

Abstract
Background:
Recent anatomical studies have identified the anterolateral ligament (ALL). Injury to this structure may lead to the presence of residual pivot shift in some reconstructions of the anterior cruciate ligament. The behavior of the length of this structure and its tension during range of motion has not been established and is essential when planning reconstruction.
Purpose:
To establish differences in the ALL length during range of knee motion.
Study Design:
Descriptive laboratory study.
Methods:
Ten unpaired cadavers were dissected. The attachments of the ALL were isolated. Its origin and insertion were marked with a 2 mm–diameter metallic sphere. Computed tomography scans were performed on the dissected parts under extension and 30°, 60°, and 90° of flexion; measurements of the distance between the 2 markers were taken at all mentioned degrees of flexion. The distances between the points were compared.
Results:
The mean ALL length increased with knee flexion. Its mean length at full extension and at 30°, 60°, and 90° of flexion was 37.9 ± 5.3, 39.3 ± 5.4, 40.9 ± 5.4, and 44.1 ± 6.4 mm, respectively. The mean increase in length from 0° to 30° was 3.99% ± 4.7%, from 30° to 60° was 4.20% ± 3.2%, and from 60° to 90° was 7.45% ± 4.8%. From full extension to 90° of flexion, the ligament length increased on average 16.7% ± 12.1%. From 60° to 90° of flexion, there was a significantly higher increase in the mean distance between the points compared with the flexion from 0° to 30° and from 30° to 60°.
Conclusion:
The ALL shows no isometric behavior during the range of motion of the knee. The ALL increases in length from full extension to 90° of flexion by 16.7%, on average. The increase in length was greater from 60° to 90° than from 0° to 30° and from 30° to 60°. The increase in length at higher degrees of flexion suggests greater tension with increasing flexion.
Clinical Relevance:
Knowledge of ALL behavior during the range of motion of the knee will allow for fixation (during its reconstruction) to be performed with a higher or lower tension, depending on the chosen degree of flexion.
Keywords: anterolateral ligament, tomography, rotatory instability, anatomy
Despite having been cited by Segond17 in 1879 as a pearly, resistant, and fibrous band in the anterolateral region of the knee, only recently were specific anatomical studies conducted to characterize the anterolateral ligament (ALL).
To date, we have knowledge of 5 anatomical structure studies on the ALL.3,5,6,8,21 According to these authors, with some variations, the ALL originates in the lateral epicondyle and follows an anteroinferior course toward the tibia, with tibial insertion between the Gerdy tubercle and the fibular head, slightly more than 5 mm below the articular cartilage of the lateral tibial plateau (Figure 1).
Figure 1.
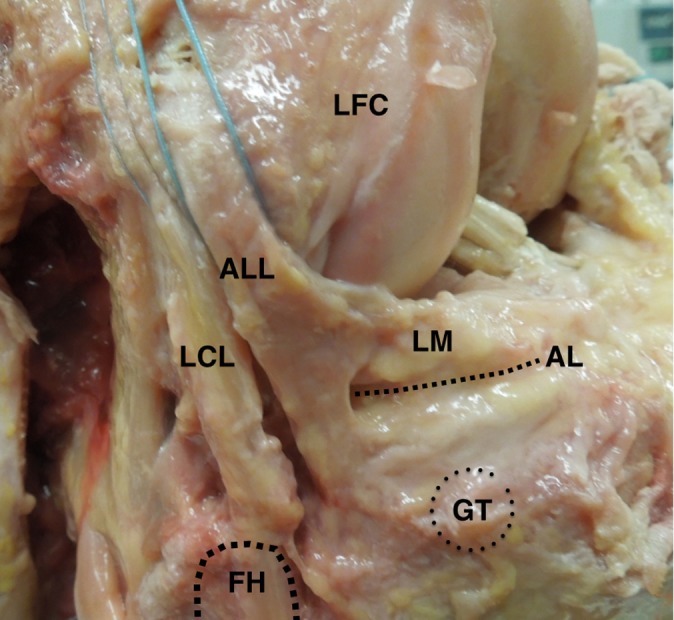
Anatomy of the anterolateral ligament (ALL). It originates in the lateral epicondyle, anterior and distal to the lateral collateral ligament (LCL) origin and follows an anteroinferior course toward the tibia, with tibial insertion between the Gerdy tubercle (GT) and the fibular head (FH), slightly more than 5 mm below the articular cartilage of the lateral tibial plateau. AL, articular line; LFC, lateral femoral condyle; LM, lateral meniscus.
