

Abstract
Background:
Men’s ice hockey allows for body checking, and women’s ice hockey prohibits it. Studies have reported injury data on both sexes, but no systematic reviews have compared the injury patterns between male and female ice hockey players.
Hypothesis:
Men’s and women’s ice hockey would have different types of injuries, and this difference would extend across the different age groups and levels of play.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
Three databases, 3 scientific journals, and selected bibliographies were searched to identify articles relevant to this study. Articles were further screened by the use of predetermined inclusion and exclusion criteria. Twenty-two studies met these criteria and were subsequently reviewed.
Results:
Men sustained higher rates of injuries than women at all age levels, and both sexes sustained at least twice as many injuries in games than practices. Both sexes sustained most of their injuries from player contact. Men and women in college sustained most injuries to the head and face, and women suffered from higher percentages of concussion. At all ages and levels of play, men had higher rates of upper extremity injuries (shoulder), while women were found to sustain more injuries to the lower extremity (thigh, knee).
Conclusion:
Although findings showed men sustaining higher rates of injuries than women, the predominant mechanism of player contact was the same. The most common locations and types of injuries in female ice hockey players are comparable to other sports played by women, and similar interventions could offer protection against injury.
Clinical Relevance:
Further studies that report injury data for women playing ice hockey at all levels will assist in understanding what prevention strategies should be implemented.
Keywords: ice hockey, head injuries, facial injuries, female athlete
Men’s hockey has steadily gained popularity and support over the years, while women’s hockey experienced a period of dormancy until the 1960s. Currently, ice hockey is one of the fastest growing women’s sports in the world, with the number of participants increasing more than 400% in the past 10 years, according to the United States Department of Commerce. In 1998, women’s ice hockey was added to the Winter Olympics, and leagues are now available at every level of competition.16
The fast-paced, physical nature of ice hockey would suggest high rates of player injury. Rare instances of life-threatening and disabling injuries have also drawn attention to player safety and injury prevention. Types and mechanisms of player injury have become a focus for clinical research, with hopes of the modification of rules, equipment, and penalties, along with insights for safety education. Full facial protection has offered a significantly higher level of protection against facial injuries and lacerations than half facial protection or no facial protection.4 A recent decline in spinal injuries in Canadian hockey may be related to improved education about injury prevention and specific rules against checking from behind.4,35
The most significant difference between men’s and women’s ice hockey is the allowance of body checking. Body checking can be a useful maneuver in ice hockey, but it is also one of the most common causes of injury.11 It is not permitted in any women’s leagues, and it is allowed in men’s leagues depending on the age group and level of competition. The Canadian Hockey Association recommends body checking be permitted at age 12 years and older, but several provinces allow body checking in players as young as 10 years. The American Academy of Pediatrics recommends body checking be permitted at age 15 years, but North American youth league rules vary based on geographic location.21
Men’s and women’s ice hockey injuries have been described in the literature. A majority of these studies focus on men, but recently more attention has shifted to women’s injuries. However, there have been relatively few studies that have examined sex and injury.2,8,10,12,20,29,30 All these studies have been restricted to one level of play. The present systematic review was conducted to determine the different injury rates and patterns within men’s and women’s ice hockey across several levels ranging from youth boys and girls to collegiate players. Our hypothesis was that men’s and women’s ice hockey would have different types of injuries and injury rates and that these differences would extend across the different age groups and levels of play.
Materials and Methods
Three electronic databases and 3 electronic journals were searched using a combination of terms to identify potentially relevant articles (Table 1). Bibliographies of selected articles were hand-searched to identify additional articles that were not identified by the below search strategy.
TABLE 1.
Search Strategya
| Source | Search Terms | No. of Citations Found |
|---|---|---|
| PubMed | Hockey Injuries | 768 |
| Ice Hockey AND Injuries AND Incidence | 338 | |
| Hockey AND Injuries AND Women | 242 | |
| Women’s AND Hockey | 52 | |
| Men’s AND Hockey | 33 | |
| SPORTDiscus | Ice Hockey Injuries | 602 |
| CINAHL | Hockey Injuries | 393 |
| The American Journal of Sports Medicine | Hockey Injuries | 5737 |
| Clinical Journal of Sport Medicine | Hockey Injuries | 218 |
| British Journal of Sports Medicine | Hockey Injuries | 3717 |
aAll searches were conducted in February 2012.
