

Abstract
Background:
Reconstruction of the anterior cruciate ligament (ACL) is one of the most common procedures in orthopaedic surgery. However, even with advances in surgical techniques and implants, some patients still have residual anterolateral rotatory laxity after reconstruction. A thorough study of the anatomy of the anterolateral region of the knee is needed.
Purpose:
To study the anterolateral region and determine the measurements and points of attachments of the anterolateral ligament (ALL).
Study Design:
Descriptive laboratory study.
Methods:
Dissections of the anterolateral structures of the knee were performed in 20 human cadavers. After isolating the ALL, its length, thickness, width, and points of attachments were determined. The femoral attachment of the ALL was based on the anterior-posterior and proximal-distal distances from the attachment of the lateral collateral ligament (LCL). The tibial attachment point was based on the distance from the Gerdy tubercle to the fibular head and the distance from the lateral tibial plateau. The ligaments from the first 10 dissections were sent for histological analysis.
Results:
The ALL was found in all 20 knees. The femoral attachment of the ALL at the lateral epicondyle averaged 3.5 mm distal and 2.2 mm anterior to the attachment of the LCL. Two distal attachments were observed: one inserts into the lateral meniscus, the other between the Gerdy tubercle and the fibular head, approximately 4.4 mm distal to the tibial articular cartilage. The mean measurements for the ligament were 37.3 mm (length), 7.4 mm (width), and 2.7 mm (thickness). The histological analysis of the ligaments revealed dense connective tissue.
Conclusion:
The ALL is consistently present in the anterolateral region of the knee. Its attachment to the femur is anterior and distal to the attachment of the LCL. Moving distally, it bifurcates at close to half of its length. The ALL features 2 distal attachments, one at the lateral meniscus and the other between the Gerdy tubercle and the fibular head.
Clinical Relevance:
The ALL may be important in maintaining normal rotatory limits of knee motion; ALL rupture could be responsible for rotatory laxity after isolated intra-articular reconstruction of the ACL.
Keywords: ACL, rotatory instability, anatomy, anterolateral ligament
The anterior cruciate ligament (ACL) is the most frequently injured ligament in the knee.5 In the United States, approximately 200,000 ACL reconstructions are performed each year.5,23 Historically, the first techniques for ACL reconstruction used extra-articular grafts. Subsequently, intra-articular reconstructions were performed, initially through an arthrotomy and later arthroscopically.4 More recently, there has been an emphasis on anatomic reconstruction using single- and double-bundle techniques.4
It is well known that patients diagnosed with “isolated” complete ACL tears may have different degrees of rotational laxity. ACL reconstruction may not entirely restore normal rotatory control leading to residual pathologic laxity.4 This concept was highlighted by recent research on the function of the ACL bundles and the growing popularity of more anatomic ACL reconstruction.9 Although the inability to restore normal kinematics may be because of limitations of current intra-articular techniques, lateral peripheral structure insufficiency may play a role in residual knee laxity.4,16,27
The various techniques of anatomic ACL reconstruction try to reduce rotatory laxity by placing the graft in the footprint of the original ligament. However, even without any technical flaws and proper positioning of the bone tunnels, a residual pivot-shift may be observed in approximately 7% of patients after ACL reconstruction.12,20,22 The most common cause of residual pathologic laxity is graft failure. In addition, untreated concomitant tears of the anterolateral structures may contribute to postoperative knee laxity.27 Previous and recent studies have demonstrated the importance of the iliotibial band, the anterolateral capsule, and the thickening of this capsule in limiting anterolateral rotatory laxity of the knee.14,16,17 These structures, particularly the anterolateral ligament (ALL) may be the key to restoring the normal limits of knee motion.17,29
The ALL was first described by Segond in 1879, and over more than 130 years, there were several different descriptions of this ligament but few really focused on its structure.29 Vieira et al28 previously described the anterolateral ligament in an anatomic study of the iliotibial tract.29 Even though it has already been described, the literature has not yet revealed details of the ALL measurements in relation to anatomic landmarks of the femur, and especially not quantifying the bifurcation point of the meniscal attachment.
