

Abstract
Background:
Osteochondritis dissecans (OCD) of the capitellum is a well-recognized cause of elbow pain and disability in adolescent athletes. However, little is known about the prevalence of OCD in adolescent baseball players.
Purpose:
To determine the prevalence of OCD in baseball players aged 10 to 12 years based on ultrasonographic findings and to investigate the clinical characteristics of those with OCD lesions.
Study Design:
Descriptive epidemiology study.
Methods:
A total of 1040 players aged 10 to 12 years completed a questionnaire, ultrasound imaging, and radiographic examination to investigate OCD. Sonographic findings were classified into 5 grades (0, 1a, 1b, 2, and 3). Subjects with grade 1a, 1b, 2, or 3 were considered to have abnormal findings of the capitellum and were advised to undergo radiography. Radiographic and ultrasonographic findings were then compared. The prevalence of OCD was calculated, and differences by age and player position were determined.
Results:
Of the 1040 players, 33 (3.2%) had an abnormal finding on initial ultrasonography screening, and all 33 agreed to undergo radiography. Of them, 22 (66.7%) were found to have OCD of the capitellum on radiographs, giving an overall prevalence of 2.1%. Seven subjects (31.8%) had no history of elbow pain. Based on the radiographic classification, 20 subjects (90.9%) had stage I lesions. Analysis of OCD by age and player position revealed no significant differences.
Conclusion:
The prevalence of OCD of the capitellum was 2.1% in 1000 baseball players aged 10 to 12 years, with no differences in prevalence according to age or player position.
Keywords: osteochondritis dissecans, capitellum, ultrasonography, baseball
Osteochondritis dissecans (OCD) of the capitellum is a well-recognized cause of elbow pain and disability in adolescent athletes. This condition is more common in males than in females, and its prevalence is high among individuals who have played baseball since childhood.1 Repetitive throwing is considered to be one of the main etiological factors of this disease,1,2,4,10 although the exact etiology remains unclear.
Matsuura et al12 reported that OCD can be classified into 3 stages based on radiographic findings: stage I (radiolucent area), stage II (nondisplaced fragments), and stage III (loose bodies and sclerotic changes). Conservative treatment induced healing in 90.5% of patients with stage I lesions and in 52.9% of those with stage II lesions,12 suggesting that OCD can be successfully treated conservatively if treatment is started early. Furthermore, prevention seems to be of the utmost importance due to the lack of scientific evidence directing the management of this condition. To develop preventive strategies for OCD of the capitellum, its magnitude and origins must be clarified.
Nielsen13 investigated the prevalence of OCD of the capitellum and found an overall prevalence of 41 per 1000 workers aged 15 years or older. Little is known about the prevalence of OCD in adolescent baseball players, however. Previous studies have reported that patients with OCD are typically aged 11 to 21 years.3,14,15 In a previous study of ours,12 the average age at which stage I OCD was diagnosed was 11.5 years, suggesting a typical age range for prevalence of 10 to 12 years in baseball players. It is difficult to detect early-stage OCD because most of the patients are asymptomatic or minimally symptomatic. Ultrasound imaging, which is a safe, inexpensive, and portable type of diagnostic imaging, has been used to assess elbow injuries.7,16,17 Harada et al7 found it to be a useful tool for detecting elbow injuries because the reliability of abnormal ultrasonographic findings was confirmed by radiography.
The purpose of this study was to determine the prevalence of OCD, as detected on ultrasonography, in baseball players aged 10 to 12 years and to investigate the clinical characteristics of those found to have OCD lesions.
Materials and Methods
The Institutional Review Board of Tokushima University Hospital approved the study protocol, and all parents and coaches provided informed consent.
All 1040 baseball players aged 10 to 12 years (mean, 10.7 years), who participated in the regional summer championship in July 2011, completed a questionnaire and underwent ultrasonographic and radiographic examinations to investigate the presence and characteristics of OCD. Of 1040 players, 1006 were male and 34 female. Questionnaires were distributed to team coaches, and the subjects answered the questions with the assistance of their coaches and/or parents. Questionnaire items included age, player position, and any past episodes of elbow pain. The first author (T.M.) then reviewed the questionnaire with individual subjects to increase their understanding of the questions and the accuracy of the responses provided.