Some authors such as Claes et al,3 Helito et al,6 and Vincent et al21 also found an insertion on the lateral meniscus, between the anterior horn and the body of this structure. Helito et al6 confirmed the meniscal insertion by histological analysis of the dissected specimens.
The ALL function is related to the genesis of the knee’s anterolateral instability, and its injury would generate an increased grade in the pivot-shift test when associated with injury to the anterior cruciate ligament (ACL).15
Monaco et al15 conducted a biomechanical study causing injury to the anterolateral knee capsule and showed a significant increase in the pivot shift in these cases. We believe that the ALL function was indirectly being tested in this study.
Among the anatomical studies that have been conducted, there is wide divergence regarding the changes in length of the ALL with variations in the flexion-extension of the knee. Vieira et al,20 in a study on the iliotibial tract, suggested that the structure denominated ALL decreases in length with increased knee flexion, in concordance with Dodds et al.5 Vincent et al21 and Claes et al3 in turn suggested a greater tensioning of the structure under flexion.
Dodds et al5 and Claes et al3 measured the ALL under flexion and extension and obtained different results. Whereas Claes et al3 observed an increase of approximately 3 mm, Dodds et al5 found a decrease of 4 mm in the length of the ligament with flexion. These differences may be due to variations between the ALL anatomy among these studies.
We believe that these changes are controversial and that an effort to establish the actual behavior of this structure is necessary for the development of biomechanical tests aiming to elucidate the role of this ligament in the genesis of anterolateral knee instability. Furthermore, knowledge of the isometry of the ligaments is important for successful repair or reconstruction of ligament injuries.
Thus, the present study aimed to establish the differences in length of the ALL of the knee under different degrees of knee flexion with the use of computed tomography (CT). We hypothesize that the ligament length increases with increased knee flexion, thus suggesting a greater tension at this position.
Materials and Methods
For the present study, 10 unpaired cadaver knees were used. Eight knees were from males, and 2 were from females. The study was conducted following approval from the science and research ethics committee at our institution.
The knees were dissected to isolate the origin and insertion of the ALL, without violating the adjacent structures. After skin and subcutaneous tissue dissection, the only structure that was removed for access to the ALL was the iliotibial tract, as a standard procedure for ALL dissection, similar to previous studies analyzing this structure.3,5,6,8 After dissection of the ligament, metal markers were placed in the femoral origin and tibial insertion. Local soft tissues were cleared for viewing the correct points. The marker was placed adjacent to the femoral and tibial cortical bone, the same way performed by Helito et al7 in an radiographic study on the ALL. After placement of the markers, the iliotibial tract, subcutaneous tissue, and skin were closed.
Computed tomography scans were performed on the dissected specimens in full extension and at 30°, 60°, and 90° of flexion. The degree of flexion of the specimens was controlled with a goniometer. The rotation was controlled during flexion so that all images in different degrees of flexion were performed with the knee in neutral rotation.
The CT scans were analyzed using the OsiriX DICOM viewer software (v3.6; 32-bit). This software was used recently for several studies in the knee and has good accuracy and reliability with length measurements.10,12,13,18 Measurements were taken of the distance between the metal markers on all specimens and under all the aforementioned degrees of flexion. The measurement consisted of the linear distance between the 2 markers, using multiplanar reconstruction (MPR) oriented at an oblique coronal plane in which both markers were identified, representing the long axis of the ligament (Figure 2). The center of the marker and the level of the cortical bone in which it was inserted were standardized as references for the measurements. The measurements were performed by 2 investigators. Interobserver correlations of the measurements were performed.
