

Abstract
Background:
Repetitive tensile stresses from valgus torque can induce elbow injury in adolescent baseball players. Insufficient hip range of motion (ROM) can change throwing mechanics, reducing the transfer of energy from the lower to the upper extremities. Thus, hip ROM limitations may force the upper extremities to bear the burden of a strong throw. Improper pitching mechanics caused by insufficient hip ROM are thought to increase valgus torque on the elbow when throwing, increasing the risk of elbow injury.
Purpose:
To investigate the relationship between elbow pain and hip ROM in adolescent baseball players.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 122 adolescent baseball players with a mean age of 12.0 years (range, 6-14 years) participated in this study. Elbow pain, hip flexion angle, and the internal rotation angles of the hip at 0° and 90° of flexion were assessed. Participants were divided into a pain group and a normal group based on the pain assessment, and each hip angle was compared between groups using Student t tests. P values <.05 were considered statistically significant.
Results:
Thirty-one of 122 players had elbow pain. The hip flexion angle of the trail leg was 121.9° ± 12.3° for the normal group and 111.2° ± 11.3° for the pain group (P = .0001). The plant leg hip flexion angles were 122.0° ± 12.4° and 113.6° ± 11.3° (P = .0014) for the normal and pain groups, respectively. The internal rotation angle at 0° of hip flexion of the trail leg was 49.4° ± 12.6° and 45.6° ± 8.8° (not significant), and of the plant leg was 49.1° ± 12.5° and 48.7° ± 11.5° (not significant), for the normal and pain groups, respectively. The internal rotation of the trail leg at 90° of hip flexion was 46.9° ± 13.3° in the normal group and 36.1° ± 15.7° in the pain group (P = .0005). In the plant leg, the internal rotation angle at 90° of hip flexion was 46.9° ± 12.2° and 36.4° ± 18.1° for the normal and pain groups, respectively (P = .0013).
Conclusion:
Limitations to hip flexion and internal rotation at 90° of hip flexion were risk factors for elbow injury. Differences in internal rotation angles between 0° and 90° of hip flexion may be important criteria for identifying adolescent baseball players at risk of elbow pain.
Keywords: throwing elbow, pitching mechanics, hip range of motion, prevention
During throwing, the combination of valgus torque and rapid extension generates tensile stress on the elbow. This repetitive tensile force challenges the ultimate strength of the ulnar collateral ligament and the medial apophysis and results in compressive loading of the lateral compartment of the elbow joint; these are well-known risk factors for throwing elbow injury.8,9,15,17,18 The force generated by the lower extremities of the body during throwing is transferred via the kinetic chain through the core, shoulder, elbow, and ultimately, the hand before ball release.5,10,22,23,26,27 Proper positioning of the plant leg, which is the leg contralateral to the throwing arm, allows for optimal rotation of the hips, pelvis, and trunk. This is crucial for providing the most effective transfer of energy through the kinetic chain.5,10 Proper alignment of the pelvis with the intended target at lead foot contact, maximal shoulder external rotation, and correct ball release have been shown to decrease the magnitude of the forces and torque on the arm.22,26 An insufficient hip rotation range of motion (ROM) can arrest the throwing mechanics, thereby reducing the transfer of energy from the lower to the upper extremities.5,14,24,27 Thus, proper positioning of the pelvis is an important factor not only for performance but also for preventing upper extremity injuries.
There are currently no reports that compare hip ROM between healthy adolescent players and adolescent players with a painful throwing elbow. This study examined the relationships between hip ROM and throwing elbow pain.
Materials and Methods
Participants
A total of 122 baseball players (mean age, 12.0 ± 1.9 years) who attended our preseason medical check volunteered to participate in this cross-sectional study. All participants and their parents provided informed consent. No participant had any history of hip disorders, such as Perthes disease, slipped capital femoral epiphysis, or any congenital disorders. To assess the relationships between hip ROM and throwing elbow pain, participants were divided into 2 groups: Those who reported elbow tenderness (medial, lateral, and posterior) at the medical check or who had felt pain while throwing during the past month were allocated to the pain group, and the rest were allocated to the normal group. The straight-leg raising angle (SLR) and hip ROM were measured in all participants using a standard technique19 and the same double-long-arm goniometer (Figure 1). Elbow pain was assessed separately from the SLR and hip measurements so that the examiners were unaware of each subject’s group designation.
