

Abstract
Background:
Tarsometatarsal (TMT) dislocations are uncommon yet debilitating athletic injuries, particularly in American football. To date, the mechanisms of athletic TMT dislocation have been described only anecdotally. This lack of information confounds the development of preventative countermeasures.
Purpose:
To use video analysis to provide direct, independent identification of the etiologic and mechanistic variables responsible for TMT dislocations in professional football players.
Study Design:
Case series; Level of evidence, 4.
Methods:
Sixteen professional National Football League players who sustained publicly reported TMT dislocations were identified. Publicly broadcast game footage of the plays in which injury occurred was reviewed by a panel of 5 biomechanists. Consensus was reached regarding the details surrounding injury, and a weighting was assigned to each detail based on the panel’s confidence.
Results:
Roughly 90% of injuries occurred while the injured player was engaged with or by another player, a detail that has heretofore been undocumented. Few injuries resulted from direct loading of either the foot or the ipsilateral limb; however, the injured foot was frequently subjected to axial loading from ground engagement with the foot in plantar flexion and the toes dorsiflexed. Injurious loading was often due to external rotation of the midfoot (86%). Fifteen of 16 injuries were season ending.
Conclusion:
TMT dislocations are frequently associated with engagement by or with a second player but infrequently caused by a direct blow to the foot. Axial loading of the foot, external rotation, and pronation/supination are the most common conditions during injurious loading.
Keywords: Lisfranc injury, tarsometatarsal dislocation, biomechanics, video analysis, professional football
The term tarsometatarsal (TMT) dislocation covers a spectrum of ligamentous injuries ranging in severity from mild midfoot sprains to frank dislocations.25 These injuries are commonly observed in sports, specifically in American football.22
While it has been estimated that only 3% of football players will suffer a TMT dislocation,17 this injury is responsible for a large amount of lost playing time. Mild midfoot sprains may require up to 1 month of recovery time.15,24 More serious dislocations may keep a player from athletic participation for 6 to 9 months if surgery is needed.9,14 In extreme cases, the injury may end an athlete’s career.12,16,21,29 Given the risk that these injuries pose to the careers and performance of professional football players, it is critical that the etiology and mechanisms of TMT dislocations be established to guide the development of protective countermeasures.31
Unfortunately, what little information exists regarding the mechanisms of injury in football results from either retrospective surveys24 or patient histories.8,9,14,15,26,30 Using these techniques, 2 main mechanisms have been identified in the literature: twisting and axial loading of the foot.24 The former can occur when a player pivots about a planted forefoot. It has been suggested that the second mechanism, which is also referred to as a “forced plantar flexion” injury,32 results from loading along the long axis of the foot, which raises the longitudinal arch and forces the midfoot into plantar flexion. This injurious loading may occur when a second player falls on the injured player’s foot or lower leg. Although these mechanisms are frequently described in the literature, the evidence supporting them is limited to player and trainer recollections.
There are at least 3 limitations to the use of retrospective surveys and patient interviews for data gathering. One inherent shortcoming is that the interviewee will have limited or incomplete knowledge of the injury event. These missing details may be pertinent to the cause or mechanism of injury. A second problem is the instability of memory: Not only can the quality of true memories degrade with time, but conflated or false memories can also be created.11,13,23 Finally, the respondent may have implicit biases that filter or distort their interpretation of events. Trainers, for example, because of their own experiences or reports in the scientific literature, may have preconceptions about the mechanism by which certain injuries occur. Therefore, while follow-up questionnaires are invaluable research tools, an independent third-party analysis of injury mechanisms is needed to corroborate otherwise anecdotal observations.
Video analysis has been frequently employed by researchers to provide independent information regarding injury mechanisms. Over the past decade, this technique has been applied successfully to identify etiologic and mechanistic injury information in sports as diverse as alpine skiing,7 Australian and American football,5,28 basketball,20 handball,27 ice/inline skating,18 lacrosse,10 soccer,1–4,6 and taekwondo.19 The advantages of this technique include the ability to replay and pause events, to magnify regions of interest for detailed examination, and to allow multiple observers to discuss and assess the level of evidence provided.
Furthermore, there is evidence to suggest that self-reported mechanisms and video analysis can yield significantly different evaluations of the injury scenario. Olsen et al27 found that specific details of an athlete’s account of his injury disagreed with video analysis in up to one third of cases. The greatest disagreement was associated with those details surrounding the role of others in the injury event, such as identifying whether contact with another player occurred (disagreement in 5 of 15 cases).27 Therefore, video analysis is a valuable complement to interview-based research regarding the biomechanics of injury, particularly in a sport such as football where multiple athletes may be involved in the injury event.