Figure 2.

Computed tomography scan of one of the cadaver knees with 30º of flexion exemplifying the ligament measurement technique. Multiplanar reconstruction (A) axially, (B) sagittally, and (C) coronal-obliquely oriented on the long axis of the ligament. The anterolateral ligament length was measured in the coronal oblique plane by calculating the distance between the centers of the metallic markers fixed in its origin and insertion.
The distances between the fixed points were described with the use of summary measures (mean, standard deviation, median, minimum, and maximum) and were compared among the degrees of knee flexion with the use of repeated-measures analysis of variance (ANOVA) followed by multiple Bonferroni comparisons16 to check for differences in the distances between each degree of knee flexion. Comparison of differences16 between the variations of the distances among the degrees of knee flexion was performed.
The results are illustrated in Table 1, with the mean profile of the distances in the varying degrees of knee flexion with the respective standard errors. All tests were performed with a significance level of 5% (P < .05).
TABLE 1.
Length of Anterolateral Ligament at Full Extension (0°) and at 30°, 60°, and 90° of Knee Flexion
| Knee flexion, deg | Length, cm | ||
|---|---|---|---|
| Mean ± SD | Median | Range | |
| 0 | 3.79 ± 0.53 | 3.71 | 2.99-4.72 |
| 30 | 3.93 ± 0.54 | 3.97 | 3.09-4.77 |
| 60 | 4.09 ± 0.54 | 4.21 | 3.11-4.82 |
| 90 | 4.41 ± 0.64 | 4.54 | 3.12-5.23 |
Results
The ALL was found in all dissected anatomical specimens. The mean length of the 10 specimens under study increased with increased degree of knee flexion. The mean length at full extension and at 30°, 60°, and 90° of flexion was 37.9, 39.3, 40.9, and 44.1 mm, respectively (Table 1 and Figure 3). The mean length increase from 0° to 30° was 3.99%, from 30° to 60° was 4.20%, and from 60° to 90° was 7.45%. From full extension to 90° of flexion, the length of the ligament increased by 16.7% on average (Figure 4). Only 2 cadavers showed a decrease in ligament length from 0° to 30°; all other measurements showed an increase in length with increased flexion. Nevertheless, this decrease was less than 1.0 mm.
Figure 3.
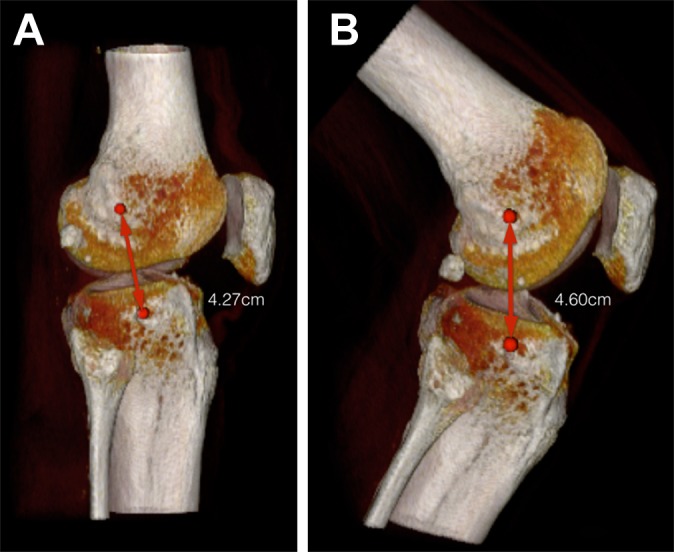
Three-dimensional computed tomography scans of one of the knees used in the study under (A) full extension and (B) 90° of flexion. Metal markers show an increase in length between the points of origin and insertion of the anterolateral ligament.
Figure 4.