Figure 1.

Measurement techniques for (A) straight-leg raising angle (SLR), (B) hip flexion, (C) internal rotation at 90° of hip flexion (IR90), and (D) internal rotation at 0° of hip flexion (IR0).
Supine Position Measurements
Straight-Leg Raising Angle
With the contralateral hip and knee fully extended along the midline, the study limb was raised until the pelvis began to move. To control for pelvis tilt, 1 examiner held the anterior-superior iliac spine in a fixed position while the other measured the SLR angle, which was the angle between the horizontal and the axis of the raised leg.
Flexion
With the contralateral hip and knee fully extended along the midline, the study limb was flexed until the hip was felt to impinge on the pelvis and the pelvis began to move. To control for pelvis tilt, 1 examiner held the anterior-superior iliac spine in a fixed position while the other measured the hip flexion angle, which was the angle between the horizontal and the axis of the flexed thigh.
Internal Rotation at 90° of Hip Flexion
With the contralateral hip and knee fully extended, the hip and knee of the study limb were flexed to 90° (confirmed by goniometer). While 1 examiner stabilized the pelvis and contralateral thigh, the other rotated the hip internally to its maximal point. The internal rotation (IR90) was then measured as the angle between the trunk and the axis of the flexed leg.
Prone Position Measurements
Internal Rotation of the Extended Hip
With the contralateral hip and knee in a neutral position along the midline, the study limb was held at 0° of hip flexion/extension and the knee was flexed to 90° (confirmed by goniometer). The hip was then internally rotated until the pelvis started to move. The internal rotation (IR0) was measured as the angle between vertical and the axis of the leg.
In each participant, both hips were measured, and the 2 values were averaged to produce a single data point for each ROM index (eg, flexion, IR0, and IR90). Previous reports suggest that a difference of more than 6° is required to accurately detect a real change in ROM by goniometry.1,2,19 Power analysis indicated that 23 subjects would be necessary to assess the intra- and interobserver reliability of our measurements with an α of .05 and power of 0.8 using a minimal detectable difference of 6° in goniometric measurements and a standard deviation of 11°.2,19
Statistical Analysis
Statistical analyses were performed using JMP software version 8.0 (SAS Institute, Cary, North Carolina, USA). Results are presented as means ± standard deviations for each group. A Student t test was used to assess differences between the normal group and the pain group. Differences between hip ROM in the plant leg and the trail leg were assessed using a paired t test. P values of <.05 were considered statistically significant. Pearson correlation coefficients were used to assess the associations between hip ROM, IR0, and IR90. Intraclass correlation coefficients (ICCs) were calculated to measure intra- and inter-rater reliability to detect the conformity of the measurements between examiners and within the same examiner at different times.20 Ninety-five percent confidence intervals (95% CIs) were constructed around the ICC. We used the Landis and Koch13 classification to determine strength of agreement: 0.61 to 0.80 was considered substantial agreement and 0.81 to 1 was considered almost perfect agreement. Statistical power was analyzed using PS version 3.0.34 (Vanderbilt University, Nashville, Tennessee, USA).
Ethical Considerations
We obtained informed consent from all participants, their parents, and coaches before beginning this investigation. Study protocols were approved by the ethics committee of our hospital.