Titles and abstracts of the identified citations were screened to identify all potentially relevant citations. If the abstract was insufficient or unavailable, the full article text was read to determine its relevance.
The following predetermined inclusion criteria were used to select relevant studies: (1) original data (case series, case controls, prospective cohorts, randomized controlled trials); (2) injuries sustained in the sport of ice hockey; (3) male or female athletes of any age; (4) data that were separated based on sex; (5) athletes participating at the youth, adolescent, and collegiate level; (6) data that report all injuries; and (7) English language. Exclusion criteria were as follows: (1) data on sports other than ice hockey, including field hockey; (2) hockey data compiled with other sports data; (3) data exclusively on 1 type of injury; (4) compiled male and female data; (5) data exclusively on 1 type of mechanism (eg, body checking); (6) case reports, review articles, commentaries, letters to the editor; (7) studied prevention and treatment of injuries; and (8) non–English language. Twenty-two studies met these criteria and were subsequently reviewed by all 3 authors. The study selection followed guidelines set by the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement (Figure 1).23
Figure 1.
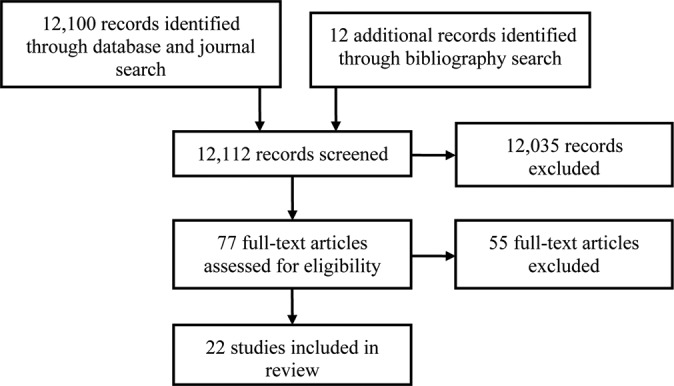
Study selection based on the PRISMA flowsheet.
Results
The majority of studies described men’s injuries. Of the 22 studies, only 6 studies included data for women’s injuries. Data from all 22 studies were extracted. The results were summarized by injury incidence, location, type, and mechanism.
Injury Incidence
Men have experienced higher rates of injury than women at all levels of play and regardless of the allowance of body checking (Tables 2 and 3). Studies on youth and adolescent players reported variable data. Boys averaged 36.45 injuries/1000 hours (range, 1-117.3 injuries/1000 hours) and girls averaged 34.54 injuries/1000 hours (range, 2.62-50.5 injuries/1000 hours). In the 3 most comparative adolescent reports that kept all variables constant, injuries were twice more common in boys than in girls.8,12,29 There was a much smaller difference between sexes in collegiate injury rates than at the youth and adolescent level. In one of the comparative studies, men only suffered from 1.42 more injuries than women per 1000 exposures.30
TABLE 2.
Injury Rates in Male Ice Hockey Playersa
| Study (Year) | Age or Level | Injury Rate | ||
|---|---|---|---|---|
| Practice | Game | Overall | ||
| Emery and Meeuwisse (2006)12 | 8-17 y | 4.15/1000 h | ||
| Stuart et al (1995)33 | 9-10 y | 1.1/1000 h | 0 | 1.0/1000 h |
| 11-12 y | 2.2/1000 h | 0 | 1.8/1000 h | |
| 13-14 y | 2.5/1000 h | 10.9/1000 h | 4.3/1000 h | |
| Brust et al (1992)7 | 9-15 y | 1/44 h | 1/7 h | |
| Brust et al (1998)8 | 11-14 y | 106.4/1000 h | ||
| Roberts et al (1999)29 | 11-19 y | 117.3/1000 h | ||
| Gerberich et al (1987)15 | 14-18 y | 5.0/1000 h | ||
| Park and Castaldi (1980)24 | 15-19 y | 1.57/game | ||
| Pinto et al (1999)26 | 16-20 y | 4/1000 h | 83/1000 h | |
| Stuart and Smith (1995)31 | 17-20 y | 3.9/1000 h | 96.1/1000 h | 9.4/1000 h |
| McKnight et al (1992)22 | College | 2.5/1000 AE | 14.7/1000 AE | 10.22/1000 AE |
| Rielly (1982)27 | College | 78.7/1000 h | ||
| Flik et al (2005)14 | College | 2.2/1000 AE | 13.8/1000 AE | |
| Agel et al (2007)2 | College | 1.96/1000 AE | 16.27/1000 AE | |
| Rishiraj et al (2009)28 | College | 1.1/1000 AE | 8.2/1000 AE | |
| Schick and Meeuwisse (2003)30 | College | 9.19/1000 AE | ||
| Pelletier et al (1993)25 | College | 19.95/1000 player-games | ||
aAE, athlete-exposure.