Therefore, the aim of this study was to describe the ALL of the knee, establish its anatomic points of attachment relative to other anatomic structures in the region, determine the measurements of this ligament, and perform a histological analysis to verify that it is a ligament.
Materials and Methods
For the present study, 21 human cadaveric knees were used. This study was approved by the research ethics committee of our institution. One of the cadavers was excluded from our study because of a previous distal femur fracture, which was identified by the presence of osteosynthesis with a plate and screws and scars that indicated access through the anterolateral region of the knee. None of the human cadavers included in this study had a history of infection, previous surgery of the lower limbs, or other conditions that could alter the anatomy of the region. Of the 20 human cadavers, there were 16 males and 4 females, and we obtained 13 right knees and 7 left knees. Anthropometric measures of the cadavers are described in Table 1.
TABLE 1.
Anthropometric Measures of the Cadavers Used in Dissection
| Age, y | Weight, kg | Height, m | |
|---|---|---|---|
| Average | 61.5 | 71.0 | 1.8 |
| Standard deviation | 11.2 | 13.9 | 0.09 |
| Range | 37-67 | 40-92 | 1.53-1.86 |
The anatomic dissection was performed in a standardized manner. We initially dissected the skin and subcutaneous tissue and then performed a tenotomy of the quadriceps tendon at the myotendinous junction. The medial parapatellar retinaculum was then opened and an osteotomy of the anterior tuberosity of the tibia was performed, thus moving the patella for lateral access to the anterolateral region of the knee without violation of the adjacent extra-articular soft tissues. Part of the retropatellar fat in the region was resected for better viewing. The iliotibial tract at the Gerdy tubercle was removed, and a biceps femoris tenotomy was performed at the fibular head. The meniscotibial ligament was kept intact.
The tendon of the popliteus muscle (TPM) and the lateral collateral ligament (LCL) were isolated carefully to avoid reaching the attachment of the ALL in the region of the lateral epicondyle. The dissection of these last 2 structures was performed distal to proximal, starting at the fibular head of the LCL and following a posterior to anterior path of the ventral area of the popliteal muscle to the TPM to not violate the femoral attachment of the ALL during dissection, which could eventually alter its anatomy. With the exception of these ligaments, all of the other soft tissue structures were removed from the lateral condyle for clear visualization of the area.
After isolation of the lateral structures, clear visualization of the capsular thickening of the anterolateral region of the knee, compatible with the ALL of the knee, was possible (Figure 1).
Figure 1.
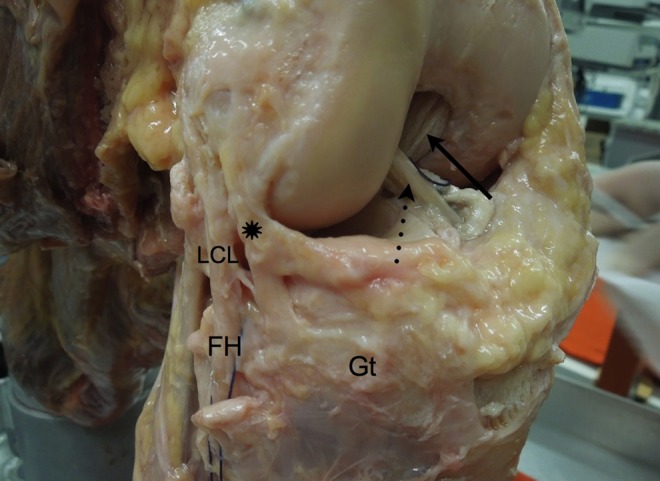
Anterolateral view of the right knee showing the anterolateral ligament (asterisk), the anterior cruciate ligament (dotted arrow), the posterior cruciate ligament (solid arrow), the fibular head (FH), the Gerdy tubercle (Gt), and the lateral collateral ligament (LCL).