Both elbows of each subject were sonographically examined in the field. Ultrasonography of the lateral aspect of the elbow was performed by 2 of the authors (N.S., an orthopaedic surgeon, and S.N., an ultrasonography technician) using the following equipment: a FAZONE M sonography diagnostic imaging system (ZONARE Medical Systems Inc) with a 5- to 10-MHz linear array transducer (FAZONE CB; Fujifilm Corp), the MyLabFive portable ultrasound system (Esaote Europe BV) with a 6- to 18-MHz linear array transducer, and the M-Turbo ultrasound system (SonoSite Inc) with a 6- to 13-MHz linear array transducer. Anterior view images were taken with the subject seated and the elbow fully extended. Posterior view images were taken with the elbow fully flexed to obtain sufficient view of the anterior aspect of the capitellum. Sonographic findings were graded as follows according to a modification of the classification proposed by Ishizaki8: grade 0, normal (Figure 1A); grade 1a, irregular surface of subchondral bone (Figure 1B); grade 1b, a cystic lesion of the subchondral bone surface (Figure 1C); grade 2, irregularity of the subchondral bone (Figure 1D); and grade 3, discontinuity of the subchondral bone (Figure 1E). We defined grades 1a, 1b, 2, and 3 as abnormal findings of the capitellum. We then recommended radiographic examination to those subjects with abnormal ultrasonographic findings.
Figure 1.

Sonographic classification of osteochondritis dissecans of the capitellum. (A) Grade 0 is normal, (B) grade 1a shows an irregular surface on the subchondral bone, (C) grade 1b shows a cystic lesion on the subchondral bone surface, (D) grade 2 shows irregularity of the subchondral bone, and (E) grade 3 shows discontinuity of the subchondral bone.
Radiography of the elbow was performed in 4 directions: anteroposterior with the elbow extended, anteroposterior with the elbow flexed at 45°, lateral, and oblique. Two of the authors (T.M. and T.I.) then compared the radiographic and ultrasonographic findings and diagnosed the radiographic stage using the classification of Matsuura et al.12
The prevalence of OCD was calculated separately for age and player position and was expressed as a percentage. The chi-square test was used to determine whether the prevalence rate differed by age and player position. All tests were 2-sided, and P < .05 was regarded as significant.
Results
Of the 1040 players, 1007 (96.8%) had grade 0 (normal) findings in the throwing arm. Of them, 437 (43.4%) had history of elbow pain. Thirty-three (3.2%) had an abnormal finding on initial ultrasonography screening. Grade 1a was seen in 6 elbows (0.6%), grade 1b in 7 (0.7%), grade 2 in 11 (1.0%), and grade 3 in 9 (0.9%). A total of 1037 (99.7%) had grade 0 in the nonthrowing side. Only 3 players (0.3%) had a grade 1b lesion, and they had the same grade 1b lesion on the throwing side. All 33 subjects who had ultrasonographic abnormalities were male, and all agreed to undergo radiography. Of them, OCD of the capitellum was evident in 22 (66.7%) on the throwing side on radiography. Three subjects (9.1%) had a cystic lesion on both sides, and 8 (24.2%) had a normal appearance. Of the 11 players with cystic or normal appearance, 5 (45.5%) had experienced elbow pain in the throwing side. Table 1 shows the details of the ultrasonographic and radiographic findings in the throwing arm. The 3 cystic lesions were monitored by follow-up radiography, and in all 3 cases, the lesions decreased in size with no evidence of OCD (Figure 2). The 8 subjects with a normal appearance on the initial radiographic examination were monitored for 2 years, but none showed signs of OCD. The overall prevalence of OCD of the capitellum was 2.1%.
TABLE 1.