TABLE 3.
Injury Rates in Female Ice Hockey Playersa
| Study (Year) | Age or Level | Injury Rate | ||
|---|---|---|---|---|
| Practice | Game | Overall | ||
| Brust et al (1998)8 | 8-14 y | 50.5/1000 h | ||
| Emery and Meeuwisse (2006)12 | 8-17 y | 2.62/1000 h | ||
| Decloe et al (2013)10 | 9-17 y | 1.1/1000 h | 2.3/1000 h | 1.9/1000 h |
| Roberts et al (1999)29 | 11-19 y | 50.5/1000 h | ||
| Schick and Meeuwisse (2003)30 | College | 7.77/1000 AE | ||
| Agel et al (2007)1 | College | 2.5/1000 AE | 12.6/1000 AE | |
aAE, athlete-exposure.
Both men and women sustained at least twice as many injuries during games than in practices.1,7,10,14,22,26,28,31 For men and women, youth and adolescent rates are often reported per 1000 hours and are difficult to compare with college rates, which have been mostly reported per 1000 athlete-exposures.
Injury Location
Men playing at all ages and levels suffered injuries primarily to the head and face, shoulder, and knee. Only 1 study reported data on location of injury in youth and adolescent women and found that all injuries were sustained to the trunk and lower extremity. Women in college suffered from higher rates of head and face injuries than men, and they also sustained high numbers of knee, thigh, and ankle injuries (Table 4).
TABLE 4.
Injury Location in Ice Hockey Playersa
| Age or Level | Anatomic Location of Injury, % | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Head | Upper Extremity | Trunk | Lower Extremity | |||||||||||||||
| Head, Face | Neck | Shoulder | Upper Arm | Elbow | Forearm | Wrist | Hand | Ribs | Abdomen | Back | Hip, Groin | Thigh | Knee | Lower Leg | Ankle | Foot | ||
| Men’s studies | ||||||||||||||||||
| Sutherland (1976)34 | 5-14 y | 58.7 | — | 5.9 | — | — | — | — | 5.9 | — | — | — | — | 5.9 | 23.5 | — | — | — |
| 14-18 y | 68.2 | — | 2.4 | — | — | — | — | — | — | — | 4.9 | 4.9 | 4.9 | 4.9 | 2.4 | — | — | |
| Stuart et al (1995)33 | 9-14 y | 7 | 7 | 22 | 22 | — | — | 14 | — | 7 | — | 7 | 7 | — | — | 7 | ||
| Brust et al (1992)7 | 9-15 y | 13.6 | 9.7 | 12 | 3.9 | 5.8 | — | 2 | 7.8 | 25 | 3.9 | — | 9.7 | 2.9 | 3.9 | — | ||
| Björkenheim et al (1993)5 | 9-18 y | 10 | — | 55 | 13 | 19 | ||||||||||||
| Brust et al (1998)8 | 11-14 y | 40 | 20 | 20 | 20 | |||||||||||||
| Gerberich et al (1987)15 | 14-18 y | 19 | 3 | 16 | 13 | 6 | 2 | 5 | 4 | — | 10 | 11 | 5 | — | ||||