All dissections were performed using the same protocol.8 After isolation and identification, the length, thickness, and width measurements were performed using a digital caliper (150 mm [6 inch] DC-60 Western, Zhejiang, China). The points of attachment were also documented. The ALL femoral attachment was based on the anterior-posterior and proximal-distal distances relative to the attachment of the LCL near the lateral epicondyle. The point of tibial attachment was based on the lateral portion of the Gerdy tubercle and the most anterior portion of the fibular head, the lateral tibial plateau cartilage, and the lateral meniscus. The bifurcation point of the ligament was measured relative to its femoral attachment, and the meniscus attachment of the ligament was measured relative to the TPM.
In 10 dissections, the ligament was removed in a block with its attachments in the femur, in the tibia, and in the meniscus and sent for histological analysis.
Results
Results are reported as averages ± standard deviations. The ALL was clearly observed in the dissections of all 20 knees studied. The attachment of the ALL in the lateral epicondyle was found anterior and distal to the attachment of the LCL, near the articular cartilage of the distal region of the lateral femoral condyle.
Observing the course of the ligament proximal to distal, a bifurcation was observed at approximately 52.5% ± 8.1% of its length. After the bifurcation, 2 notable ligament attachments were observed, one more proximal to the lateral meniscus, in the peripheral portion of the transition between the anterior horn and the body, and the other to the tibia more distal between the Gerdy tubercle and the fibular head (Figure 2).
Figure 2.
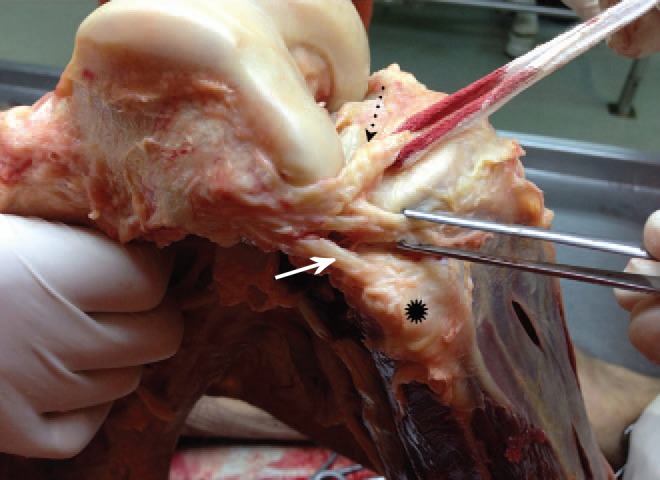
Lateral view of the right knee showing 2 notable ligament attachments, one more proximal in the lateral meniscus (dotted arrow), in the peripheral portion of the transition between the anterior horn and the body, and the other more distal between the Gerdy tubercle and the fibular head (asterisk). Lateral collateral ligament is indicated by the solid arrow.
The attachment in the anterolateral region of the knee to the meniscus occurred approximately 19.4 ± 3.5 mm anterior to the popliteus tendon, as it passes through the meniscal groove between the posterior horn and the body of the lateral meniscus. Viewing the inside of the joint, it was possible to visualize a triangular image with a distal base formed by the tibia, popliteus tendon, and the meniscal portion of the ALL (Figure 3).
Figure 3.
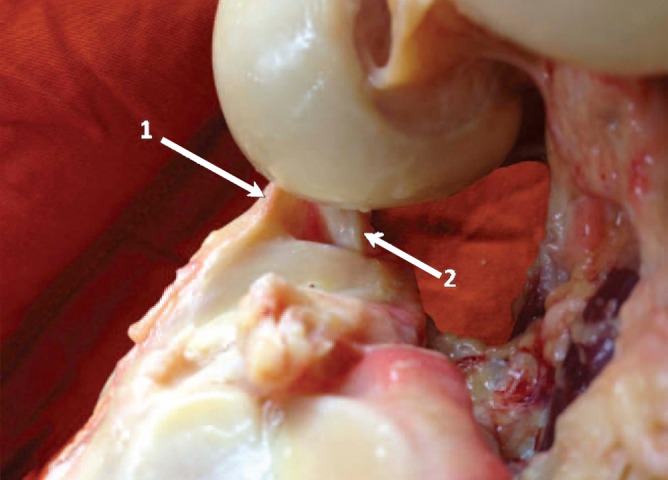
Inside view of the lateral section of the right knee showing a triangular image with a distal base formed by the tibia, popliteus tendon (2), and the meniscal portion of the anterolateral ligament (1).