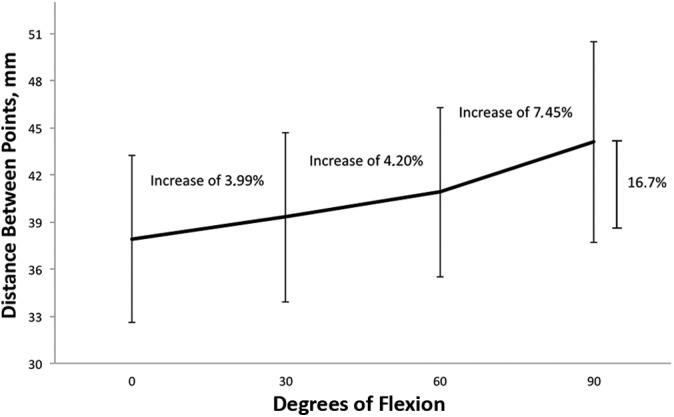
Plot showing the percentage increase in anterolateral ligament length according to the degree of knee flexion. Bars indicate the standard deviation in each degree of knee flexion.
The interobserver correlation indices for the studied variables were 0.91 to 0.99.
Change in the ligament length under varying degrees of knee flexion was statistically significant, according to ANOVA (P < .001). For every increase of 30° of flexion of the knee, there was a statistically significant mean increase in the distance between the points (P < .05). The mean increase in the distance between the points from 0° to 30° was statistically equal to the mean increase from 30° to 60° of knee flexion (P = .843); however, from 60° to 90° of flexion, there was a statistically higher mean increase in the distance between points than from 0° to 30° and from 30° to 60° (P = .033 and P = .050, respectively) (Table 2).
TABLE 2.
Comparison of Anterolateral Ligament Length Differences Under Varying Degrees of Knee Flexion
| Analysis, deg of knee flexion | Mean Difference in Distance Between Points, cm | P |
|---|---|---|
| 0 × 30 | 0.15 | .05 |
| 0 × 60 | 0.31 | .001 |
| 0 × 90 | 0.62 | <.001 |
| 30 × 60 | 0.16 | .025 |
| 30 × 90 | 0.47 | <.001 |
| 60 × 90 | 0.31 | <.001 |
| 0-30 × 30-60 | 0.01 | .843 |
| 0-30 × 60-90 | 0.17 | .033 |
| 30-60 × 60-90 | 0.15 | .05 |
Discussion
According to the results of the present study, this structure exhibited an increase in length, with knee flexion increasing by 6.3 mm (or 17.6%) of its length on average. These findings corroborate the subjective findings of Vincent et al,21 who reported that knee flexion at 90° causes the ALL to be tenser, and the objective findings of Claes et al,3 who demonstrated that the ligament increases, on average, by 3 mm from extension to flexion. Dodds et al5 reported a decrease in the ALL length with flexion. We believe that this decrease is because the femoral origin point found by this author greatly differs from the findings of other studies. Dodds et al5 found the source of the ALL to be posterior and proximal to the origin of the lateral collateral ligament (LCL), whereas other authors have found it to be anterior and distal to the LCL. In this study, the anatomical findings were similar to the findings of the anatomical dissections performed Claes et al3 and Helito et al.6,8 Helito et al6 also performed histological analysis of the femoral attachment of the ALL, which suggests that the findings in this study should correspond to the correct origin of the ALL.
According to the biomechanical study conducted by Monaco et al,15 transection of the anterolateral capsule after transection of the ACL significantly increases the grade in the pivot-shift test. These authors also showed increased internal rotation at all degrees of flexion (from 0° to 90°), with knee capsule transection after transection of the ACL; however, only at 30° of flexion was this increase statistically significant, which might suggest higher tensioning of the ligament at this degree of flexion.