Details of Ultrasonographic and Radiographic Findings in Subjects With OCD: Throwing Sidea
| Stage | OCD | Cystic Lesion | Normal |
|---|---|---|---|
| 1a | 4 | 0 | 2 |
| 1b | 0 | 2 | 5 |
| 2 | 10 | 0 | 1 |
| 3 | 8 | 1 | 0 |
aOCD, osteochondritis dissecans of the capitellum.
Figure 2.
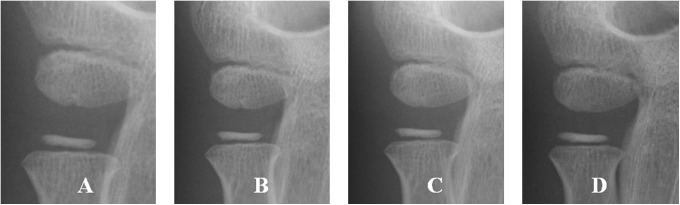
Anteroposterior view on radiography with the elbow flexed at 45° during follow-up in a representative case of cystic lesion. The lesion decreased in size over time, and no osteochondritis dissecans was evident. (A) Initial examination and examinations at (B) 1 month, (C) 4 months, and (D) 6 months later.
The characteristics of the OCD subjects are listed in Table 2. Fifteen (68.2%) had experienced elbow pain. Based on our radiographic classification, 20 had stage I lesions and 2 had stage II lesions. Tables 3 and 4 show the occurrence of OCD by age and player position, respectively, with no significant differences for either factor (P = .810 for age, P = .224 for position).
TABLE 2.
Characteristic of Patients With Osteochondritis Dissecans of the Capitellum
| Patient No. | Age, y | Position | Elbow Pain | Radiographic Stage |
|---|---|---|---|---|
| 1 | 10 | Catcher | – | I |
| 2 | 10 | Catcher | + | I |
| 3 | 10 | Infielder | – | I |
| 4 | 10 | Infielder | + | I |
| 5 | 10 | Infielder | + | I |
| 6 | 10 | Infielder | + | I |
| 7 | 10 | Outfielder | – | I |
| 8 | 10 | Outfielder | + | I |
| 9 | 10 | Outfielder | + | I |
| 10 | 11 | Pitcher | – | I |
| 11 | 11 | Pitcher | + | I |
| 12 | 11 | Catcher | – | I |
| 13 | 11 | Catcher | + | I |
| 14 | 11 | Infielder | – | I |
| 15 | 11 | Infielder | + | I |
| 16 | 11 | Infielder | + | II |
| 17 | 11 | Outfielder | + | I |
| 18 | 11 | Outfielder | + | II |
| 19 | 12 | Pitcher | – | I |
| 20 | 12 | Catcher | + | I |
| 21 | 12 | Infielder | + | I |
| 22 | 12 | Infielder | + | I |
TABLE 3.
OCD by Agea
| Age, y | No. of Participants | Cases of OCD, n (%) |
|---|---|---|
| 10 | 496 | 9 (1.8) |
| 11 | 379 | 9 (2.4) |
| 12 | 165 | 4 (2.4) |
aOCD, osteochondritis dissecans of the capitellum.
TABLE 4.
OCD by Player Positiona
| Player Position | No. of Participants | Cases of OCD, n (%) |
|---|---|---|
| Pitcher | 123 | 3 (2.4) |
| Catcher | 110 | 5 (4.6) |
| Infielder | 426 | 9 (2.1) |
| Outfielder | 381 | 5 (1.3) |
aOCD, osteochondritis dissecans of the capitellum.
Discussion
This is the first study to report specifically on the prevalence of OCD of the capitellum in baseball players aged 10 to 12 years based on ultrasonographic findings. The overall prevalence of OCD in this study was 2.1%. OCD of the capitellum is a disorder commonly seen in young, male baseball players. However, only a few studies have examined the prevalence rate specifically in this population. In 1976, Gugenheim et al5 surveyed 549 Little League pitchers aged 9 to 13 years and identified no cases of OCD on radiography. Larson et al9 evaluated 120 Little League pitchers aged 11 to 12 years and found radiographic changes in the capitellum or radial head in 5% of the subjects. Hang et al6 studied 343 Little League pitchers, catchers, and fielders aged 9 to 12 years and found OCD in 1 player (0.3%) on radiography. As with any musculoskeletal injury or disease, an improved understanding of the risk factors and populations at risk is essential before any preventive strategies can be developed and employed. Therefore, in this study we sought to formally determine the incidence and characteristics of OCD in young baseball players.