The tibial attachment was found to be approximately 4.4 ± 1.1 mm from the most distal portion of the anterior articular cartilage of the proximal tibia. Considering 2 imaginary lines, one tangent to the posterior border of the Gerdy tubercle and the other tangent to the anterior border of the fibular head, the tibial attachment occurs at 38% ± 11% of the way from the fibular head to the Gerdy tubercle (Table 2).
TABLE 2.
Anatomic Locations of the Femoral, Tibial, and Meniscal Attachments of the Anterolateral Ligamenta
| Anatomic Landmark | Average | SD | Range |
|---|---|---|---|
| Femoral attachment | |||
| Anterior to the LCL, mm | 2.2 | 1.5 | 0-5 |
| Distal to the LCL, mm | 3.5 | 2.1 | 2-6 |
| Bifurcartion point from femoral attachment | |||
| Distance, mm | 20.3 | 4.1 | 14-26 |
| Percentage of total ligament length | 52.5 | 8.1 | 42-71 |
| Meniscal attachment | |||
| Anterior to the TPM, mm | 19.4 | 3.5 | 13-22 |
| Tibial attachment | |||
| Distal to the lateral plateau cartilage, mm | 4.4 | 1.1 | 2-7 |
| Between the fibular head and Gerdy tubercle, % | 38 | 11 | 22-52 |
aLCL, lateral collateral ligament; SD, standard deviation; TPM, tendon of the popliteus muscle.
The measurements found for the ligament were as follows: mean length, 37.3 ± 4.0 mm (range, 33-46 mm); mean width, 7.4 ± 1.7 mm (range, 5-11 mm); and mean thickness, 2.7 ± 0.6 mm (range, 2-4 mm).
In the histological analysis of the ligaments, the presence of dense connective tissue with arranged fibers and little cellular material was found in all specimens (Figure 4).
Figure 4.
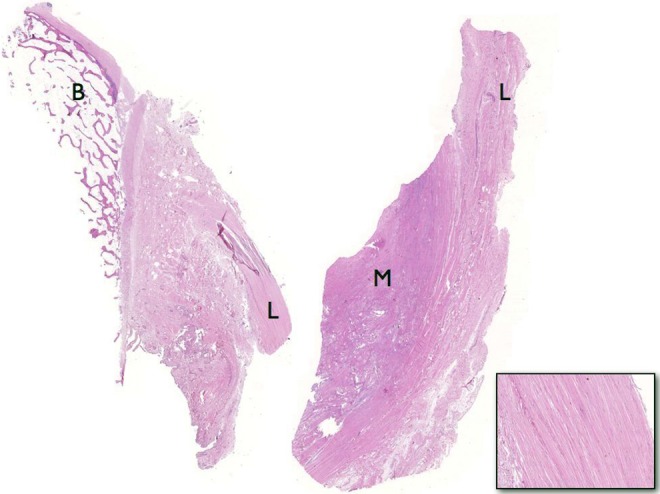
Sections of the anterolateral ligament (L) showing its well-defined femoral bone attachment (B) in the left and its meniscal attachment (M) in the right. The bottom right image shows the histological structure, with dense connective tissue, arranged fibers, and little cellular material.
Discussion
The aim of this study was to investigate the presence of a ligament structure in the anterolateral region of the knee and determine the anatomic parameters of this ligament. This line of research can be very significant because the current techniques of ACL reconstruction may not achieve normal rotatory laxity.11,12 The presence of an extra-articular structure responsible for limiting anterolateral rotatory laxity of the knee may explain why isolated intra-articular reconstructions, even when performed correctly, are not always sufficient to restore the rotatory movements of the knee.29
The importance of the anterolateral structures in ACL reconstruction was documented in the older literature, but with the emergence of intra-articular techniques, function of the ALL was thought to be less relevant to successful reconstruction.7,13 Wroble et al,30 in 1993, proved that an ACL tear associated with a lateral ligament injury would produce more external rotation than an isolated ACL tear. Terry et al,26 in 1993, concluded that injuries to the components of the iliotibial tract contributed to the variation in anterior tibial translation. Samuelson et al,21 in 1996, also showed that adding an extra-articular reconstruction to intra-articular ACL reconstruction would improve results if the patient had anterolateral ligamentous injuries. More recently, the ALL, was described by Vincent et al29 in an anatomic study. Monaco et al,17 in a biomechanical study, showed that sectioning the anterolateral structures increased internal rotation and the pivot-shift grade substantially. They found that the function of the ligament was important, and eventually, additional studies may find it to be crucial to correcting anterolateral rotatory laxity.