All of the existing information regarding athletic TMT dislocations relies on athlete or trainer recollections of the mechanism of injury. The goal of the current work is to use video analysis to identify the etiologic and mechanistic variables responsible for TMT dislocations in professional football players. Publicly broadcast game footage of the injury events was analyzed to determine the general circumstances surrounding injury, the position of the foot and ankle at the onset of injurious loading, and the nature of injurious loading. Descriptive statistics are presented based on raw and confidence-weighted analyses of the videos. Further illuminating the causes and mechanisms of TMT dislocations will facilitate the development of experimental models able to replicate and quantify these injuries in vitro, thereby enabling the development of interventions aimed at injury reduction.
Materials and Methods
An Internet search was performed for press releases describing National Football League (NFL) players who had sustained Lisfranc or TMT injuries during the years 2004 to 2009. A total of 16 players, along with the game in which the injury occurred, were identified in this manner. This represents a convenience sample. As this method of identification relied on publicly available information, no player consent was required.
The NFL season consists of 4 weeks of preseason and 17 weeks of regular season. Player game logs are available from the website NFL.com, which lists those games for which a player was active. These logs were used to confirm the date of injury (players were inactive in subsequent games) and to estimate the time loss due to injury based on the week in which the player returned. Since not all teams make the playoffs, these calculations terminated at the end of the regular season. If a player did not return, the injury was termed “season ending.” This method assumes that the failure to return to play was solely a function of the injury sustained. While this assumption fails to recognize that a player may not resume game participation for reasons unrelated to the injury, it provides a convenient method of estimating injury severity.
The NFL.com website also lists anthropometric data for current and former players. The reported heights and weights were used to calculate a body mass index (BMI) value for each player. This value should be viewed as an approximation, as it is unclear the extent to which the posted weight corresponded to the player’s weight on the date of injury. The player’s date of birth was used to calculate their age at the time of injury. Age, in days, when injured (date of injury minus date of birth) was divided by 365.25 to determine age in years. Average age, height, weight, and BMI are reported for the 16 players studied.
Broadcast footage was requested from the NFL of those games in which injuries occurred. Video analysis was performed by 5 biomechanical engineers with between 1 and 25 years of experience in the study of lower extremity injury mechanics. Each member of the 5-person panel contributed to a discussion of the video, and consensus was reached on the descriptions and confidence levels reported herein. Roxio VideoWave software (Santa Clara, California, USA) was used for all analyses as it allowed for slow motion frame-by-frame analysis of each video.
Video analysis of each player followed the same major steps. The play in which injury occurred was first isolated. Next, 1 or more candidate injury events were identified from that play. It should also be noted that 2 or more camera angles were typically available to assist in evaluation. Injury events were identified based on either abnormal foot motion or subsequent behavior that indicated an injury had occurred (eg, a player hobbling or favoring a foot). Three categories of data were then determined for each injury event: a general description of the injury mechanism, the position of the foot at the initiation of injurious loading, and the types of motion and loading experienced by the foot during the injury event. Each category had 3 to 8 descriptive variables that were identified from the videos. The definitions of the descriptive variables are given in Appendix A. Once all injuries had been coded in this way, these results of each descriptive variable were summarized to determine the most common injury scenarios.
The confidence of the panel in characterizing certain details from the videos was affected by a number of factors, including the available camera angles relative to the injured foot as well as difficulties in visualization due to obstruction. To deal with these complexities, a confidence weighting was assigned to each descriptive variable on a 4-point scale: 0 = unknown, 1 = possible, 2 = probable, and 3 = certain. The confidence weights for each descriptive variable were then summed to determine a weighted count to better reflect the confidence of the panel. Both the absolute and weighted analyses are reported.
An exemplar set of video images is shown in Appendix B along with the panel’s determinations for the descriptive variables and confidence weights for that case.
Results
Sixteen players were identified whose injuries covered the years 2004 to 2009. The positions of the players at the time of injury included 3 running backs, 3 defensive ends, 3 offensive lineman, 3 linebackers, 1 tight end, 1 cornerback, 1 safety, and 1 kickoff return player. Average player anthropometry is given in Table 1.
TABLE 1.
