique (Figure 4).
Figure 2.

Computed tomographic images of the knee with anatomic double-bundle anterior cruciate ligament reconstruction at 2-week (top row) and 1-year (bottom row) follow-up. Sclerotic lines of the femoral anteromedial tunnel wall are enhanced in coronal (left), sagittal (center), and axial (right) views.
Figure 3.

Computed tomographic images of the knee with anatomic double-bundle anterior cruciate ligament reconstruction at 2-week (top row) and 1-year (bottom row) follow-up. Sclerotic lines of the tibial anteromedial tunnel wall are enhanced in coronal (left), sagittal (center), and axial (right) views.
Figure 4.
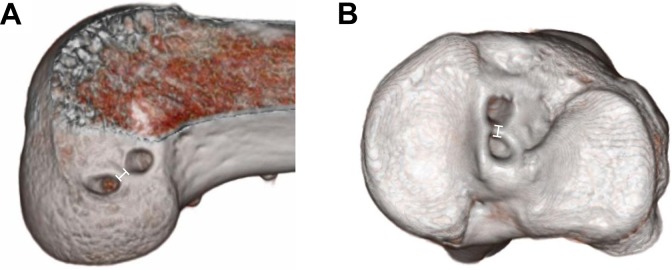
Three-dimensional computed tomography scan of (A) the femur and (B) the tibia with anatomic double-bundle anterior cruciate ligament reconstruction at 1 year after surgery.
According to previous studies,2 , 4 , 25 the tunnel measurement was taken digitally at 10 mm from the intra-articular outlet of both the femoral and the tibial tunnels in the coronal, sagittal, and axial views, respectively, perpendicular to the direction of the long axis of the tunnels (Figures 2 and 3). All measurements were taken from the sclerotic bony margins by a blinded radiologist and orthopedic surgeon. The percentage change in the diameter between the scans performed at 2 weeks and 1 year was defined as the degree of tunnel enlargement. The incidence of tunnel enlargement was determined by the number of femoral or tibial tunnels that enlarged more than 20%.
Tunnel coalition was determined by observing the AM and PL tunnel outlets on the intra-articular bone surface of the femur or the tibia using 3D CT images and measuring the width of the bony septum between the 2 tunnels, according to Hantes et al9 (Figure 4). In addition, the thickness of the bony septum between the AM and PL tunnels was measured at 10 mm from the intra-articular outlet with coronal, sagittal, and axial 2D CT images (Figure 5). When the width was zero, we defined it as tunnel coalition.
Figure 5.

The thickness of the bony septum between the anteromedial and posterolateral tunnels in (A) the femoral and (B) tibial sides measured on 2-dimensional computed tomography images at 10 mm from the intra-articular outlet.
Clinical Evaluations
Each patient underwent clinical examination 1 year after surgery. The side-to-side anterior laxity was measured using a KT-2000 arthrometer (MEDmetric, San Diego, California) at 30° of knee flexion under an anterior drawer force of 133 N. A well-trained physical therapist who was not a coauthor of this study collected the KT-2000 arthrometer results postoperatively. Another experienced orthopedic surgeon performed the pivot-shift test, the results of which were subjectively evaluated as “++,” “+,” and “−” using previously reported criteria.18 , 33 For the overall evaluation, the Lysholm knee score (maximum score, 100 points) and the International Knee Documentation Committee (IKDC) form were used.
Statistical Analysis
Intraobserver variability for tunnel measurement was satisfactory (mean intraclass correlation coefficient, 0.93; range, 0.88-0.97). An a priori power analysis was performed. A sample size was calculated to have 84% to 97% power to test the hypothesis. The Pearson correlation coefficient and the chi-square test were used to characterize the relationship of tunnel enlargement and coalition to clinical parameters. Statistical comparison was performed using the chi-square test and unpaired Student t test for the change in tunnel enlargement and coalition. A commercially available software program (StatView; SAS Institute, Cary, North Carolina) was used for statistical calculation. The significance level was set at P = .05.
RESULTS
Tunnel Position
According to the grid system,1 , 26 the mean distance between the center and the y-axis (Xc) and distance between the center and the x-axis (Yc) coordinates of the center of the AM femoral tunnel were 27.9% and 19.4%, respectively (Figure 6). The mean Xc and Yc were as follows for the center of the PL femoral tunnel: 37.7% and 53.0%, respectively; the center of the AM tibial tunnel: 39.2% and 55.8%, respectively; and the center of the PL tibial tunnel: 55.8% and 46.3%, respectively.