An important restrictor of the external rotation of the tibia is the complex formed by the tendon of the popliteus muscle and the popliteal fibular ligament.11 According to the biomechanical tests conducted by Zhang et al,23 the increase in the external rotation of the tibia relative to the femur when these structures are sectioned is increased with increasing knee flexion. Taking into account an antagonistic function of the ALL and the tendon of the popliteus muscle, as suggested by Helito et al6 in an anatomical study of the ALL, and considering a major function of the popliteal–popliteal fibular complex at higher degrees of flexion, it is possible that the ALL also exhibits greater tension with higher degrees of flexion. LaPrade et al11 also noted a greater external rotation with transection of the popliteus muscle at 90° of flexion, compared with 30° and 60°.
The characterization of the degree of flexion at which the ligament exhibits higher tension is important at the time of reconstruction of this structure. All ligamentous structures of the knee have been analyzed through similar studies, which is essential at the time of graft fixation in a reconstruction.2,4,19,22 Structures fixed with high tension can cause restriction of movement, while fixation without proper tension can lead to laxity and failure of the reconstruction.1
According to the data analysis, especially the increase in the length of the structure from 60° to 90°, compared with the increase from 0° to 30° and from 30° to 60°, the ALL appears to have higher tension and therefore is under greater mechanical stress with higher degrees of flexion. We believe that the ALL exhibits a more erratic behavior from 0° to 30°, possibly due to lack of significant tension because, despite having a mean increase similar to the variation from 30° to 60°, 2 cadavers showed a decrease, albeit small, in the ALL length compared with full extension.
The behavior exhibited by the ALL in the present study is different from the behavior exhibited by other peripheral structures of the knee, both at the lateral and the medial sides. Victor et al19 showed that the superficial medial collateral ligament (MCL) and the deep MCL tend to remain isometric during range of motion, whereas the LCL and the medial patellofemoral ligament tend to exhibit a smaller distance between bone landmarks with increasing knee flexion. The ALL exhibited characteristics similar to those of the posterior cruciate ligament (PCL), with a gradual increase in length from 0° to 90°, as shown by Cross et al,4 and different from those of the ACL, which also displays a decrease in length from 0° to 90° of flexion, as shown by Yoo et al22 and Iwahashi et al9 in biomechanical studies. Li et al14 studied both the ACL and the PCL and corroborated the aforementioned findings, showing a decrease in the ACL length during flexion, particularly of the posterolateral band, and stretching of the 2 PCL bands, with the largest increase being observed for the anterolateral band. Li et al14 used the same degrees of flexion as in the present study.
Considering the ALL as a ligament with a function analogous to that of the ACL, we hypothesized that its stretching behavior under flexion seems logical and differs from the behavior of the ACL, which stretches under extension. Thus, the ALL would be an important secondary restrictor assist to the ACL in the angles of flexion in which the ACL is looser. Table 3 lists the measurements of the ACL and PCL reported in the study by Li et al14 and the measurements of the ALL found in the present study.
TABLE 3.
Anterolateral Ligament Length Compared With ACL and PCL Lengthsa
| Length, cm | |||||
|---|---|---|---|---|---|
| ALLb | ACLc | PCLc | |||
| AM Bundle | PL Bundle | AL Bundle | PM Bundle | ||
| Knee flexion, deg | |||||
| 0 (full extension) | 3.78 | 3.25 | 2.76 | 2.78 | 2.88 |
| 30 | 3.93 | 3.25 | 2.63 | 3.37 | 3.22 |
| 60 | 4.09 | 3.07 | 2.41 | 3.54 | 3.37 |
| 90 | 4.40 | 3.02 | 2.35 | 3.64 | 3.51 |
| Increase from 0° to 90°, cm (%) | 0.62 (16) | –0.23 (–7) | –0.41 (–15) | 0.86 (31) | 0.63 (22) |
aIn the table, it is possible to observe the behavior of the anterolateral ligament (ALL), which is similar to that of the posterior cruciate ligament (PCL) and different from that of the anterior cruciate ligament (ACL) during knee flexion. AL, anterolateral; AM, anteromedial; PL, posterolateral; PM, posteromedial.
bFrom the present study.
cFrom Li et al.14
The ALL behavior observed in the present study suggests that, during potential reconstruction, the ALL tensioning and fixation should be set between 60° and 90° of flexion, similar to the PCL.