In our study, the ALL was found in all knees and it had similar length, width, and thickness measurements in all specimens, with values similar to recent studies.29 The attachment of the ligament to the lateral epicondyle region was similar in all specimens. The ALL from the 20 dissected knees, while presenting minor variations, had a femoral attachment that was anterior and distal to the attachment of the LCL. Contrary to previous studies, attachment was not proximal or at the same level of the LCL.8
In these cadavers, a clear bifurcation of the ligament in its path toward the tibia was observed. This can be very significant during biomechanical structural testing because the resulting 2 different attachments may have different roles in the control of rotatory laxity. The section of only one of the attachments with the preservation of the other may confound the results of biomechanical testing.
The attachment of the ALL to the lateral meniscus periphery was identified in all dissections. It was difficult to visualize a clear separation between the meniscus fibers and the attachment of the ligament. Thus, it is possible to hypothesize that the ALL may participate in the genesis of lateral meniscus tears, especially peripheral rim detachment tears. Also, lateral meniscus tears in the region of the ALL may be caused by anterolateral rotatory instability of the knee.18,19,24 Further studies are necessary to determine the biomechanical relationship between the ALL and lateral meniscus.
Visualizing the inside of the joint after dissection, with the formation of a triangle between the tibia, the TPM, and the ALL, also suggests that injury to the ALL may cause increased anterolateral rotatory laxity. The TPM restricts posterior-lateral rotatory instability, and this triangular image (Figure 3) suggests the opposite function of the ALL because the attachment points of these structures are very close together on the lateral epicondyle and apart on the tibia.6,15
The tibial attachment of the ALL was also constant and slightly posterior to half the distance between the Gerdy tubercle and the fibular head. The attachment was closer to the Gerdy tubercle in only 1 dissected case, but even in this case, the attachment was at only 52% of the distance from the fibular head. This attachment of the ALL may be associated with the Segond fracture, which is a bony avulsion from the anterolateral tibia found in approximately 9% of patients with ACL ruptures.10 This fracture is probably not caused by the iliotibial band, the anterior oblique band of the LCL, or the meniscotibial ligament, as has been reported in other studies.3,10
We found some anatomic differences in the ALL compared with the findings of Vincent et al.29 The femoral attachment was halfway between the LCL and the TPM and closer to the LCL. Neither the ligament bifurcation and its anatomic parameters nor the meniscus attachment in relation to the popliteus tendon sulcus were described by Vincent et al.29 The tibial attachment was also closer to the fibular head than the Gerdy tubercle. In the histological analysis, the finding of a well-arranged dense connective tissue confirmed the presence of a true ligament in this area not just a capsular thickening of less organized, less cellular, and less dense tissue, as previously described.25
This study of 20 human cadaveric dissections establishes the anatomic landmarks of the ALL. The main weakness of our study was the absence of a biomechanical analysis of this ligament. Our findings can serve as a guide for more precise biomechanical studies, particularly regarding the bifurcation of the ligament at approximately one-half its length, resulting in a double distal attachment. We feel that biomechanical studies should also focus on the importance of each of these bands in controlling rotation of the tibia relative to the femur.
