

Abstract
Background:
Since their conception during the mid-1970s, international participation in extreme sports has grown rapidly. The recent death of extreme snowmobiler Caleb Moore at the 2013 Winter X Games has demonstrated the serious risks associated with these sports.
Purpose:
To examine the incidence and prevalence of head and neck injuries (HNIs) in extreme sports.
Study Design:
Descriptive epidemiological study.
Methods:
The National Electronic Injury Surveillance System (NEISS) was used to acquire data from 7 sports (2000-2011) that were included in the Winter and Summer X Games. Data from the NEISS database were collected for each individual sport per year and type of HNI. Cumulative data for overall incidence and injuries over the entire 11-year period were calculated. National estimates were determined using NEISS-weighted calculations. Incidence rates were calculated for extreme sports using data from Outdoor Foundation Participation Reports.
Results:
Over 4 million injuries were reported between 2000 and 2011, of which 11.3% were HNIs. Of all HNIs, 83% were head injuries and 17% neck injuries. The 4 sports with the highest total incidence of HNI were skateboarding (129,600), snowboarding (97,527), skiing (83,313), and motocross (78,236). Severe HNI (cervical or skull fracture) accounted for 2.5% of extreme sports HNIs. Of these, skateboarding had the highest percentage of severe HNIs.
Conclusion:
The number of serious injuries suffered in extreme sports has increased as participation in the sports continues to grow. A greater awareness of the dangers associated with these sports offers an opportunity for sports medicine and orthopaedic physicians to advocate for safer equipment, improved on-site medical care, and further research regarding extreme sports injuries.
Keywords: extreme sports, head and neck injuries, concussions, epidemiology
Over the past few decades, extreme sports has become a widely used phrase to describe a variety of nontraditional and adventure sports. The label has evolved to denote activities such as bungee jumping, snowboarding, extreme skiing, canyoning, surfing, skateboarding, skydiving, paragliding, rock climbing, and mountain bicycling.2,7,14,16,22 Several epidemiological studies have shown that since the conception of extreme sports in the 1960s, participation has grown exponentially.5,6 Extreme sports have been accepted as a separate and organized entity, as evidenced by the advent and rising popularity of the X Games, the introduction of slope-style snowboarding events into the Winter Olympics in 2014, and an increasing number of nationally televised events over the past decade. Extreme sports are believed to have a greater risk of injury compared with traditional sports. Currently, little evidence exists describing the injury rates for extreme sports due to their nontraditional, independent participation and lack of official regulation.5 Our preconception of an increased risk of injury and death with extreme sports necessitates the need to better understand injury rates and trends.3–5,22
Injury characteristics of extreme sports vary extensively due to their high-energy, high-risk nature.8,13 Specifically, head and neck injuries (HNIs) are of growing concern because of increased awareness of short- and long-term consequences reported in the literature.2,9,14,17,19 HNIs include concussions, fractures, and traumatic brain injuries (TBIs), which can result in outcomes such as chronic depression, headaches, paralysis, and death.9 Several articles have described injuries associated with extreme sports; however, they have primarily focused on mainstream activities such as snowboarding, snow skiing, and skateboarding. The objective of this study was to examine the epidemiology of HNI in 7 extreme sports over the past decade (2000-2011). The sports were selected based on their popularity and active status in the X Games (both winter and summer) and other major televised extreme sporting events. Our hypothesis was that there would be an increased rate of HNI over the 12-year time period and that concussions would be the most common HNI reported among the 7 extreme sports.