Our study is important because it objectively and accurately characterized the differences in length of the ALL under different degrees of flexion, suggesting a higher tensioning of the ligament with increasing flexion. We believe that the tomographic measurement is more accurate than the anatomical measurement and less subject to interpretation bias, and therefore this method was chosen. Other options to evaluate the isometry would involve computer graphics models, as used by Victor et al19; however, simple tomography with reconstruction appears adequate, in our opinion, for length measurements. To our knowledge, no other studies have characterized the ALL length under varying degrees of flexion, which increases the relevance of the present investigation.
Possible criticisms to the present study are the incision of the iliotibial tract in the anterolateral region of the knee to access the ALL, measurements of the knee in neutral rotation, and the small number of cadavers. Without resection of the iliotibial tract, access to the region for clear delineation of the ligament is not possible; however, its opening can, even in a small way, have affected the distance between the points when performing knee flexion. Due to the experience in dissections on the lateral region of the knee and especially of the ALL, we hypothesized no other local structures were injured or had their biomechanical function impaired. An additional limitation of our method is that we measured the linear distance between the attachment points of the ligament, which may represent a simplification of the 3-dimensional anatomic situation. Different degrees of rotation of the knee may interfere with the length and tension of the ALL; however, we consider it essential to understand the length pattern of the ligament in neutral rotation at different degrees of flexion so that we can progress to studies on the effects of internal and external rotation. Regarding the relatively small number of cadavers used in the present study, similar studies have been performed with a smaller number of knees.4,23
Conclusion
The ALL has no isometric behavior during the range of motion of the knee. The ALL increases in length by 16.7%, on average, from full extension to 90° of flexion. The increase in length is greater from 60° to 90° than from 0° to 30° and from 30° to 60°. The increase in length at higher degrees of flexion suggests greater tension with increasing flexion.
Footnotes
The authors declared that they have no conflicts of interest in the development and publication of this contribution.
References
- 1. Austin JC, Phornphutkul C, Wojtys EM. Loss of knee extension after anterior cruciate ligament reconstruction: effects of knee position and graft tensioning. J Bone Joint Surg Am. 2007;89:1565–1574. [DOI] [PubMed] [Google Scholar]
- 2. Boisgard S, Levai JP, Geiger B, Saidane K, Landjerit B. Study of the variations in length of the anterior cruciate ligament during flexion of the knee: use of a 3D model reconstructed from MRI sections. Surg Radiol Anat. 1999;21:313–317. [DOI] [PubMed] [Google Scholar]
- 3. Claes S, Vereecke E, Maes M, Victor J, Verdonk P, Bellemans J. Anatomy of the anterolateral ligament of the knee. J Anat. 2013;223:321–328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Cross MB, Raphael BS, Maak TG, Plaskos C, Egidy CC, Pearle AD. Characterization of the orientation and isometry of Humphrey’s ligament. Knee. 2013;20:515–519. [DOI] [PubMed] [Google Scholar]
- 5. Dodds AL, Halewood C, Gupte CM, Williams A, Amis AA. The anterolateral ligament: anatomy, length changes and association with the Segond fracture. Bone Joint J. 2014;96-B:325–331. [DOI] [PubMed] [Google Scholar]