Additional research could include the investigation of ALL injuries and posterior-lateral corner injuries to ACL tears. Further evaluation of the clinical importance of the ALL and proposals for repair and reconstruction of the ALL, as done for all other ligaments in the knee, may be indicated.1,2
Conclusion
The ALL attaches to the femur anterior and distal to the attachment of the LCL. It has a clear bifurcation at close to half of its length and 2 important distal attachments, one at the lateral meniscus and another at the Gerdy tubercle and the fibular head.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
References
- 1. Camanho GL, Bitar AC, Hernandez AJ, Olivi R. Medial patellofemoral ligament reconstruction: a novel technique using the patellar ligament. Arthroscopy. 2007;23:108.e1–108.e4. [DOI] [PubMed] [Google Scholar]
- 2. Camanho GL, Viegas AdC. Anatomic and arthroscopic study of the medial patellofemoral ligament [in Portuguese]. Acta Ortop Bras. 2003;11:145–149. [Google Scholar]
- 3. Campos JC, Chung CB, Lektrakul N, et al. Pathogenesis of the Segond fracture: anatomic and MR imaging evidence of an iliotibial tract or anterior oblique band avulsion. Radiology. 2001;219:381–386. [DOI] [PubMed] [Google Scholar]
- 4. Chambat P, Guier C, Sonnery-Cottet B, Fayard JM, Thaunat M. The evolution of ACL reconstruction over the last fifty years. Int Orthop. 2013;37:181–186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Frank RM, Verma NN. Graft selection in revision ACL reconstruction In:Bach BR, Jr, Provencher MT, eds. ACL Surgery: How to Get It Right the First Time and What to Do if It Fails. Philadelphia, PA: Elsevier; 2010:217. [Google Scholar]
- 6. Gadikota HR, Seon JK, Wu JL, Gill TJ, Li G. The effect of isolated popliteus tendon complex injury on graft force in anterior cruciate ligament reconstructed knees. Int Orthop. 2011;35:1403–1408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Garcia R, Jr, Brunet ME, Timon S, Barrack RL. Lateral extra-articular knee reconstruction: long-term patient outcome and satisfaction. J South Orthop Assoc. 2000;9:19–23. [PubMed] [Google Scholar]
- 8. Helito CP, Miyahara HS, Bonadio MB, et al. Anatomical study of the anterolateral knee ligament [in Portuguese]. Rev Bras Ortop. 2013;48:368–373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Hemmerich A, van der Merwe W, Batterham M, Vaughan CL. Knee rotational laxity in a randomized comparison of single- versus double-bundle anterior cruciate ligament reconstruction. Am J Sports Med. 2011;39:48–56. [DOI] [PubMed] [Google Scholar]
- 10. Hess T, Rupp S, Hopf T, Gleitz M, Liebler J. Lateral tibial avulsion fractures and disruptions to the anterior cruciate ligament. A clinical study of their incidence and correlation. Clin Orthop Relat Res. 1994;(303):193–197. [PubMed] [Google Scholar]
- 11. Hussein M, van Eck CF, Cretnik A, Dinevski D, Fu FH. Individualized anterior cruciate ligament surgery: a prospective study comparing anatomic single- and double-bundle reconstruction. Am J Sports Med. 2012;40:1781–1788. [DOI] [PubMed] [Google Scholar]
- 12. Hussein M, van Eck CF, Cretnik A, Dinevski D, Fu FH. Prospective randomized clinical evaluation of conventional single-bundle, anatomic single-bundle, and anatomic double-bundle anterior cruciate ligament reconstruction: 281 cases with 3- to 5-year follow-up. Am J Sports Med. 2012;40:512–520. [DOI] [PubMed] [Google Scholar]
- 13. Johnston DR, Baker A, Rose C, Scotland TR, Maffulli N. Long-term outcome of MacIntosh reconstruction of chronic anterior cruciate ligament insufficiency using fascia lata. J Orthop Sci. 2003;8:789–795. [DOI] [PubMed] [Google Scholar]