Average Anthropometry for the Study Participants (N = 16)
| Measure | Mean ± Standard Deviation |
|---|---|
| Age at injury, y | 27.4 ± 3.2 |
| Height, inches | 74.2 ± 2.5 |
| Weight, lbs | 250.5 ± 34.4 |
| Body mass index, kg/m2 | 31.9 ± 2.8 |
The injuries were distributed between the final week of the preseason and the 16th week of the regular season (mean, week 8). One of 16 players returned after missing 6 games. All other players did not return; these were deemed season-ending injuries. All 16 players did return to play in the following season: 14 during the preseason and 2 during the regular season.
While the play in which injury occurred could be determined easily (in all cases it was the injured player’s last active play), each play contains multiple actions and events that could be responsible for the injury. A unique injurious event was identified for 12 of 16 players; however, 2 equally probable potential events were identified in the game footage of 4 players. Therefore, a total of 20 candidate injury events were identified in the 16 sets of videos. The subsequent analysis treated all 20 events independently and did not consider the potential bias associated with using 2 events for some players.
A single camera angle was available in 1 case. All others had either 2 (n = 7 cases), 3 (n = 6 cases), or 4 (n = 3 cases) camera angles. The general mechanisms, the position of the foot and ankle at the initiation of injurious loading, as well as the nature of injurious loading were identified for all possible candidates (Tables 2-4).
TABLE 2.
General Injury Mechanismsa
| Mechanism | n (%) | Weighted n (%) |
|---|---|---|
| Direct blow to foot | ||
| Yes | 7 (35) | 16 (31) |
| No | 12 (60) | 36 (69) |
| Unknown | 1 (5) | |
| Direct loading of ipsilateral lower extremity, not on foot | ||
| Yes | 3 (15) | 6 (12) |
| No | 15 (75) | 42 (88) |
| Unknown | 2 (10) | |
| Player engaged/engaging with another player | ||
| Yes | 17 (85) | 45 (90) |
| No | 2 (10) | 5 (10) |
| Unknown | 1 (5) | |
aSee Appendix A.1 for definition of mechanisms. Values in boldface indicate the most common determinations for each descriptive variable.
TABLE 4.
Prominent Motion/Loading During Injurya
| Motion/Loading | n (%) | Weighted n (%) |
|---|---|---|
| Ankle flexion/extension | ||
| Plantar flexed | 1 (5) | 1 (5) |
| Neutral | 5 (25) | 11 (52) |
| Dorsiflexed | 7 (35) | 9 (43) |
| Unknown | 7 (35) | |
| Ankle inversion/eversion | ||
| Inverted | 0 (0) | 0 (0) |
| Neutral | 7 (35) | 13 (76) |
| Everted | 2 (10) | 4 (24) |
| Unknown | 11 (55) | |
| Ankle rotation | ||
| Internal | 0 (0) | 0 (0) |
| Neutral | 1 (5) | 2 (14) |
| External | 9 (45) | 12 (86) |
| Unknown | 10 (50) | |
| Axial twist of foot | ||
| Pronation | 6 (30) | 9 (47) |
| Neutral | 2 (10) | 3 (16) |
| Supination | 4 (20) | 7 (37) |
| Unknown | 8 (40) | |
| Toe flexion | ||
| Plantar flexed | 0 (0) | 0 (0) |
| Neutral | 6 (30) | 8 (35) |
| Dorsiflexed | 8 (40) | 15 (65) |
| Unknown | 7 (30) | |
| Ankle joint compression | ||
| Yes | 9 (45) | 15 (79) |
| No | 2 (10) | 4 (21) |
| Unknown | 9 (45) | |
| Ankle joint shear | ||
| Yes | 6 (30) | 7 (54) |
| No | 4 (20) | 6 (46) |
| Unknown | 10 (50) | |
| Force along long axis of foot | ||
| Yes | 8 (40) | 16 (73) |
| No | 5 (25) | 6 (27) |
| Unknown | 7 (35) | |
aSee Appendix A.3 for definitions of motion/loading. Values in boldface indicate the most common determinations for each descriptive variable.
The general mechanisms of injury are given in Table 2. For both the unweighted and weighted evaluation, more than half of the injuries did not involve direct loading of the foot or the ipsilateral lower extremity. By contrast, the vast majority of the injuries occurred while a player was either engaged by or engaging another player.