Figure 6.

(A) The quadrant method to evaluate the position of the femoral tunnel. A measurement grid1 was superimposed onto the intra-articular femoral tunnel outlet of the 3-dimensional computed tomographic (3D CT) image so that the superior limit of the grid was located on the femoral notch roof, and the anterior, posterior, distal, and proximal sides of the grid were located on the articular cartilage margin. An x-y coordinate system was placed on this grid, with the roof line of the intercondylar notch defined as the x-axis and the most proximal-posterior line of the grid lines perpendicular to the x-axis as the y-axis. On this coordinate system, the coordinates of the center of the anteromedial (AM) and posterolateral (PL) femoral tunnels were defined as follows: Xc, distance between the center and the y-axis; Yc, distance between the center and the x-axis. (B) The quadrant method to evaluate the position of the tibial tunnel. To analyze the center of the tunnel outlet position on the tibia, a rectangular grid was also superimposed onto the axial 3D CT image of the tibial plateau.26 The most medial-anterior corner was defined as the origin of the x-y coordinates, with the anterior line of the tibial plateau defined as the x-axis and the most medial line of the grid lines perpendicular to the x-axis defined as the y-axis. On this grid, the center of each tunnel was expressed using the above-described coordinate values (Xc, Yc). Red dots, center of the AM tunnel; blue dots, center of the PL tunnel.
Degree and Incidence of Tunnel Enlargement
The degree of tunnel enlargement (expressed as mean ± SD throughout) of the femoral AM tunnel averaged 11.1% ± 10.9%, 9.8% ± 16.5%, and 10.7% ± 13.3% in the coronal, sagittal, and axial images, respectively, while that of the femoral PL tunnel averaged 7.0% ± 11.7%, 8.9% ± 13.4%, and 7.6% ± 12.7%. The degree of tunnel enlargement of the tibial AM tunnel averaged 6.7% ± 13.0%, 3.3% ± 10.9%, and 6.1% ± 8.6% in the coronal, sagittal, and axial images, respectively, while that of the tibial PL tunnel averaged 6.4% ± 13.9%, 1.2% ± 9.8%, and 2.9% ± 9.9%. The degree of the AM tunnel enlargement was significantly greater in the femur than in the tibia (coronal: P = .0296, sagittal: P = .0226, and axial: P = .0335), while the PL tunnel enlargement was significantly greater in the femur than in the tibia only in the sagittal view (P < .0001). There was no significant correlation between the degree of each tunnel enlargement and the clinical outcome.
The incidence of the femoral AM tunnel enlargement was 20.5%, 23.1%, and 23.1% in the coronal, sagittal, and axial images, respectively, while that of the femoral PL tunnel was 12.8%, 15.4%, and 17.9%, respectively (Table 2). The incidence of the tibial AM tunnel enlargement was 2.6%, 5.1%, and 5.1% in the coronal, sagittal, and axial images, respectively, while that of the tibial PL tunnel was 7.7%, 2.6%, and 5.1%, respectively. Concerning the AM tunnel, the incidence of enlargement was significantly greater in the femur than in the tibia (coronal: P = .0227, sagittal: P = .0405, and axial: P = .0405). Regarding the PL tunnel, we found the same tendency but the difference was not significant.
Table 2.
Incidence of Tunnel Enlargement (in Percentages) at 1 Year After ACL Reconstructiona
| Femur | Tibia | P Value, Femur vs Tibia | |
|---|---|---|---|
| Coronal | |||
| AM | 20.5 | 2.6 | .0227 |
| PL | 12.8 | 7.7 | .297 |
| Sagittal | |||
| AM | 23.1 | 5.1 | .0405 |
| PL | 15.4 | 2.6 | .0717 |
| Axial | |||
| AM | 23.1 | 5.1 | .0405 |
| PL | 17.9 | 5.1 | .1178 |
aACL, anterior cruciate ligament; AM, anteromedial; PL, posterolateral.
Incidence of Tunnel Coalition
On the femoral surface, tunnel outlet coalition was found in only 1 knee (2.6% of cases) at 2 weeks and in 2 knees (5.1%) at 1 year after surgery. However, there were no knees with tunnel coalition at a level 10 mm from the bone surface at each period. In the 2 knees with outlet coalition, the postoperative knee laxity was not worse (P = .712) than the other knees. On the tibial surface, tunnel outlet coalition was observed in 22 knees (56.4% of cases) at 2 weeks and in 30 knees (76.9%) at 1 year after surgery, while tibial tunnel coalition at a level 10 mm from the joint surface was seen in 5 knees (12.8% of cases) at each period. The incidence of tunnel outlet coalition in the femur was significantly less than that in the tibia (P < .0001) 1 year after surgery. The frequency of femoral and tibial coalition did not increase significantly, and there was no significant correlation between each tunnel coalition and postoperative knee laxity.