| Park and Castaldi (1980)24 | 15-19 y | 27.6 | 4.8 | — | 4.8 | 7.2 | 4.8 | 1.2 | 0 | 4.8 | 14.4 | 6 | 13.3 | 1.2 | 3.6 | 1.2 | ||
| Pinto et al (1999)26 | 16-20 y | 24.2 | 6.7 | 12.1 | 1.3 | 4 | 1.3 | 1.4 | 9.4 | 2.7 | — | 4 | 5.4 | 12.1 | 6.7 | 1.3 | 1.4 | 1.3 |
| Stuart and Smith (1995)31 | 17-20 y | 28 | — | 20 | — | 2 | — | 1 | 5 | 2 | 1 | 7 | 14 | 4 | 6 | 1 | 4 | 5 |
| Hayes (1975)18 | College | 45 | 9 | 8 | 9 | 3 | 5 | 10 | 2 | 8 | ||||||||
| Rielly (1982)27 | College | 34.5 | 14.4 | 0 | 3.9 | 0.9 | 9.6 | 0 | 2.9 | 10.6 | 13.6 | 9.6 | ||||||
| Flik et al (2005)14 | College | 19 | 15 | — | — | — | 7 | — | — | 9 | 9 | 22 | 12 | |||||
| Sutherland (1976)34 | College | 26.6 | — | 13.3 | — | 3.3 | — | 3.3 | — | — | — | — | 26.6 | — | 10 | — | 6.7 | 10 |
| Agel et al (2007)2 | College | 13.9 | 31.6 | 17.9 | 34.8 | |||||||||||||
| Pelletier et al (1993)25 | College | 27.6 | 14.9 | 3.7 | 6.9 | 4.8 | 6.4 | 9 | 18.6 | 1.1 | 3.2 | 1.6 | ||||||
| Rishiraj et al (2009)28 | College | 40 | 11 | 12 | — | — | 4 | 4 | — | 8 | — | 12 | ||||||
| Schick and Meeuwisse (2003)30 | College | 14.3 | 0.6 | 14.9 | 1.9 | 1.2 | — | 5 | 5.6 | 1.9 | — | 10.6 | 3.7 | 16.8 | 14.9 | 0.6 | 5 | — |
| McKnight et al (1992)22 | College | 1.13b | 1.86b | 1.20b | 0.73b | — | — | 1.06b | 1.02b | 1.61b | 0.77b | 0.84b | — | |||||
| Women’s studies | ||||||||||||||||||
| Brust et al (1998)8 | 8-14 y | — | — | — | — | — | — | — | — | 50 | 50 | |||||||
| Schick and Meeuwisse (2003)30 | College | 16.7 | 3 | 7.6 | 3 | — | — | 4.5 | — | 4.5 | — | 10.6 | 1.5 | 16.7 | 15.1 | 3 | 12.1 | — |
| Agel et al (2007)1 | College | 21.8 | 27.2 | 17.2 | 31.5 | |||||||||||||
aAnatomic location expressed as percentages unless otherwise indicated. A dash indicates this injury site was not reported in the study; values in shaded areas are shared by multiple injury sites as shown.
bPer 1000 athlete-exposures.
Injury Type
Different types of injuries were seen in men and women at different ages (Table 5). Youth and adolescent boys suffered mostly from contusions, which on average accounted for 38% of injuries. Boys also sustained significant numbers of strains and sprains (17%) and fractures (13%). Girls also suffered from mostly contusions (58%) and strains (14%). In college men and women, one third of injuries were strains and sprains. The next most common types of injuries were concussions (17%) in women and contusions (14%) and lacerations (13%) in men.
TABLE 5.