Results
Thirty-three (27.0%) of 122 players had elbow pain. The mean ages of both groups were similar (normal group, 11.9 ± 2.0 years; pain group, 12.5 ± 1.4 years; P = .24). Twenty-seven players had pain on the medial side of the elbow, 4 had pain on the lateral side of the elbow, and 2 had pain on both the medial and lateral sides. Two of 6 players were diagnosed radiographically as having osteochondritis dissecans. All players could achieve 0° of hip extension during ROM measurements. Descriptive statistics for hip ROM are shown in Table 1. There were 2 participants in the pain group for whom IR0 measurements were not recorded; these participants were excluded from the statistical comparison of IR0 and IR90 in the pain group. There were no significant differences in SLR between the pain group and the normal group on either the trail leg or the plant leg side (P = .061, power = 0.50 and P = .18, power = 0.25, respectively). The hip flexion of the pain group was significantly lower than that of the normal group in both the trail leg (P = .0001, power = 0.96) and the plant leg (P = .0014, power = 0.92) (Figure 2). However, the IR0 angle did not differ between the 2 groups in either leg (trail leg, P = .16, power = 0.26; plant leg, P = .67, power = 0.052). The IR90 angle of the pain group was significantly lower than that of the normal group in both the trail leg and the plant leg (P = .0005, power = 0.96 and P = .0013, power = 0.95, respectively) (Figure 3). In the normal group, there were no significant differences between the IR90 and the IR0 angles in either leg (trail leg, P = .19, power = 0.26; plant leg, P = .23, power = 0.23). However, in the pain group, the IR90 angle was significantly lower than the IR0 angle in both the trail leg (P = .0057, power = 0.81) and the plant leg (P = .0075, power = 0.78) (Figure 4).
TABLE 1.
Results of Straight-Leg Raising Angle and Hip Range of Motion Measurementsa
| Normal Group (n = 89) | Pain Group (n = 33) | |||
|---|---|---|---|---|
| Trail Leg | Plant Leg | Trail Leg | Plant Leg | |
| SLR | 75.1 ± 14.1 | 74.8 ± 14.8 | 69.5 ± 11.5 | 71.1 ± 10.5 |
| Hip flexion | 121.9 ± 12.3 | 122.0 ± 12.4 | 111.2 ± 11.3 | 113.6 ± 11.3 |
| IR0b | 49.4 ± 12.6 | 49.1 ± 12.5 | 45.6 ± 8.8 | 48.7 ± 11.5 |
| IR90 | 46.9 ± 13.3 | 46.9 ± 12.2 | 36.1 ± 15.7 | 36.4 ± 18.1 |
aIR0, internal rotation at 0° of hip flexion; IR90, internal rotation at 90° of hip flexion; SLR, straight-leg raising angle.
bThere were 2 players in the pain group who did not have IR0 measurements recorded.
Figure 2.
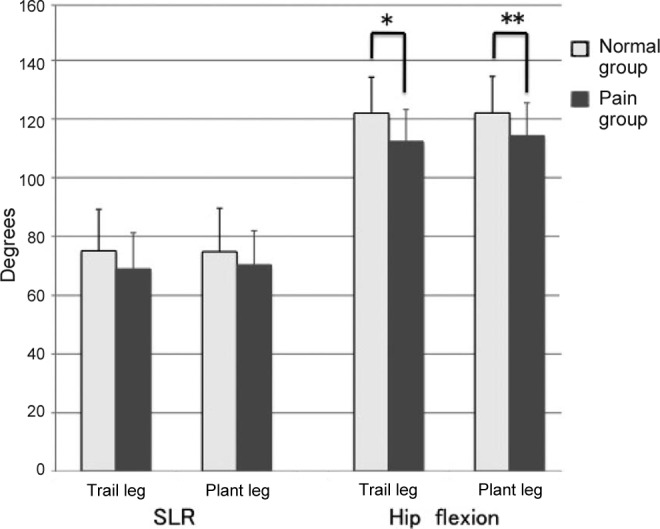
Comparison of the straight-leg raising angle (SLR) and hip flexion between the normal group and the pain group.
There were no differences in SLR between the normal group and the pain group on either side (trail leg, P = .061, power = 0.50; plant leg, P = .18, power = 0.25). Significant differences in hip flexion between the 2 groups were observed in both the trail and plant legs: *trail leg, P = .0001, power = 0.96; **plant leg, P = .0014, power = 0.92.