Clinical Results
There were no graft failures at the final follow-up. All patients underwent a second surgery to remove the 2 staples that fixed the grafts onto the tibia. The postoperative side-to-side difference in anterior laxity measured with the KT-2000 arthrometer was 0.9 ± 1.6 mm (Table 3). The Lysholm knee score was 97.9 ± 2.7 points. According to the IKDC evaluation, 26, 11, and 2 patients were ranked as A, B, and C, respectively. There were no significant relationships between the clinical results and the incidence of tunnel enlargement. Also, there were no significant differences between patients with and without tibial tunnel coalition.
Table 3.
Clinical Outcome After Anatomic Double-Bundle ACL Reconstruction (N = 39)a
| Outcome Measure | |
|---|---|
| Side-to-side anterior laxity, mm, mean (standard deviation) | 0.9 (1.6) |
| Lysholm Knee score, mean (standard deviation) | 97.9 (2.7) |
| IKDC grade, No. of patients | |
| A (normal) | 26 |
| B (nearly normal) | 11 |
| C (abnormal) | 2 |
| D (severely abnormal) | 0 |
aACL, anterior cruciate ligament; IKDC, International Knee Documentation Committee.
DISCUSSION
The present study demonstrated that the degree of tunnel enlargement of the femoral AM and PL tunnels averaged 10% to 11% and 7% to 9%, respectively, while that of the tibial AM and PL tunnels averaged 3% to 7% and 1% to 6%. The incidence of enlargement in the femoral AM and PL tunnels was 21% to 23% and 13% to 18%, respectively, while enlargement incidence in the tibial AM and PL tunnels was 3% to 5% and 3% to 8%, respectively. In addition, femoral and tibial tunnel outlet coalition was found in 5% and 77%, respectively, at 1 year after surgery.
The degree and incidence of femoral tunnel enlargement were significantly greater than those of tibial tunnel enlargement after double-bundle ACL reconstruction. Siebold and Cafaltzis24 reported, using MRI, that at 7 months after double-bundle reconstruction, the degree of AM and PL femoral and tibial tunnel enlargement was in 34% and 46% and 20% and 38% of patients, respectively. Järvelä et al14 reported, using MRI, that at 27 months after double-bundle reconstruction, the degree of the AM and PL femoral and tibial tunnel enlargement was in 54% and 42% and 39% and 43% of patients, respectively. In a number of reports, enlargement was more evident for the femoral than the tibial tunnel.2 , 4 , 6 , 21 , Biomechanical and biological differences may explain why femoral tunnel enlargement was more likely to be found than tibial tunnel enlargement after double-bundle reconstruction. First, the graft in the femoral tunnel was bent, which applied a compressive force to the edge of the tunnel. In contrast, the tibial graft does not bend as much and, consequently, there is less compression and better stress distribution on the tunnel edge.11 The second potential mechanism involves the remnant tissue at the tibial insertion, which was thicker than that of the femoral insertion. This tissue may limit synovial fluid propagation within the tibial tunnel. These biomechanical and biological differences may reduce the incidence and the degree of tunnel enlargement in the tibial tunnel.
This study showed that tibial tunnel outlet coalition occurred in 56% of cases at 2 weeks and in 77% at 1 year after surgery, while the coalition at a level 10 mm from the joint surface was observed in only 13% of cases at each period. The incidence of tunnel coalition in the tibia was significantly greater than that in the femur at the joint surface. Siebold23 reported, using MRI, that tibial tunnel coalition occurred in 41% of patients at 12 months after surgery. In contrast, Hantes et al9 reported that tunnel coalition occurred intraoperatively in only 1 of 36 patients on the tibial side at the level of the joint line in double-bundle ACL reconstruction. This discrepancy in the incidence of tibial tunnel coalition may be explained by the differences in the surgical technique used. The AM tunnel angle in this series was approximately 40° in the lateral view.19 Therefore, the shape of the AM tibial tunnel outlet was oval, causing frequent overlapping of the tibial tunnels. As a result, a substantial space would exist in the proximal aspect of the tibial tunnels. This would allow transverse motion of the graft at the outlet level of the tibial tunnel when the joint is moved, throughout the range of motion. This phenomenon has been referred to as the windshield wiper effect.21
On the other hand, this study demonstrated that femoral joint surface tunnel coalition was found in only 2 knees at the 1-year examination, and there were no knees with tunnel coalition at a level 10 mm from the bone surface at each period. In these 2 knees, the cause of the coalition was considered to be an intraoperative technical error in which the 2 tunnel outlets were created too close together. In the other 95% of knees, however, the 2 femoral tunnels were created at the appropriate positions.5 These results suggest that appropriate femoral tunnels can be created using the transtibial procedure and that appropriately created femoral tunnels do not result in tunnel coalition.