The foot positions at the initiation of injurious loading are given in Table 3. The most frequent initial position of the ankle (weighted count) was plantar flexion, although a neutral position was comparably frequent. Similarly, the long axis of the foot was most frequently oriented either vertically or obliquely relative to the field, with only 1 player sustaining injury with his foot parallel to the surface of the ground. Associated with this vertical or oblique foot orientation, the toes were frequently dorsiflexed. The foot was not often inverted or everted, nor was it often internally or externally rotated at the initiation of injurious loading. During loading, however, external rotation of the ankle was the most prominent motion (Table 4). The ankle joint was frequently in compression, and axial twisting of the foot (either pronation or supination) was also common. Though direct loading of the injured foot did not occur in the majority of cases, the injurious loading did involve axial forces along the foot resulting from the player pushing off the ground with that foot while engaged with another player.
TABLE 3.
Foot/Ankle Positions at Initiation of Injurious Loadinga
| Position | n (%) | Weighted n (%) |
|---|---|---|
| Ankle flexion/extension | ||
| Plantar flexed | 6 (30) | 12 (44) |
| Neutral | 8 (40) | 10 (37) |
| Dorsiflexed | 2 (10) | 5 (19) |
| Unknown | 4 (20) | |
| Ankle inversion/eversion | ||
| Inverted | 1 (5) | 1 (4) |
| Neutral | 14 (70) | 21 (91) |
| Everted | 1 (5) | 1 (4) |
| Unknown | 4 (20) | |
| Ankle rotation | ||
| Internal | 0 (0) | 0 (0) |
| Neutral | 10 (50) | 15 (60) |
| External | 6 (30) | 10 (40) |
| Unknown | 4 (20) | |
| Foot orientation | ||
| Vertical/oblique | 11 (55) | 19 (95) |
| Horizontal | 1 (5) | 1 (5) |
| Unknown | 8 (45) | |
aSee Appendix A.2 for definitions of foot positions. Values in boldface indicate the most common determinations for each descriptive variable.
Discussion
An analysis of 16 videos was performed to document etiologic and mechanistic variables associated with TMT dislocations in professional football players. Twenty candidate injury events were identified, and the general circumstances of injury, the position of the foot at the initiation of injurious loading, and the nature of the injurious loading were documented by consensus of a 5-member panel. The relative confidence of the panel for each detail was quantified on a scale of 0 (unknown) to 3 (certain).
The severity of the TMT injuries was evident in terms of the time loss due to injury. Only 1 of 16 players returned to play by the end of the season. Since the use of game logs for calculating time loss does not provide any insight into why the player did not participate, it does not eliminate the possibility that they were inactive for reasons unrelated to their injury. Nevertheless, it is reasonable to assume that the injury was the primary factor preventing participation, particularly since all players returned to play the following season. These details underscore the severity of these injuries and the need for establishing the causes and mechanisms of TMT dislocations.
One significant finding of the current study is the high frequency with which the injury event occurred while the player was engaged by or engaging with another player (Table 2). This engagement frequently caused the injured player to step awkwardly onto the injured foot, thereby generating off-axis foot loads superimposed on the axial force generated by ground contact. These off-axis loads were associated with several of the ankle and foot motions and loads most frequently observed when the injury occurred (viz, ankle flexion/extension, inversion/eversion, rotation, and shear and axial twist of the foot). In contrast, very few injuries resulted from direct loading of the foot or of the ipsilateral lower extremity. The current figures (35% or 31%) are consistent with the 38% of cases involving direct loading reported by Meyer et al.24 The fact that the prominence of player engagement has not been reported to date may reflect the poorer ability of athletes to accurately recall the roles of other players in an injury event.27
The injured player’s foot was most frequently oriented obliquely or near-vertically relative to the field, in a near-neutral ankle position, or with some degree of plantar flexion. This configuration suggests that a large component of force is oriented along the long axis of the foot during injurious loading. Therefore, while very little direct loading of the foot was observed, the current results do support the notion of axial loading as an important injury mechanism. The axial twisting mechanism described in the literature24 is also supported by the large number of cases involving pronation or supination (84%).
The limitations of the current work relate to the general limitations of video analyses. It can be difficult to visualize the foot at the moment of injury, particularly in a game such as football where players are often clustered together. Between 2 to 4 camera angles were available for 15 of 16 cases evaluated in this study. Although this improved the chance of clearly viewing the injury event, it could not completely eliminate all obstructions. It should also be noted that these cases represent a convenience sample. The degree to which they represent the population of NFL injuries is unknown; moreover, no conclusions about risk can be drawn.