Injury Type in Ice Hockey Playersa
| Age or Level | Type of Injury | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Strain | Sprain | Dislocation | Separation | Concussion | Contusion | Laceration | Fracture | ||
| Men’s studies | |||||||||
| Stuart et al (1995)33 | 9-14 y | 21 | — | — | — | 36 | 7 | 29 | |
| Brust et al (1992)7 | 9-15 y | 13 | 6 | 4 | — | — | 50 | 2 | 8 |
| Björkenheim et al (1993)5 | 9-18 y | 16 | 2 | — | — | 47 | 3 | 25 | |
| Brust et al (1998)8 | 11-14 y | — | 10 | — | — | — | 65 | — | 5 |
| Gerberich et al (1987)15 | 14-18 y | 14 | 3 | 6 | 12 | 29 | 13 | 11 | |
| Park and Castaldi (1980)24 | 15-19 y | 9.6 | 10.9 | — | — | — | 45.8 | 9.6 | 2.4 |
| Hastings et al (1974)17 | 15-21 y | — | 8 | 2 | — | 5 | 23 | 27 | 20 |
| Pinto et al (1999)26 | 16-20 y | — | 36.3 | — | 1.3 | 28.2 | 16.1 | 6.7 | |
| Stuart and Smith (1995)31 | 17-20 y | 25 | 16 | — | — | — | 18 | 24 | 8 |
| Rielly (1982)27 | College | 6.7 | 7.7 | — | 9.6 | 5.7 | 19.4 | 28.9 | 14.4 |
| Agel et al (2007)2 | College | 13.4 | 22.5 | 3.2 | 7.6 | 7.9 | 13.2 | 1.1 | 1.7 |
| Pelletier et al (1993)25 | College | 11.3 | 31 | — | 7.5 | 21 | 13 | 10.2 | |
| Rishiraj et al (2009)28 | College | 20 | 20 | — | 1 | 13 | 12 | 11 | 8 |
| Schick and Meeuwisse (2003)30 | College | 12.5 | 21.2 | 1.9 | — | 10.6 | 6.8 | — | 2.5 |
| McKnight et al (1992)22 | College | 1.50b | 3.03b | 033b | — | — | 3.32b | 0.91b | 0.58b |
| Women’s studies | |||||||||
| Brust et al (1998)8 | 8-14 y | — | — | — | — | — | 100 | — | — |
| Decloe et al (2013)10 | 9-17 y | 28.3 | 16.9 | 5.7 | — | 15.1 | 16.9 | — | 3.8 |
| Schick and Meeuwisse (2003)30 | College | 18.1 | 18.2 | 3 | — | 15.1 | 1.5 | — | — |
| Agel et al (2007)1 | College | 11.1 | 13.7 | 3.5 | 4.2 | 18.3 | 4.4 | — | — |
aType of injury expressed as percentages unless otherwise indicated. A dash indicates this type was not reported in the study; values in shaded areas are shared by multiple injury types as shown.
bPer 1000 athlete-exposures.
Injury Mechanism
Ice hockey players of both sexes sustained most of their injuries from player contact (Table 6). In college, player contact accounted for almost half of all injuries for both men and women. Player contact as the mechanism of injury in adolescent boys ranged from 12% to 48%, while the 1 study on girls reported that 58% of injuries were caused by player contact.
TABLE 6.
Injury Mechanism in Ice Hockey Playersa
| Age or Level | Mechanism of Injury | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Player Contact | Ice | Boards | Stick | Puck | Skate | Goal | Noncontact | ||
| Men’s studies | |||||||||
| Stuart et al (1995)33 | 9-14 y | 21 | 7 | 29 | 7 | 14 | 7 | — | 14 |
| Björkenheim et al (1993)5 | 9-18 y | 44 | — | 5 | 23 | 25 | — | — | — |
| Gerberich et al (1987)15 | 14-18 y | 34.8 | 8 | 19.8 | — | 7.5 | — | 19.8 | 4.8 |
| Park and Castaldi (1980)24 | 15-19 y | 48 | — | — | 12 | 17 | — | — | — |
| Hastings et al (1974)17 | 15-21 y | 12 | 11 | 17 | 41 | 11 | 3 | — | — |
| Pinto et al (1999)26 | 16-20 y | 12.2 | 12.2 | — | 16.2 | 8.1 | 2.7 | — | 13.5 |
| Stuart and Smith (1995)31 | 17-20 y | 24 | — | 22 | 14 | 11 | 3 | — | 6 |
| Hayes (1975)18 | College | 38 | 14 | — | 29 | 3 | 15 | — | — |
| Rielly (1982)27 | College | 43.3 | — | — | 14.4 | — | 27 | — | 9.6 |
| Flik et al (2005)14 | College | 36.3 | 6 | 18.6 | 1.8 | 3.5 | 6.2 | 2.7 | 9 |
| Agel et al (2007)2 | College | 44.7 | 37.6 | — | |||||
| Pelletier et al (1993)25 | College | 97.9 | 2.2 | ||||||
| Schick and Meeuwisse (2003)30 | College | 38.37 | — | 38.05 | 12.79 | — | 12.79 | 21 | |
| Rishiraj et al (2009)28 | College | 0.89b | 0.95b | 0.56b | — | 1.30b | |||
| McKnight et al. (1992)22 | College | 4.20b | 1.97b | 0.58b | — | 0.99b | 0.11b | — | |
| Women’s studies | |||||||||
| Decloe et al (2013)10 | 9-17 y | 58 | 15 | 20 | |||||
| Schick and Meeuwisse (2003)30 | College | 48.39 | — | 41.94 | — | — | 9.68 | 4 | |
| Agel et al (2007)1 | College | 37.20 | 39.40 | 22.60 | |||||
aMechanism of injury expressed as percentages unless otherwise indicated. A dash indicates this mechanism was not reported in the study; values in shaded areas are shared by multiple injury mechanisms as shown.