Figure 3.
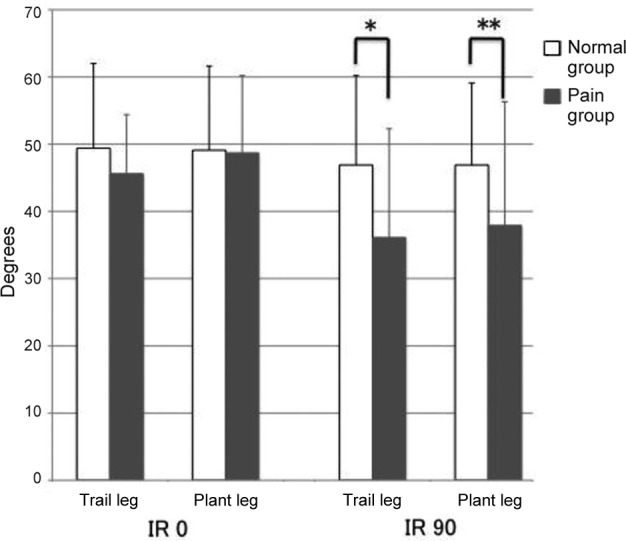
Comparison of internal rotation at 0° of hip flexion (IR0) and internal rotation at 90° of hip flexion (IR90) between the normal group and the pain group. There were no differences in IR0 between the normal group and the pain group on either side (trail leg: P = .16, power = 0.26; plant leg: P = .67, power = 0.052). Significant differences in IR90 between the 2 groups were observed bilaterally: *trail leg, P = .0005, power = 0.96; **plant leg: P = .0013, power = 0.95.
Figure 4.
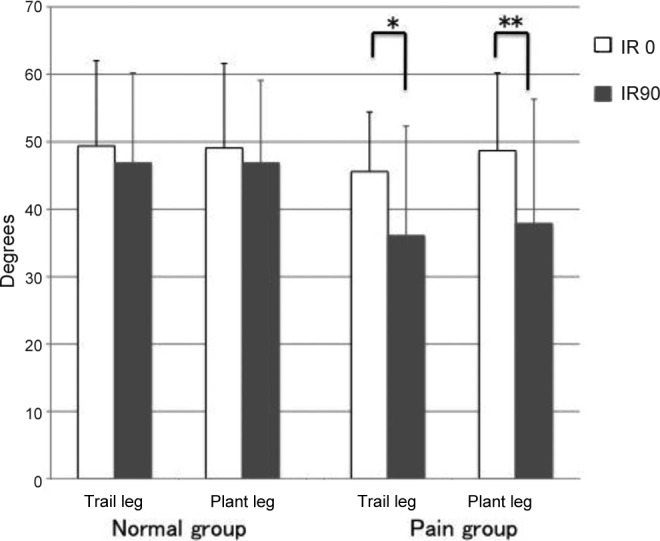
Comparison between internal rotation at 0° of hip flexion (IR0) and internal rotation at 90° of hip flexion (IR90) on the same side. There was no significant difference between IR90 and IR0 in the normal group (trail leg, P = .19, power = 0.26; plant leg, P = .23, power = 0.23). The IR90 angle was significantly lower than the IR0 angle on both sides in the pain group: *trail leg, P = .0057, power = 0.81; **plant leg, P = .0075, power = 0.78.
Interexaminer reliability indicated excellent agreement for all indices (ICC >0.81). Intraexaminer assessments also revealed excellent agreement for all indices (ICC >0.81).