All existing information regarding athletic TMT injuries has been based on athlete or trainer recollections.8,9,14,15,24,26,30 The video analyses described in the current work provide important independent, third-party information about the circumstances of injury. We feel that these 2 methods of information gathering are complementary. For example, we have already described how the 2 methods corroborate the importance of an axial twisting injury mechanism, yet the video analysis has also underscored the role of player engagement, which has not been highlighted in previous research. One way in which this information could be further synthesized in future studies would be to combine athlete interviews and video analysis. This was not possible in the current study as we did not have direct access to the injured players and the variable lengths of time that had passed might have affected their recall of the injury event. Nevertheless, future work should consider combining both methods of analysis to better improve our understanding of these debilitating injuries.
The current work has identified the general circumstances, initial foot position, and injurious loading that is likely to be responsible for generating TMT dislocations. The key contribution is the independent observation of injury rather than a post hoc determination based on the recollections and impressions of players or trainers. Future work must incorporate this information into studies designed to quantify the loads that generate injury. Such quantitative information is needed to devise interventions capable of reducing the incidence and severity of TMT dislocations in athletes.
Acknowledgment
The authors thank the National Football League (NFL) and the members of the Foot & Ankle Subcommittee of the NFL for funding, supporting, and providing valuable input to this study.
Appendix A
Definition of Terms Used in the Video Analysis
A.1 General injury mechanisms
Direct blow to foot: Did the injury event involve loading of the foot due to direct external contact with the foot itself?
Direct loading of ipsilateral lower extremity, not on foot: Did the injury event involve loading of the limb of the injured foot, but not of the foot itself?
Player engaged/engaging with another player: Was the injured player actively blocking or tackling, or being blocked or tackled, when the injury occurred?
A.2 Foot position at initiation of injurious loading
Ankle flexion/extension: Orientation of the ankle about the medial-lateral axis, described as plantarflexed, neutral, or dorsiflexed.
Ankle inversion/eversion: Orientation of the ankle about the anterior-posterior axis, described as inverted, neutral, or everted.
Ankle rotation: Orientation of the ankle about the inferior-superior axis, described as internally rotated, neutral, or externally rotated.
Foot orientation: The position of the foot relative to the playing surface in the sagittal plane. Horizontal reflects a fully or nearly fully planted foot, while vertical/oblique describes a foot with toe planted and heel raised.
A.3 Motion/loading during injury
Ankle flexion/extension: Motion of the ankle about the medial-lateral axis, described as plantar flexed, neutral, or dorsiflexed.
Ankle inversion/eversion: Motion of the ankle about the anterior-posterior axis, described as inverted, neutral, or everted.
Ankle rotation: Motion of the ankle about the inferior-superior axis, described as internally rotated, neutral, or externally rotated.
Axial twist of foot: Angular motion of the forefoot relative to the hindfoot, described as pronation, neutral, or supination.
Toe flexion: Motion of the toes relative to the midfoot, described as either plantar flexed, neutral, or dorsiflexed.
Ankle joint compression: Was the ankle joint loaded primarily in compression?
Ankle joint shear: Was the ankle joint loaded primarily in shear?
Force along long axis of foot: Was the ground reaction force vector oriented primarily along the long axis of the foot? This axial force was not necessarily caused by a direct blow to the foot.
Appendix B
Exemplar Set of Video Images and Data Generated by the Panel
Narrative
Player sustained a Lisfranc injury of his right foot and missed 6 games. Two video views were available for analysis: (1) an oblique lateral view and (2) an oblique isolation view (Figure B1). Player lines up in a 3-point stance with his left foot forward at the left end of the defensive line. As he starts to rush the quarterback he is engaged by the right offensive tackle. As he attempts to go left around the blocker, his right foot loads the ground in a plantar-flexed orientation, and the injury appears to result from a ground reaction force on the foot in this position. In addition to a component down the long axis of the foot, the ground reaction force is oriented to cause external rotation, eversion, and pronounced dorsiflexion of the ankle and pronation of the forefoot. There was no direct contact to the foot from another player.
Figure B1.

Sample images from 2 camera views illustrating Lisfranc injury to the right foot: (A) the player approaches the blocker and prepares to go left, (B) the player engages the blocker and cuts left, (C) the right foot crosses behind the left, striking the ground in a plantar-flexed, slightly externally rotated position, and (D) the ground reaction forces and player engagement cause the right ankle to evert, externally rotate, and dorsiflex and causes the forefoot to pronate. Images used with the permission of the National Football League (NFL).