- 6. Helito CP, Demange MK, Bonadio MB, et al. Anatomy and histology of the knee anterolateral ligament. Orthop J Sports Med. 2013;1(7). doi: 10.1177/2325967113513546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Helito CP, Demange MK, Bonadio MB, et al. Radiographic landmarks for locating the femoral origin and the tibial insertion of the knee anterolateral ligament. Am J Sports Med. 2014;42:2356–2362. [DOI] [PubMed] [Google Scholar]
- 8. Helito CP, Miyahara HS, Bonadio MB, et al. Anatomical study of the anterolateral knee ligament [in Portuguese]. Rev Bras Ortop. 2013;48:368–373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Iwahashi T, Shino K, Nakata K, et al. Assessment of the “functional length” of the three bundles of the anterior cruciate ligament. Knee Surg Sports Traumatol Arthrosc. 2008;16:167–174. [DOI] [PubMed] [Google Scholar]
- 10. Kim G, Jung HJ, Lee HJ, Lee JS, Koo S, Chang SH. Accuracy and reliability of length measurements on three-dimensional computed tomography using open-source OsiriX software. J Digit Imaging. 2012;25:486–491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. LaPrade RF, Wozniczka JK, Stellmaker MP, Wijdicks CA. Analysis of the static function of the popliteus tendon and evaluation of an anatomic reconstruction: the “fifth ligament” of the knee. Am J Sports Med. 2010;38:543–549. [DOI] [PubMed] [Google Scholar]
- 12. Lee YS, Lee BK, Oh WS, Cho YK. Comparison of femoral tunnel widening between outside-in and trans-tibial double-bundle ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2014;22:2033–2039. [DOI] [PubMed] [Google Scholar]
- 13. Lee YS, Oh WS, Chun DI. Change of the tunnel configuration in the non-anatomic trans-tibial double bundle ACL reconstruction. Knee. 2014;21:757–762. [DOI] [PubMed] [Google Scholar]
- 14. Li G, DeFrate LE, Sun H, Gill TJ. In vivo elongation of the anterior cruciate ligament and posterior cruciate ligament during knee flexion. Am J Sports Med. 2004;32:1415–1420. [DOI] [PubMed] [Google Scholar]
- 15. Monaco E, Ferretti A, Labianca L, et al. Navigated knee kinematics after cutting of the ACL and its secondary restraint. Knee Surg Sports Traumatol Arthrosc. 2012;20:870–877. [DOI] [PubMed] [Google Scholar]
- 16. Neter J, Kutner MH, Nachtsheim CJ, Wasserman W. Applied Linear Statistical Models. 4th ed Chicago, IL: Irwin; 1996. [Google Scholar]
- 17. Segond P. Recherches Cliniques et Expérimentales sur les Épanchements Sanguins du Genou par Entorse. Paris, France: Bureaux du Progrès Médical; 1879. [Google Scholar]
- 18. Shea KG, Polousky JD, Jacobs JC, Jr, Ganley TJ. Anatomical dissection and CT imaging of the posterior cruciate and lateral collateral ligaments in skeletally immature cadaver knees. J Bone Joint Surg Am. 2014;96:753–759. [DOI] [PubMed] [Google Scholar]
- 19. Victor J, Wong P, Witvrouw E, Sloten JV, Bellemans J. How isometric are the medial patellofemoral, superficial medial collateral, and lateral collateral ligaments of the knee? Am J Sports Med. 2009;37:2028–2036. [DOI] [PubMed] [Google Scholar]
- 20. Vieira EL, Vieira EA, da Silva RT, Berlfein PA, Abdalla RJ, Cohen M. An anatomic study of the iliotibial tract. Arthroscopy. 2007;23:269–274. [DOI] [PubMed] [Google Scholar]
- 21. Vincent JP, Magnussen RA, Gezmez F, et al. The anterolateral ligament of the human knee: an anatomic and histologic study. Knee Surg Sports Traumatol Arthrosc. 2012;20:147–152. [DOI] [PubMed] [Google Scholar]
- 22. Yoo YS, Jeong WS, Shetty NS, Ingham SJ, Smolinski P, Fu F. Changes in ACL length at different knee flexion angles: an in vivo biomechanical study. Knee Surg Sports Traumatol Arthrosc. 2010;18:292–297. [DOI] [PubMed] [Google Scholar]
- 23. Zhang H, Zhang J, Liu X, et al. In vitro comparison of popliteus tendon and popliteofibular ligament reconstruction in an external rotation injury model of the knee: a cadaveric study evaluated by a navigation system. Am J Sports Med. 2013;41:2136–2142. [DOI] [PubMed] [Google Scholar]