Discussion
Throwing generates tensile stress on the elbow through a combination of valgus torque and rapid extension. The mechanics of pitching are quite complex and require the coordination of multiple motion segments. Improper coordination of the kinetic chain from the lower extremity to the trunk results in an improper upper arm position and increased forces on the elbow.4 Therefore, modification of throwing technique to properly coordinate the kinetic chain is important for minimizing painful injuries to the throwing elbow. One reason for poor coordination of the kinetic chain while throwing is thought to be hip ROM limitation.5,10,14,24,27 Achieving proper plant leg positioning when the foot is planted (a closed-shoulder position) allows for optimal rotation of the hips, pelvis, and trunk, which is crucial for providing increased speed in both hips after flexion through the kinetic chain.5,10 To achieve this position during the cocking phase of the throwing motion requires sufficient hip ROM to allow internal rotation of the trail leg.27 Davis et al4 reported that the elbow valgus load increased when the closed-shoulder position was incorrect. Compared with healthy players, the adolescent players with throwing pain in our study had significantly restricted hip flexion and IR90. These ROM restrictions inhibit proper trunk rotation; therefore, players with hip ROM limitations tend to have an open-shoulder position when the plant foot contacts the ground. Our results are similar to those of other studies,4,14,23 which also suggest that limitations in hip flexion and IR90 may be related to throwing elbow pain in adolescent baseball players.
We found no significant differences between the normal group and the pain group in IR0 values for either leg; however, IR90 values for both legs were significantly lower in the pain group than in the normal group. There were no significant differences between the IR0 and IR90 of either the plant or trail leg in both the pain group and the normal group. Ellenbecker et al6 reported that there was significant variability in the differences between dominant and nondominant lower extremities and that a consistent pattern of hip rotation was not evident in professional baseball pitchers. Previous studies have also reported no significant differences in the IR90 and IR0 of healthy children and adults.7,12,19 Compared with the normal group, hip flexion and IR90 in the pain group were restricted significantly in our results. Moreover, the difference between mean IR0 and mean IR90 in pain group was around 10° in both hips. Taken together, this information suggests that differences between IR90 and IR0, especially in players who show asymmetry between IR0 and IR90 more than 10°, may be a physical feature of adolescent players who are prone to throwing elbow pain.
Bone, ligament, and muscle are all thought to be factors in ROM limitations. The participants in this study did not have any history of congenital or traumatic hip disorders. The hip is a complex ball and socket joint that permits movement in multiple planes.16 Ellenbecker et al6 suggested that subjects with significant ROM limitations may have subclinical pathologic changes, such as early osteoarthritis or femoroacetabular impingement. Siebenrock et al21 reported that alteration of the growth plate rather than reactive bone formation precedes a cam-type deformity of the hip in athletes. Differences between IR90 and IR0 may potentially indicate femoroacetabular impingement.21 A limitation of this study was the lack of imaging to determine the source of hip ROM limitations. Further research on the relationship between IR90 and IR0 values and femoroacetabular impingement is needed. Fuss and Bacher11 and Wagner et al25 reported that the superior ischiofemoral ligament restricts internal rotation of the hip. However, this ligament spirals in a proximolateral direction across the superior aspect of the femoral neck to attach to the base of the greater trochanter and is lax during hip flexion. Therefore, the superior ischiofemoral ligament acts to restrict internal rotation of the hip more in IR0 than in IR90. Since the normal group in the current study showed no significant difference between IR0 and IR90, and there was also no significant difference between the normal group and the pain group in SLR, hip ROM restrictions do not appear to be because of tightness of the hamstrings but rather tightness in the muscles around the hip, especially the gluteus maximus and other external rotator muscles of the hip. It is likely that the factors that most restricted IR90 in the pain group were femoroacetabular impingement or tightness in the muscles that extend and externally rotate the hip.
This study had some limitations. Because it was a cross-sectional study, it remains unclear whether hip ROM limitations came before or after elbow pain. However, if playing baseball induced hip ROM limitations, then the normal group should show ROM reductions similar to those seen in the pain group. Hip flexion and IR90 were significantly restricted in the pain group relative to the normal group. Thus, it does not seem that playing baseball induces hip ROM limitations in all players. In players that do have hip ROM limitations, we need to determine when this limitation occurred relative to the onset of elbow pain. If players acquired hip ROM limitations through compensation to avoid pain during pitching, then we need to primarily treat the painful throwing elbow. However, if hip ROM limitations occurred before throwing elbow pain, then improving hip ROM might help to prevent injury to the throwing elbow. Further research is needed to clarify the chronology of the relationship between throwing elbow pain and hip ROM limitations.