bPer 1000 athlete-exposures.
Discussion
This study represents the first attempt to systematically review and compare the literature on male and female ice hockey injuries. During the 1980s, the number of women participating in organized amateur hockey leagues in Canada almost tripled.13 In female ice hockey, intentional body checking is prohibited. One would suspect that this difference in rules would lead to a different pattern of injuries, and many people believe that women’s hockey is safer because of the rule against checking.13 We found that men experienced higher rates of injuries than women at all age levels; however, most injuries were caused by player contact regardless of sex.
Men suffered from higher rates of injuries than women, which is consistent with the theory that the difference in rules has an impact on player safety. Despite this finding, most injuries in men and women were because of player contact, suggesting that women’s hockey is still a very physical game in spite of no-checking rules. The high percentage of injuries caused by player contact likely explains the significantly higher injury rates in both sexes during games compared with practices. Some practice time is spent on noncontact skills such as skating and stick handling, so there is more contact per hour during games. In studies conducted by Agel et al,1,2 game injury rates were 5 and 8 times higher than practice injury rates in women and men, respectively. Since player contact was found to be the leading mechanism for injuries, further research is needed to see how the sport itself, or checking specifically, affects the player contact mechanism and specific types of injuries.
Men and women both sustained a majority of the injuries to the head and face, which on average accounted for 29% and 17% of injuries, respectively. This finding may reflect changes in safety equipment over the years. Several of the men’s studies were conducted in the 1970s, before the mandatory use of a helmet, and the percentages of head and face injuries are disproportionately high when compared with more recent studies included in our review. Also, the mandatory use of full facial protection for athletes across many age groups has increased over the past decades, and it has significantly reduced the number of facial and ocular injuries.32 The 3 most recent studies comparing men’s and women’s injuries found higher rates of head and face injuries in women.1,2,30 In 2012, Brainard et al6 found that although women have been found to have a higher incidence of concussion, female players sustain fewer impacts.
Extremity injury patterns differed between men and women. Men sustained the highest percentage of injuries to the shoulder (13%), and women sustained more injuries to the thigh (17%) and knee (15%). The higher number of injuries to the upper extremity in men is most likely because of the allowance of body checking in men’s leagues. The higher incidence of injuries to the lower extremity in women is consistent with studies that have found similar results in women compared with men in other sports, including soccer and basketball.3 Herman et al19 found that the incorporation of neuromuscular warm-up strategies led to a decrease in lower extremity injuries in female soccer and basketball players. Future research could investigate whether similar strategies could be implemented to reduce incidence of injury in female ice hockey players.
Concussions were also noted to have a gender difference in injury distribution. Concussions accounted for 17% of the injuries sustained by women versus 8% in men. Similarly, Daneshvar et al9 found higher rates of concussion in female athletes compared with male athletes participating in high school and collegiate soccer and basketball. Specific training on safely absorbing contact could help improve rates of concussion in women. Further research is needed to evaluate the type of player contact that results in most concussions and whether it is contact with the ice, boards, or another player. A better understanding of the context in which these concussions occur can lead to the development of equipment and helmets that are more specific for women.
Several limitations exist that made a comparison of studies difficult. The method of data collection varied between studies. Many studies had physicians record injuries, players reported their own injuries in some studies, and other studies relied on records from insurance claims. The definition of the outcome variable (injury) differed between studies. Some studies defined an injury as any event that an athlete sought care for, while others only considered an incident an injury if it led to time loss. The description of injury rate varied among studies. A majority of studies reported injuries per 1000 hours, but several studies reported injuries per athlete-exposure or per game. A few studies did not report any standardized injury rate. Finally, no studies have reported injury data on women’s professional ice hockey players. The eligible studies on men’s professional ice hockey injuries have nothing to be compared with at this time.