- 14. Kaplan EB. The iliotibial tract; clinical and morphological significance. J Bone Joint Surg Am. 1958;40:817–832. [PubMed] [Google Scholar]
- 15. LaPrade RF, Wozniczka JK, Stellmaker MP, Wijdicks CA. Analysis of the static function of the popliteus tendon and evaluation of an anatomic reconstruction: the “fifth ligament” of the knee. Am J Sports Med. 2010;38:543–549. [DOI] [PubMed] [Google Scholar]
- 16. Leitze Z, Losee RE, Jokl P, Johnson TR, Feagin JA. Implications of the pivot shift in the ACL-deficient knee. Clin Orthop Relat Res. 2005;(436):229–236. [DOI] [PubMed] [Google Scholar]
- 17. Monaco E, Ferretti A, Labianca L, et al. Navigated knee kinematics after cutting of the ACL and its secondary restraint. Knee Surg Sports Traumatol Arthrosc. 2012;20:870–877. [DOI] [PubMed] [Google Scholar]
- 18. Musahl V, Citak M, O’Loughlin PF, Choi D, Bedi A, Pearle AD. The effect of medial versus lateral meniscectomy on the stability of the anterior cruciate ligament-deficient knee. Am J Sports Med. 2010;38:1591–1597. [DOI] [PubMed] [Google Scholar]
- 19. Petrigliano FA, Musahl V, Suero EM, Citak M, Pearle AD. Effect of meniscal loss on knee stability after single-bundle anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2011;19(suppl 1):86–93. [DOI] [PubMed] [Google Scholar]
- 20. Piefer JW, Pflugner TR, Hwang MD, Lubowitz JH. Anterior cruciate ligament femoral footprint anatomy: systematic review of the 21st century literature. Arthroscopy. 2012;28:872–881. [DOI] [PubMed] [Google Scholar]
- 21. Samuelson M, Draganich LF, Zhou X, Krumins P, Reider B. The effects of knee reconstruction on combined anterior cruciate ligament and anterolateral capsular deficiencies. Am J Sports Med. 1996;24:492–497. [DOI] [PubMed] [Google Scholar]
- 22. Scheffel PT, Henninger HB, Burks RT. Relationship of the intercondylar roof and the tibial footprint of the ACL: implications for ACL reconstruction. Am J Sports Med. 2013;41:396–401. [DOI] [PubMed] [Google Scholar]
- 23. Siegel L, Vandenakker-Albanese C, Siegel D. Anterior cruciate ligament injuries: anatomy, physiology, biomechanics, and management. Clin J Sport Med. 2012;22:349–355. [DOI] [PubMed] [Google Scholar]
- 24. Tanaka M, Vyas D, Moloney G, Bedi A, Pearle A, Musahl V. What does it take to have a high-grade pivot shift? Knee Surg Sports Traumatol Arthrosc. 2012;20:737–742. [DOI] [PubMed] [Google Scholar]
- 25. Terry GC, Hughston JC, Norwood LA. The anatomy of the iliopatellar band and iliotibial tract. Am J Sports Med. 1986;14:39–45. [DOI] [PubMed] [Google Scholar]
- 26. Terry GC, Norwood LA, Hughston JC, Caldwell KM. How iliotibial tract injuries of the knee combine with acute anterior cruciate ligament tears to influence abnormal anterior tibial displacement. Am J Sports Med. 1993;21:55–60. [DOI] [PubMed] [Google Scholar]
- 27. Vadala AP, Iorio R, De Carli A, et al. An extra-articular procedure improves the clinical outcome in anterior cruciate ligament reconstruction with hamstrings in female athletes. Int Orthop. 2013;37:187–192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Vieira EL, Vieira EA, da Silva RT, Berlfein PA, Abdalla RJ, Cohen M. An anatomic study of the iliotibial tract. Arthroscopy. 2007;23:269–274. [DOI] [PubMed] [Google Scholar]
- 29. Vincent JP, Magnussen RA, Gezmez F, et al. The anterolateral ligament of the human knee: an anatomic and histologic study. Knee Surg Sports Traumatol Arthrosc. 2012;20:147–152. [DOI] [PubMed] [Google Scholar]
- 30. Wroble RR, Grood ES, Cummings JS, Henderson JM, Noyes FR. The role of the lateral extraarticular restraints in the anterior cruciate ligament–deficient knee. Am J Sports Med. 1993;21:257–262. [DOI] [PubMed] [Google Scholar]