Differences that occur with changing hip position are unique to every generation.7,12,19 Studies have yet to prove that poor pitching mechanics increase the risk of injury to young pitchers4,15; however, Davis et al4 reported that incorrect performance of multiple biomechanical pitching parameters increased elbow valgus load. The throwing motion is a complicated process; thus, it is difficult to evaluate risk parameters with any certainty. However, if aging (a risk factor for throwing elbow injury) is related not only to different loading stresses but also to the physical changes associated with increasing age, then physical features such as differences between IR0 and IR90 may help identify players who are susceptible to throwing elbow injury. The participants in the current study were adolescents, many of whom may have been going through a growth spurt. As part of the normal growth process, elongation of the musculotendinous units occurs as a secondary response to the increase in length that takes place in the long bones at their growth plates. During an adolescent growth spurt, this creates tightness and inflexibility across the joints as the lengthening of the musculotendinous unit lags behind that of the bone itself.3 This imbalance between musculotendinous units and bone may be a cause of tightness around the hip joint. However, in this study, we did not record the number of years of baseball experience or changes in height of the participants. Further research is needed to confirm a relationship between throwing elbow pain and rapid growth. If a relationship between rapid growth and hip ROM is confirmed, then baseball players can easily be screened for hip ROM limitations as these measurements are easy to do and require no special tools. This could provide a means of identifying players at risk of throwing elbow injury. To confirm the relationship between changes to ROM in hip positions and throwing elbow pain, a longitudinal study is required.
Conclusion
We examined differences in hip ROM between adolescent baseball players with and without throwing elbow pain. The results suggest that limitations of hip flexion and IR90 may identify players at risk of a painful throwing elbow. Differences between IR0 and IR90 may be an important indication of players who require intervention to prevent elbow injury.
Acknowledgment
The authors thank Keika Hoshi (Kitasato Clinical Research Center) for support with statistical calculations.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
References
- 1. Boone DC, Azen SP. Normal range of motion of joints in male subjects. J Bone Joint Surg Am. 1979;61:756–759. [PubMed] [Google Scholar]
- 2. Boone DC, Azen SP, Lin CM, Spence C, Baron C, Lee L. Reliability of goniometric measurements. Phys Ther. 1978;58:1355–1390. [DOI] [PubMed] [Google Scholar]
- 3. Dalton SE. Overuse injuries in adolescent athletes. Sports Med. 1992;13:58–70. [DOI] [PubMed] [Google Scholar]
- 4. Davis JT, Limpisvasti O, Fluhme D, et al. The effect of pitching biomechanics on the upper extremity in youth and adolescent baseball pitchers. Am J Sports Med. 2013;37:1484–1491 [DOI] [PubMed] [Google Scholar]
- 5. Dillman CJ, Fleisig GS, Andrew JR. Biomechanics of pitching with emphasis upon shoulder kinematics. J Orthop Sports Phys Ther. 1993;18:402–408. [DOI] [PubMed] [Google Scholar]
- 6. Ellenbecker TS, Ellenbecker GA, Roetert EP, Silva RT, Keuter G, Sperling F. Descriptive profile of hip rotation range of motion in elite tennis players and professional baseball pitchers. Am J Sports Med. 2007;35:1371–1376. [DOI] [PubMed] [Google Scholar]
- 7. Ellison JB, Rose SJ, Sahrmann SA. Patterns of hip rotation range of motion: a comparison between healthy subjects and patients with low back pain. Phys Ther. 1990;70:537–541. [DOI] [PubMed] [Google Scholar]