General Description of Mechanism:
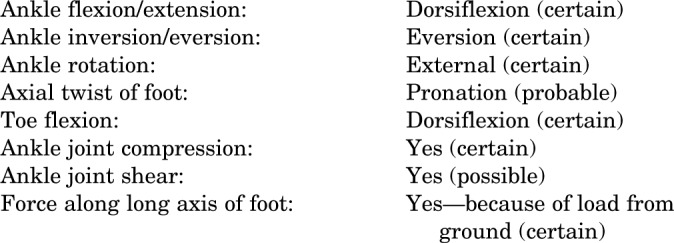
Plantar-flexed foot is loaded by the ground through the ball of the foot. In addition to a component down the long axis of the foot, the ground reaction force is oriented to cause external rotation, eversion, and pronounced dorsiflexion of the ankle and pronation of the forefoot.
General Injury Mechanisms:

Foot Position at Initiation of Injurious Loading:
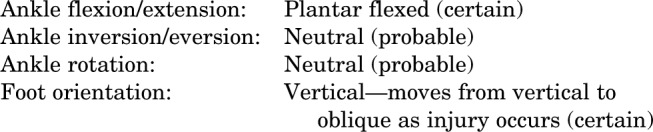
Motion/Loading During Injury:
Footnotes
One or more of the authors declared the following potential conflicts of interest or source of funding: The National Football League provided funding for this study. Financial support for the study was also provided by Biomechanics Consulting and Research (BioCore) LLC; this sponsorship covered a portion of the salary of the study authors. R.W.K. and J.R.C. are principals of BioCore LLC.
References
- 1. Andersen TE, Árnason Á, Engebretsen L, Bahr R. Mechanisms of head injuries in elite football. Br J Sports Med. 2004;38:690–696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Andersen TE, Floerenes TW, Arnason A, Bahr R. Video analysis of the mechanisms for ankle injuries in football. Am J Sports Med. 2004;32 (suppl):69S–79S. [DOI] [PubMed] [Google Scholar]
- 3. Andersen TE, Larsen Ø, Tenga A, Engebretsen L, Bahr R. Football incident analysis: a new video based method to describe injury mechanisms in professional football. Br J Sports Med. 2003;37:226–232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Andersen TE, Tenga A, Engebretsen L, Bahr R. Video analysis of injuries and incidents in Norwegian professional football. Br J Sports Med. 2004;38:626–631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Appleby B, Dawson B. Video analysis of selected game activities in Australian Rules Football. J Sci Med Sport. 2002;5:129–142. [DOI] [PubMed] [Google Scholar]
- 6. Arnason A, Tenga A, Engebretsen L, Bahr R. A prospective video-based analysis of injury situations in elite male football: football incident analysis. Am J Sports Med. 2004;32:1459–1465. [DOI] [PubMed] [Google Scholar]
- 7. Bere T, Flørenes TW, Krosshaug T, et al. Mechanisms of anterior cruciate ligament injury in World Cup alpine skiing: a systematic video analysis of 20 cases. Am J Sports Med. 2011;39:1421–1429. [DOI] [PubMed] [Google Scholar]
- 8. Berg JH, Silveri CP, Harris M. Variant of the Lisfranc fracture-dislocation: a case report and review of the literature. J Orthop Trauma. 1998;12:366–369. [DOI] [PubMed] [Google Scholar]
- 9. Bloome DM, Clanton TO. Treatment of Lisfranc injuries in the athlete. Tech Foot Ankle Surg. 2002;1:94–101. [Google Scholar]
- 10. Caswell SV, Lincoln AE, Almquist JL, Dunn RE, Hinton RY. Video incident analysis of head injuries in high school girls’ lacrosse. Am J Sports Med. 2012;40:756–762. [DOI] [PubMed] [Google Scholar]
- 11. Cohen G, Java R. Memory for medical history: accuracy of recall. Appl Cognit Psychol. 1995;9:273–288. [Google Scholar]
- 12. Curtis MJ, Myerson M, Szura B. Tarsometatarsal joint injuries in the athlete. Am J Sports Med. 1993;21:497–502. [DOI] [PubMed] [Google Scholar]
- 13. Gonsalves B, Paller KA. Mistaken memories: remembering events that never happened. Neuroscientist. 2002;8:391–395. [DOI] [PubMed] [Google Scholar]