Radiographic screening is associated with radiation exposure. On the other hand, ultrasound imaging, where there is no exposure to radiation, is an inexpensive and portable type of diagnostic imaging that has been successfully used to assess elbow injuries.7,16,17 In a study of 35 young baseball players, Harada et al7 found ultrasonography useful and reliable (as confirmed against radiographic findings) for detecting elbow injuries. They conducted ultrasonography at the baseball practice field and found 2 cases of OCD (1.3%) among 153 players aged 9 to 12 years.7 The prevalence of OCD in our study (2.1%) was higher than that reported by Harada et al7 (1.3%). However, it is difficult to compare our results with those of Harada et al7 because our study did not include 9-year-old players and because our players had a higher number of practicing hours due to the warmer climate in Tokushima, which allows baseball to be a year-round sport. Nielsen13 reported a prevalence of over 4% in workers aged 15 years or older. Although his study investigated a great number of materials, the study participants were biased; 10% were patients with problems other than their joints, and 90% were friends or family visiting patients in the hospital. This is the reason why the prevalence rate in our study was lower than that of Nielsen.13
Of the 22 subjects with OCD, 7 (31.8%) had not experienced any episodes of elbow pain. If ultrasonography of the lateral aspect of the elbow had not been performed, OCD in these subjects would not have been detected. Therefore, our results indicate that ultrasonography has good potential for detecting asymptomatic or minimally symptomatic OCD. Furthermore, 20 of 22 subjects (90.9%) with OCD had a stage I lesion based on radiographic findings. A previous study showed that conservative treatment produced healing in 90.5% of subjects with a stage I lesion.12 These results suggest that screening for OCD using ultrasonography is useful for early detection and provides an opportunity for successful conservative treatment.
Of the 20 players with grade 2 or 3 abnormal findings, OCD was confirmed in 18 (90%) on radiography. In contrast, of the 13 players with grade 1a or 1b (abnormal findings of only the subchondral surface), only 4 players (30.8%) showed OCD on radiography. Moreover, none of the subjects with grade 1b (cystic lesion) showed signs of OCD. These results suggest that a cystic appearance of the subchondral bone surface is a variation of normal development during ossification, although the pathogenesis is not clear. It is speculated that ultrasonographic abnormalities include OCD, minor injury, and normal development during ossification. Our results indicate that assessment on ultrasonography is useful, although not perfect; therefore, OCD should be confirmed on additional radiographic examination.
Our study is the first to compare the prevalence of OCD by age and player position. It was hypothesized that older age and pitchers carry an increased risk for OCD because of the higher athletic demands placed on older subjects and pitchers. In our study, however, no significant differences were found in the prevalence of OCD by age or player position. Additional studies are therefore needed to identify high-risk groups.
This study has several limitations. Although we confirmed the ultrasonographic abnormalities on plain radiography, radiography was not performed for those subjects with no abnormalities on ultrasonography. Therefore, the sensitivity of ultrasonography could not be determined, and the true incidence of OCD may have been underestimated. Another limitation is that pitch type, pitch count, pitching mechanics, and practice hours, which have been proposed as risk factors for throwing injuries,11 were not included in our analysis. Further studies are needed to elucidate the precise mechanism underlying OCD.
Conclusion
The prevalence of OCD of the capitellum on ultrasonography in over 1000 baseball players aged 10 to 12 years was 2.1%. About 30% of the subjects had not experienced elbow pain, and over 90% had early-stage OCD. No significant differences were observed in OCD prevalence by age or player position.
Acknowledgment
The authors thank Takenobu Iwase, MD, Department of Orthopaedic Surgery, Tokushima National Hospital, and Shinji Kashiwaguchi, MD, Department of Orthopaedic Surgery, Tokyo Kosei-nenkin Hospital, for their asssistance in this study.