- 8. Fleisig GS, Andrews JR, Dillman CJ, Escamilla RF. Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med. 1995;23:233–239. [DOI] [PubMed] [Google Scholar]
- 9. Fleisig GS, Barrentine SW, Zheng N, Escamilla RF, Andrews JR. Kinematic and kinetic comparison of baseball pitching among various levels of development. J Biomech. 1999;32:1371–1375. [DOI] [PubMed] [Google Scholar]
- 10. Fleisig GS, Escamilla RF, Barrentine SW. Biomechanics of pitching: mechanism and motion analysis In: JR Andrews, B Zarins, KE Wilk, eds. Injuries in Baseball. Philadelphia, PA: Lippincott-Raven; 1998:3–22. [Google Scholar]
- 11. Fuss FK, Bacher A. New aspects of the morphology and function of the human hip joint ligament. Am J Anat. 1991;192:1–13. [DOI] [PubMed] [Google Scholar]
- 12. Kouyoumdjian P, Coulomb R, Sanchez T, Asencio G. Clinical evaluation of hip joint rotation range of motion in adults. Orthop Traumatol. 2012;98:17–23. [DOI] [PubMed] [Google Scholar]
- 13. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159–174. [PubMed] [Google Scholar]
- 14. Laudner KG, Moore SD, Sipes RC, Meister K. Functional hip characteristics of baseball pitchers and position players. Am J Sports Med. 2010;38:383–387. [DOI] [PubMed] [Google Scholar]
- 15. Lyman S, Fleisig GS, Andrews JR, Osinski ED. Effect of pitch type, pitch count and pitching mechanics on risk of elbow and shoulder pain in youth baseball pitchers. Am J Sports Med. 2002;30:463–468. [DOI] [PubMed] [Google Scholar]
- 16. Neusel E, Bierther B, Fuss B, Blasius K. Hip joint congruence: experimental studies. Acta Orthop Trauma Surg. 1996;115:321–324. [DOI] [PubMed] [Google Scholar]
- 17. Pappas AM. Elbow problem associated with baseball during childhood and adolescence. Clin Orthop Relat Res. 1982;(164):30–41. [PubMed] [Google Scholar]
- 18. Petty DH, Andrews JR, Fleisig GS, Cain EL. Ulnar collateral ligament reconstruction in high school baseball players: clinical results and injury risk factors. Am J Sports Med. 2004;32:1158–1164. [DOI] [PubMed] [Google Scholar]
- 19. Sankar WN, Laird CT, Baldwin KD. Hip range of motion in children: what is normal? J Pediatr Orthop. 2012;32:399–405. [DOI] [PubMed] [Google Scholar]
- 20. Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull. 1979;86:420–428. [DOI] [PubMed] [Google Scholar]
- 21. Siebenrock KA, Bohning A, Mamisch TC, Schwab M. Growth plate alteration precedes cam-type deformity in elite basketball players. Clin Orthop Relat Res. 2013;471:1084–1091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Stodden DF, Fleisig GS, McLean SP, Lyman SL, Andrews JR. Relationship of pelvis and upper torso kinematics to pitched baseball velocity. J Appl Biomech. 2001;17:164–172. [Google Scholar]
- 23. Stodden DF, Langendorfer SJ, Fleisig GS, Andrews JR. Kinematic constraints associated with the acquisition of overarm throwing part 1: step and trunk actions. Res Q Exerc Sport. 2006;77:417–427. [DOI] [PubMed] [Google Scholar]
- 24. Tippett SR. Lower extremity strength and active range of motion in college baseball pitchers: a comparison between stance leg and kick leg. J Orthop Sports Phys Ther. 1986;8:10–14. [DOI] [PubMed] [Google Scholar]
- 25. Wagner FV, Negrão JR, Campos J, et al. Capsular ligaments of the hip: anatomic, histologic, and positional study in cadaveric specimens with MR arthrography. Radiology. 2012;263:189–198. [DOI] [PubMed] [Google Scholar]
- 26. Wight J, Richards J, Hall S. Influence of pelvis rotation styles on baseball pitching mechanics. Sports Biomech. 2004;3:67–83. [DOI] [PubMed] [Google Scholar]
- 27. Wilk KE, Meister K, Fleisig G, Andrews JR. Biomechanics of the overhead throwing motion. Sports Med Arthrosc Rev. 2000;8:124–134. [Google Scholar]