This study, using CT images, demonstrated that the incidence of femoral AM and PL tunnel enlargement was 21% to 23% and 13% to 18%, respectively, and tibial AM and PL tunnel enlargement rarely occurred (3%-8%). These values appear to be lower in comparison to the previously reported data after single-bundle reconstruction.2 , 3 , 12 , 13 Previous studies14 , 15 reported that the incidence of tunnel enlargement after double-bundle reconstruction was significantly less than those after single-bundle reconstruction. However, in double-bundle reconstruction, the incidence of each tunnel enlargement was significantly greater in the femur than in the tibia. The infrequent femoral tunnel coalition may be due to the surgical technique used. The two femoral tunnels were created with a sufficiently wide bony septum between the tunnels. In a biomechanical study,20 when the width of the femoral bone bridge was extended to 2 and 3 mm, no fracture of the bony bridge could be seen after cyclic loading. Therefore, the results of this study support previously published recommendations that the tunnel should be created with a 2-mm bony septum to avoid femoral tunnel coalition in double-bundle ACL reconstruction. If 2 femoral tunnels are too closely created, there is a high probability that postoperative tunnel coalition will occur.
There are several limitations to the present study. First, we could not measure the extra-articular tunnel enlargement. Second, the follow-up period was 1 year in this study. Third, although all measurements were done by blinded examiners, they would have known CT scans are done for postoperative tunnel assessment, which could have led to a bias. In addition, we did not determine the accuracy and the interobserver variation in the CT measurement. Fourth, we used the conventional cannulated drill for tunnel creation and only hamstring tendon for the graft. Therefore, this study cannot provide any conclusion in comparison with other drill bits or grafts. However, beyond these limitations, the present study provided orthopaedic surgeons with important information on ACL reconstruction with hamstring tendons.
CONCLUSION
The present study demonstrated that both the incidence and the degree of femoral tunnel enlargement are significantly greater than those of tibial tunnel enlargement after anatomic double-bundle ACL reconstruction using hamstring tendon autografts. The incidence of tunnel coalition in the femur was significantly less than that in the tibia. In addition, the degree of tunnel enlargement does not affect the clinical outcome at the 1-year period after anatomic double-bundle ACL reconstruction.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
REFERENCES
- 1. Bernard M, Hertel P, Hornung H, Cierpinski T. Femoral insertion of the ACL. Radiographic quadrant method. Am J Knee Surg. 1997;10(1):14–21. [PubMed] [Google Scholar]
- 2. Buelow JU, Siebold R, Ellermann A. A prospective evaluation of tunnel enlargement in anterior cruciate ligament reconstruction with hamstrings: extracortical versus anatomical fixation. Knee Surg Sports Traumatol Arthrosc. 2002;10(2):80–85. [DOI] [PubMed] [Google Scholar]
- 3. Cinar BM, Akpinar S, Hersekli MA, et al. The effects of two different fixation methods on femoral bone tunnel enlargement and clinical results in anterior cruciate ligament reconstruction with hamstring tendon graft [in Turkish]. Acta Orthop Traumatol Turc. 2009;43(6):515–521. [DOI] [PubMed] [Google Scholar]
- 4. Clatworthy MG, Annear P, Bulow JU, Bartlett RJ. Tunnel widening in anterior cruciate ligament reconstruction: a prospective evaluation of hamstring and patella tendon grafts. Knee Surg Sports Traumatol Arthrosc. 1999;7(3):138–145. [DOI] [PubMed] [Google Scholar]