Men and women have different rates of injury but player contact is the mechanism that predominates. Further studies on women’s ice hockey injuries are needed to gain a better understanding of what measures could improve their safety. Currently, there are no data available on the number of women who receive training on how to safely absorb contact or how the occurrence of training affects their injury rates. Data on these topics can provide insight on a potentially cost-effective way to prevent injury in women and acknowledge the physicality of their type of play.
Conclusion
With increasing numbers of women playing ice hockey, it is important to continually evaluate the injury mechanisms and patterns between the sexes. Although we found that men sustained higher rates of injuries than women, the predominant mechanism of player contact was the same despite different rules. This finding provides evidence that women would receive as much benefit as men from spending time and training on safely absorbing contact. The most common locations and types of injuries in female ice hockey players are comparable to other sports played by women, and similar interventions could offer protection against injury. Further studies that report injury data for women playing ice hockey at all levels will assist in understanding what prevention strategies should be implemented.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: D.C.F. is a consultant for Sanofi and Smith & Nephew.
References
- 1. Agel J, Dick R, Nelson B, Marshall S, Dompier T. Descriptive epidemiology of collegiate women’s ice hockey injuries: National Collegiate Athletic Association Injury Surveillance System, 2000-2001 through 2003-2004. J Athl Train. 2007;42:249–254. [PMC free article] [PubMed] [Google Scholar]
- 2. Agel J, Harvey E. A 7-year review of men’s and women’s ice hockey injuries in the NCAA. Can J Surg. 2010;53:319–323. [PMC free article] [PubMed] [Google Scholar]
- 3. Arendt E, Dick R. Knee injury patterns among men and women in collegiate basketball and soccer. NCAA data and review of literature. Am J Sports Med. 1995;23:694–701. [DOI] [PubMed] [Google Scholar]
- 4. Asplund C, Bettcher S, Borchers J. Facial protection and head injuries in ice hockey: a systematic review. Br J Sports Med. 2009;43:993–999. [DOI] [PubMed] [Google Scholar]
- 5. Björkenheim J, Syvahuoko I, Rosenberg P. Injuries in competitive junior ice-hockey: 1437 players followed for one season. Acta Orthop Scand. 1993;64:459–461. [DOI] [PubMed] [Google Scholar]
- 6. Brainard LL, Beckwith JG, Chu JJ, et al. Gender differences in head impacts sustained by collegiate ice hockey players. Med Sci Sports Exerc. 2012;44:297–304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Brust J, Leonard B, Pheley A, Roberts W. Children’s ice hockey injuries. Am J Dis Child. 1992;146:741–747. [DOI] [PubMed] [Google Scholar]
- 8. Brust J, Roberts W, Leonard B. Girls’ ice hockey injuries during tournament play: how do they compare in number, type, and seriousness with boys’ injuries? Med J Allina. 1998;7:27229. [Google Scholar]
- 9. Daneshvar DH, Nowinski CJ, McKee AC, Cantu RC. The epidemiology of sport-related concussion. Clin Sports Med. 2011;30:1–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Decloe MD, Meeuwisse WH, Hagel BE, Emery CA. Injury rates, types, mechanisms and risk factors in female youth ice hockey. Br J Sports Med. 2013;27:27. [DOI] [PubMed] [Google Scholar]
- 11. Emery C, Hagel B, Decloe M, Carly M. Risk factors for injury and severe injury in youth ice hockey: a systematic review of the literature. Inj Prev. 2010;16:113–118. [DOI] [PubMed] [Google Scholar]
- 12. Emery C, Meeuwisse W. Injury rates, risk factors, and mechanisms of injury in minor hockey. Am J Sports Med. 2006;34:1960–1969. [DOI] [PubMed] [Google Scholar]