- 14. Harwood MI, Raikin SM. A Lisfranc fracture-dislocation in a football player. J Am Board Fam Med. 2003;16:69–72. [DOI] [PubMed] [Google Scholar]
- 15. Hummel CH, Lazenby TW, Geisler PR. Management of a stage III Lisfranc ligament injury in a collegiate football player: a case review. Athl Train Sports Health Care. 2011;3:95–99. [Google Scholar]
- 16. Kadel NJ, Donaldson-Fletcher EA. Lisfranc fracture-dislocation in a male ballet dancer during take-off of a jump: a case study. J Dance Med Sci. 2004;8:56–58. [Google Scholar]
- 17. Kaplan LD, Jost PW, Honkamp N, Norwig J, West R, Bradley JP. Incidence and variance of foot and ankle injuries in elite college football players. Am J Orthop (Belle Meade, NJ). 2011;40:40–44. [PubMed] [Google Scholar]
- 18. Knox CL, Comstock RD. Video analysis of falls experienced by paediatric iceskaters and roller/inline skaters. Br J Sports Med. 2006;40:268–271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Koh JO, Watkinson EJ, Yoon Y-J. Video analysis of head blows leading to concussion in competition Taekwondo. Brain Inj. 2004;18:1287–1296. [DOI] [PubMed] [Google Scholar]
- 20. Krosshaug T, Nakamae A, Boden BP, et al. Mechanisms of anterior cruciate ligament injury in basketball: video analysis of 39 cases. Am J Sports Med. 2007;35:359–367. [DOI] [PubMed] [Google Scholar]
- 21. Lattermann C, Goldstein JL, Wukich DK, Lee S, Bach BR., Jr Practical management of Lisfranc injuries in athletes. Clin J Sports Med. 2007;17:311–315. [DOI] [PubMed] [Google Scholar]
- 22. Lievers WB, Frimenko RE, Crandall JR, Kent RW, Park JS. Age, sex, causal and injury patterns in tarsometatarsal dislocations: a literature review of over 2000 cases. Foot. 2012;22:117–124. [DOI] [PubMed] [Google Scholar]
- 23. Mannan JB, Wieshmann UC. How accurate are witness descriptions of epileptic seizures? Seizure. 2003;12:444–447. [DOI] [PubMed] [Google Scholar]
- 24. Meyer SA, Callaghan JJ, Albright JP, Crowley ET, Powell JW. Midfoot sprains in collegiate football players. Am J Sports Med. 1994;22:392–401. [DOI] [PubMed] [Google Scholar]
- 25. Myerson MS, Cerrato RA. Current management of tarsometatarsal injuries in the athlete. J Bone Joint Surg Am. 2008;90:2522–2533. [PubMed] [Google Scholar]
- 26. O’Regan DJ. Lisfranc dislocations. J Med Soc NJ. 1969;66:575–577. [PubMed] [Google Scholar]
- 27. Olsen O-E, Myklebust G, Engebretsen L, Bahr R. Injury mechanisms for anterior cruciate ligament injuries in team handball: a systematic video analysis. Am J Sports Med. 2004;32:1002–1012. [DOI] [PubMed] [Google Scholar]
- 28. Pellman EJ, Viano DC, Tucker A, Casson IR, Waeckerle JF. Concussion in professional football: reconstruction of game impacts and injuries. Neurosurgery. 2003;53:799–814. [DOI] [PubMed] [Google Scholar]
- 29. Rajapakse B, Edwards A, Hong T. A single surgeon’s experience of treatment of Lisfranc joint injuries. Injury. 2006;37:914–921. [DOI] [PubMed] [Google Scholar]
- 30. Sauers RJ, Dilorio EJ, Weiss CB., Jr A Lisfranc’s fracture-dislocation in a collegiate football player. J Athl Train. 1992;27:24–25. [PMC free article] [PubMed] [Google Scholar]
- 31. van Mechelen W, Hlobil H, Kemper HCG. Incidence, severity, aetiology and prevention of sports injuries: a review of concepts. Sports Med. 1992;14(2):82–99. [DOI] [PubMed] [Google Scholar]
- 32. Wiley JJ. The mechanism of tarso-metatarsal joint injuries. J Bone Joint Surg Br. 1971;53:474–482. [PubMed] [Google Scholar]