- 5. Edwards A, Bull AMJ, Amis AA. The attachments of the anteromedial and posterolateral fibre bundles of the anterior cruciate ligament. Part 2: femoral attachment. Knee Surg Sports Traumatol Arthrosc. 2008;16(1):29–36. [DOI] [PubMed] [Google Scholar]
- 6. Fauno P, Kaalund S. Tunnel widening after hamstring anterior cruciate ligament reconstruction is influenced by the type of graft fixation used: a prospective randomized study. Arthroscopy. 2005;21(11):1337–1341. [DOI] [PubMed] [Google Scholar]
- 7. Fink C, Zapp M, Benedetto KP, Hackl W, Hoser C, Rieger M. Tibial tunnel enlargement following anterior cruciate ligament reconstruction with patellar tendon autograft. Arthroscopy. 2001;17(2):138–143. [DOI] [PubMed] [Google Scholar]
- 8. Getelman MH, Friedman MJ. Revision anterior cruciate ligament reconstruction surgery. J Am Acad Orthop Surg. 1999;7(3):189–198. [DOI] [PubMed] [Google Scholar]
- 9. Hantes ME, Liantsis AK, Basdekis GK, Karantanas AH, Christel P, Malizos KN. Evaluation of the bone bridge between the bone tunnels after anatomic double-bundle anterior cruciate ligament reconstruction: a multidetector computed tomography study. Am J Sports Med. 2010;38(8):1618–1625. [DOI] [PubMed] [Google Scholar]
- 10. Iorio R, Vadalà A, Argento G, Sanzo VD, Ferretti A. Bone tunnel enlargement after ACL reconstruction using autologous hamstring tendons: a CT study. Int Orthop. 2007;31(1):49–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Jagodzinski M, Foerstemann T, Mall G, Krettek C, Bosch U, Paessler HH. Analysis of forces of ACL reconstructions at the tunnel entrance: is tunnel enlargement a biomechanical problem? J Biomech. 2005;38(1):23–31. [DOI] [PubMed] [Google Scholar]
- 12. Jansson KA, Harilainen A, Sandelin J, Karjalainen PT, Aronen HJ, Tallroth K. Bone tunnel enlargement after anterior cruciate ligament reconstruction with the hamstring autograft and endobutton fixation technique. A clinical, radiographic and magnetic resonance imaging study with 2 years follow-up. Knee Surg Sports Traumatol Arthrosc. 1999;7(5):290–295. [DOI] [PubMed] [Google Scholar]
- 13. Järvelä T. Double-bundle versus single-bundle anterior cruciate ligament reconstruction: a prospective, randomized clinical study. Knee Surg Sports Traumatol Arthrosc. 2007;15(5):500–507. [DOI] [PubMed] [Google Scholar]
- 14. Järvelä T, Moisala AS, Paakkala T, Paakkala A. Tunnel enlargement after double-bundle anterior cruciate ligament reconstruction: a prospective, randomized study. Arthroscopy. 2008;24(12):1349–1357. [DOI] [PubMed] [Google Scholar]
- 15. Kawaguchi Y, Kondo E, Kitamura N, Kai S, Inoue M, Yasuda K. Comparison of femoral tunnel enlargement in 169 patients between single-bundle and anatomic double-bundle anterior cruciate ligament reconstructions with hamstring tendon grafts. Knee Surg Sports Traumatol Arthrosc. 2011;19(8):1249–1257. [DOI] [PubMed] [Google Scholar]
- 16. Kondo E, Merican AM, Yasuda K, Amis AA. Biomechanical comparison of anatomic double-bundle, anatomic single-bundle, and nonanatomic single-bundle anterior cruciate ligament reconstructions. Am J Sports Med. 2011;39(2):279–288. [DOI] [PubMed] [Google Scholar]
- 17. Kondo E, Merican AM, Yasuda K, Amis AA. Biomechanical comparisons of knee stability after anterior cruciate ligament reconstruction between 2 clinically available transtibial procedures: anatomic double bundle versus single bundle. Am J Sports Med. 2010;38(7):1349–1358. [DOI] [PubMed] [Google Scholar]
- 18. Kondo E, Yasuda K, Azuma H, Tanabe Y, Yagi T. Prospective clinical comparisons of anatomic double-bundle versus single-bundle anterior cruciate ligament reconstruction procedures in 328 consecutive patients. Am J Sports Med. 2008;36(9):1675–1687. [DOI] [PubMed] [Google Scholar]
- 19. Kondo E, Yasuda K, Ichiyama H, Azuma C, Tohyama H. Radiologic evaluation of femoral and tibial tunnels created with the transtibial tunnel technique for anatomic double-bundle anterior cruciate ligament reconstruction. Arthroscopy. 2007;23(8):869–876. [DOI] [PubMed] [Google Scholar]