- 13. Falconer T. Women’s hockey: speed, smarts, and skill. Equinox. 1994;January/February. [Google Scholar]
- 14. Flik K, Lyman S, Marx R. American collegiate men’s ice hockey: an analysis of injuries. Am J Sports Med. 2005;33:183–187. [DOI] [PubMed] [Google Scholar]
- 15. Gerberich S, Finke R, Madden M, Priest J, Aamoth G, Murray K. An epidemiological study of high school ice hockey injuries. Childs Nerv Syst. 1987;3:59–64. [DOI] [PubMed] [Google Scholar]
- 16. Gilenstam K, Karp S, Henriksson-Larsen K. Gender in ice hockey: women in a male territory. Scand J Med Sci Sports. 2008;18:235–249. [DOI] [PubMed] [Google Scholar]
- 17. Hastings D, Cameron J, Parker S, Evans J. A study of hockey injuries in Ontario. Ontario Med Rev. 1974;41:686–692. [Google Scholar]
- 18. Hayes D. Hockey injuries: how, why, where, and when? Phys Sportsmed. 1975;3:61–65. [DOI] [PubMed] [Google Scholar]
- 19. Herman K, Barton C, Malliaras P, Morrissey D. The effectiveness of neuromuscular warm-up strategies, that require no additional equipment, for preventing lower limb injuries during sports participation: a systematic review. BMC Med. 2012;10:75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Josse J, Baker J, Macpherson A. Hockey injuries across the lifespan: a descriptive, population-based study. Clin Kinesiol. 2009;63:39–45. [Google Scholar]
- 21. Macpherson A, Rothman L, Howard A. Body-checking rules and childhood injuries in ice hockey. Pediatrics. 2006;117:e143–e147. [DOI] [PubMed] [Google Scholar]
- 22. McKnight CM, Ferrara MS, Czerwinska JM. Intercollegiate ice hockey injuries: a three-year analysis. J Athl Train. 1992;27:338–343. [PMC free article] [PubMed] [Google Scholar]
- 23. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Park R, Castaldi C. Injuries in junior ice hockey. Phys Sportsmed. 1980;8:81–90. [DOI] [PubMed] [Google Scholar]
- 25. Pelletier R, Montelpare W, Stark R. Intercollegiate ice hockey injuries. A case for uniform definitions and reports. Am J Sports Med. 1993;21:78–81. [DOI] [PubMed] [Google Scholar]
- 26. Pinto M, Kuhn JE, Greenfield ML, Hawkins RJ. Prospective analysis of ice hockey injuries at the Junior A level over the course of one season. Clin J Sport Med. 1999;9:70–74. [DOI] [PubMed] [Google Scholar]
- 27. Rielly M. The nature and causes of hockey injuries: a five-year study. J Athl Train. 1982;17:88–90. [Google Scholar]
- 28. Rishiraj N, Lloyd-Smith R, Lorenz T, Niven B, Michel M. University men’s ice hockey: rates and risk of injuries over 6-years. J Sports Med Phys Fitness. 2009;49:159–166. [PubMed] [Google Scholar]
- 29. Roberts WO, Brust JD, Leonard B. Youth ice hockey tournament injuries: rates and patterns compared to season play. Med Sci Sports Exerc. 1999;31:46–51. [DOI] [PubMed] [Google Scholar]
- 30. Schick D, Meeuwisse W. Injury rates and profiles in female ice hockey players. Am J Sports Med. 2003;31:47–52. [DOI] [PubMed] [Google Scholar]
- 31. Stuart M, Smith A. Injuries in Junior A ice hockey. A three-year prospective study. Am J Sports Med. 1995;23:458–461. [DOI] [PubMed] [Google Scholar]
- 32. Stuart M, Smith A, Malo-Ortiguera S, Fischer T, Larson D. A comparison of facial protection and the incidence of head, neck, and facial injuries in Junior A hockey players. Am J Sports Med. 2002;30:39–42. [DOI] [PubMed] [Google Scholar]
- 33. Stuart M, Smith A, Nieva J, Rock M. Injuries in youth ice hockey: a pilot surveillance strategy. Mayo Clin Proc. 1995;70:350–356. [DOI] [PubMed] [Google Scholar]
- 34. Sutherland G. Fire on ice. Am J Sports Med. 1976;4:264–268. [DOI] [PubMed] [Google Scholar]
- 35. Tator C, Provvidenza C, Cassidy J. Spinal injuries in Canadian ice hockey: an update to 2005. Clin J Sport Med. 2009;19:451–456. [DOI] [PubMed] [Google Scholar]