Footnotes
The authors declared that they have no potential conflicts of interest in the authorship and publication of this contribution.
References
- 1. Adams JE. Injury to the throwing arm. A study of traumatic changes in the elbow joints of boy baseball players. Calif Med. 1965;102:127–132. [PMC free article] [PubMed] [Google Scholar]
- 2. Barnes DA, Tullos HS. An analysis of 100 symptomatic baseball players. Am J Sports Med. 1978;6:62–67. [DOI] [PubMed] [Google Scholar]
- 3. Bradley JP, Petrie RS. Osteochondritis dissecans of the humeral capitellum: diagnosis and treatment. Clin J Sports Med. 2001;20:565–590. [DOI] [PubMed] [Google Scholar]
- 4. Brown R, Blazina ME, Kerlan RK, Carter VS, Jobe FW, Carlson GJ. Osteochondritis of the capitellum. J Sports Med. 1974;2:27–46. [DOI] [PubMed] [Google Scholar]
- 5. Gugenheim JJ, Jr, Stanley RF, Woods GW, Tullos HS. Little League survey: the Houston study. Am J Sports Med. 1976;4:189–200. [DOI] [PubMed] [Google Scholar]
- 6. Hang DW, Chao CM, Hang YS. A clinical and roentgenographic study of Little League elbow. Am J Sports Med. 2004;32:79–84. [DOI] [PubMed] [Google Scholar]
- 7. Harada M, Takahara M, Sasaki J, Mura N, Ito T, Ogino T. Using sonography for the early detection of elbow injuries among young baseball players. AJR Am J Roentgenol. 2006;187:1436–1441. [DOI] [PubMed] [Google Scholar]
- 8. Ishizaki K. Significance and Utility of Ultrasonography. Baseball Elbow Osteochondritis Dissecans of the Capitellum [in Japanese] Tokyo, Japan: Zennihon Byoin Syuppankai; 2013. [Google Scholar]
- 9. Larson RL, Singer KM, Bergstrom R, Thomas S. Little League survey: the Eugene study. Am J Sports Med. 1976;4:201–209. [DOI] [PubMed] [Google Scholar]
- 10. Lindholm TS, Osterman K, Vankka E. Osteochondritis dissecans of the elbow, ankle and hip. A comparison survey. Clin Orthop Relat Res. 1980;(148):245–253. [PubMed] [Google Scholar]
- 11. Lyman S, Fleisig GS, Andrews JR, Osinski ED. Effect of pitch type, pitch count, and pitching mechanics on risk of elbow and shoulder pain in youth baseball pitchers. Am J Sports Med. 2002;30:463–468. [DOI] [PubMed] [Google Scholar]
- 12. Matsuura T, Kashiwaguchi S, Iwase T, Takeda Y, Yasui N. Conservative treatment for osteochondrosis of the humeral capitellum. Am J Sports Med. 2008;36:868–872. [DOI] [PubMed] [Google Scholar]
- 13. Nielsen NA. Osteochondritis dissecans capituli humeri. Acta Orthop Scand. 1933;4:307–418. [Google Scholar]
- 14. Pappas AM. Osteochondrosis dissecans. Clin Orthop Relat Res. 1981;(158):59–69. [PubMed] [Google Scholar]
- 15. Schenk RC, Jr, Goodnight JM. Osteochondritis dissecans. J Bone Joint Surg Am. 1996;78:439–456. [PubMed] [Google Scholar]
- 16. Takahara M, Ogino T, Tsuchida H, Takagi M, Kashiwa H, Nambu T. Sonographic assessment of osteochondritis dissecans of the humeral capitellum. AJR Am J Roentgenol. 2000;174:411–415. [DOI] [PubMed] [Google Scholar]
- 17. Takahara M, Shundo M, Kondo M, Suzuki K, Nambu T, Ogino T. Early detection of osteochondritis dissecans of the capitellum in young baseball players. Report of three cases. J Bone Joint Surg Am. 1998;80:892–897. [DOI] [PubMed] [Google Scholar]