- 20. Lehmann AK, Osada N, Zantop T, Raschke MJ, Petersen W. Femoral bridge stability in double-bundle ACL reconstruction: impact of bridge width and different fixation techniques on the structural properties of the graft/femur complex. Arch Orthop Trauma Surg. 2009;129(8):1127–1132. [DOI] [PubMed] [Google Scholar]
- 21. L’Insalata JC, Klatt B, Fu FH, Harner CD. Tunnel expansion following anterior cruciate ligament reconstruction: a comparison of hamstring and patellar tendon autografts. Knee Surg Sports Traumatol Arthrosc. 1997;5(4):234–238. [DOI] [PubMed] [Google Scholar]
- 22. Petersen W, Tretow H, Weimann A, et al. Biomechanical evaluation of two techniques for double-bundle anterior cruciate ligament reconstruction: one tibial tunnel versus two tibial tunnels. Am J Sports Med. 2007;35(2):228–234. [DOI] [PubMed] [Google Scholar]
- 23. Siebold R. Observations on bone tunnel enlargement after double-bundle anterior cruciate ligament reconstruction. Arthroscopy. 2007;23(3):291–298. [DOI] [PubMed] [Google Scholar]
- 24. Siebold R, Cafaltzis K. Differentiation between intraoperative and postoperative bone tunnel widening and communication in double-bundle anterior cruciate ligament reconstruction: a prospective study. Arthroscopy. 2010;26(8):1066–1073. [DOI] [PubMed] [Google Scholar]
- 25. Siebold R, Kiss ZS, Morris HG. Effect of compaction drilling during ACL reconstruction with hamstring on postoperative tunnel widening. Arch Orthop Trauma Surg. 2008;128(5):461–468. [DOI] [PubMed] [Google Scholar]
- 26. Tsuda E, Ishibashi Y, Fukuda A, Yamamoto Y, Tsukada H, Ono S. Tunnel position and relationship to postoperative knee laxity after double-bundle anterior cruciate ligament reconstruction with a transtibial technique. Am J Sports Med. 2010;38(4):698–706. [DOI] [PubMed] [Google Scholar]
- 27. Vadalà A, Iorio R, De Carli A, et al. The effect of accelerated, brace free, rehabilitation on bone tunnel enlargement after ACL reconstruction using hamstring tendons: a CT study. Knee Surg Sports Traumatol Arthrosc. 2007;15(4):365–371. [DOI] [PubMed] [Google Scholar]
- 28. Webster KE, Feller JA, Hameister KA. Bone tunnel enlargement following anterior cruciate ligament reconstruction: a randomised comparison of hamstring and patellar tendon grafts with 2-year follow-up. Knee Surg Sports Traumatol Arthrosc. 2001;9(2):86–91. [DOI] [PubMed] [Google Scholar]
- 29. Wilson TC, Kantaras A, Atay A, Johnson DL. Tunnel enlargement after anterior cruciate ligament surgery. Am J Sports Med. 2004;32(2):543–549. [DOI] [PubMed] [Google Scholar]
- 30. Yagi M, Kuroda R, Nagamune K, Yoshiya S, Kurosaka M. Double-bundle ACL reconstruction can improve rotational stability. Clin Orthop Relat Res. 2007;(454):100–107. [DOI] [PubMed] [Google Scholar]
- 31. Yagi M, Wong EK, Kanamori A, Debski RE, Fu FH, Woo SL. Biomechanical analysis of an anatomic anterior cruciate ligament reconstruction. Am J Sports Med. 2002;30(5):660–666. [DOI] [PubMed] [Google Scholar]
- 32. Yasuda K, Kondo E, Ichiyama H, et al. Anatomical reconstruction of the anteromedial and posterolateral bundles of the anterior cruciate ligament using hamstring tendon grafts. Arthroscopy. 2004;20(10):1015–1025. [DOI] [PubMed] [Google Scholar]
- 33. Yasuda K, Kondo E, Ichiyama H, Tanabe Y, Tohyama H. Clinical evaluation of anatomic double-bundle anterior cruciate ligament reconstruction procedure using hamstring tendon grafts: comparisons among 3 different procedures. Arthroscopy. 2006;22(3):240–251. [DOI] [PubMed] [Google Scholar]
- 34. Yasuda K, Sasaki T. Exercise after anterior cruciate ligament reconstruction. The force exerted on the tibia by the separate isometric contractions of the quadriceps or the hamstrings. Clin Orthop Relat Res. 1987;(220):275–283. [PubMed] [Google Scholar]