Methods
The National Electronic Injury Surveillance System (NEISS) of the Consumer Product Safety Commission (CPSC) was used to acquire data for this study from 2000 to 2011. The CPSC conducts yearly sampling frames of all active emergency departments in the United States, including information regarding the total number of emergency department visits. The NEISS is a national probability sample of 100 hospitals in the United States and its territories.1 Patient information is collected from each NEISS hospital for every emergency visit involving an injury associated with consumer products, such as sporting equipment. Data are updated on a daily basis, and any missing information is obtained by telephone interviews with patients within the first week after injury. From this sample, the total number of injuries treated in hospital emergency rooms nationwide can be estimated. The sampling procedure and the statistical basis for calculation of national estimates based on the NEISS data are validated approaches and described on the CPSC website. The derivation of sampling weights used by the NEISS is well established and used by researchers and government agencies.18 Sampling weights were applied to the NEISS data to account for selection, for number of annual emergency department visits for each hospital, and for hospitals that do not respond. After being weighted, the NEISS data provides estimates for the total number of specific consumer product–related sports injuries in the United States. Variables included in the standard NEISS case report are treatment date, sex, race, diagnostic category, body part injured, patient disposition, and location of injury. As a part of the Consumer Product Safety Mission, the NEISS database serves as a reliable and reproducible source for a wide range of epidemiological subjects.
Injuries associated with 7 extreme sports were identified and examined using the NEISS consumer product codes in this study: snowboarding (5031), snowmobiling (1290), surfing (1261), mountain biking (5033), motocross (5036), skateboarding (1333), and snow skiing (3283). Because of the way the NEISS categorizes their product codes, motocross included 2-wheeled, powered, off-road vehicles such as dirt bikes and trail bikes; mopeds and mini-bikes were excluded. Surfing included injuries related to windsurfing. Snow skiing included injuries related to downhill skiing, cross-country skiing, ski jacks, ski lifts, and snowshoes.
Four types of head injuries and 4 types of neck injuries were recorded for each extreme sport during the 12-year span. Concussion, contusions/abrasions, fractures, and lacerations were recorded for head injuries. Contusions/abrasions, fractures, lacerations, and strains/sprains were recorded for neck injuries.
The risk of concussion, neck fracture, and skull fracture were calculated using participation rates for extreme sports from the 2013 Outdoor Foundation Participation Report, which contained data from 2007 to 2012.15 The Outdoor Foundation is a not-for-profit organization focused on encouraging and enhancing the experiences of people in the outdoors. Annually, the organization conducts a series of online interviews and surveys to assess the participation in various outdoor sports. Similar to the NEISS database, a weighting technique was used to balance the data and accurately reflect the entire US population. For this study, we used participation figures from 2007 to 2011 for all Americans older than 6 years; limited data are available prior to 2007 for the 7 extreme sports.15 Of note, there were no data recorded by the Outdoor Foundation study for motocross.
For each NEISS injury case report, the activity and sampling weight were recorded. National estimates for extreme sports injuries were calculated by summing the sampling weights for all injury case reports within a specific sport. This was done for the different types of HNIs for each year from 2000 to 2011. Incidence rates and ratios were calculated only from years 2007 to 2011 using the injury statistics from the NEISS and the participation rates from the 2013 Outdoor Foundation report. Incidence rates and incidence rate ratios were calculated for all extreme sports except motocross, since the Outdoor Foundation does not include participation figures for motocross. A single simple linear regression analysis was used to assess the relationship between time and participation in the 7 extreme sports over the 12-year span. Student t tests were used to compare injury rates between sports. All statistical analyses were performed using R statistical software version 3.0.1, with α = 0.05.
Results
A total of 4,083,691 injuries were reported for all 7 extreme sports between 2000 and 2011, of which 460,115 (11.3%) were HNIs. Of the total reported HNIs, 381,760 (83%) were head injuries and 78,355 (17%) were neck injuries. The average number of HNIs was 38,385 per year. Regression analysis demonstrated a significant increase (P = .001) in the occurrence of HNIs over the studied time period (Figure 1). Although the incidence of injuries in extreme sports HNIs increased from the year 2000 (34,565) to 2011 (40,042), this trend was not consistent from year to year. Additionally, there was no significant increase in the total number of participants from year to year (P = .08). Furthermore, when combined, there was no significant difference (P = .67) in the occurrence of HNIs between the 3 winter and 4 summer extreme sports during the 12 years (Table 1).
Figure 1.
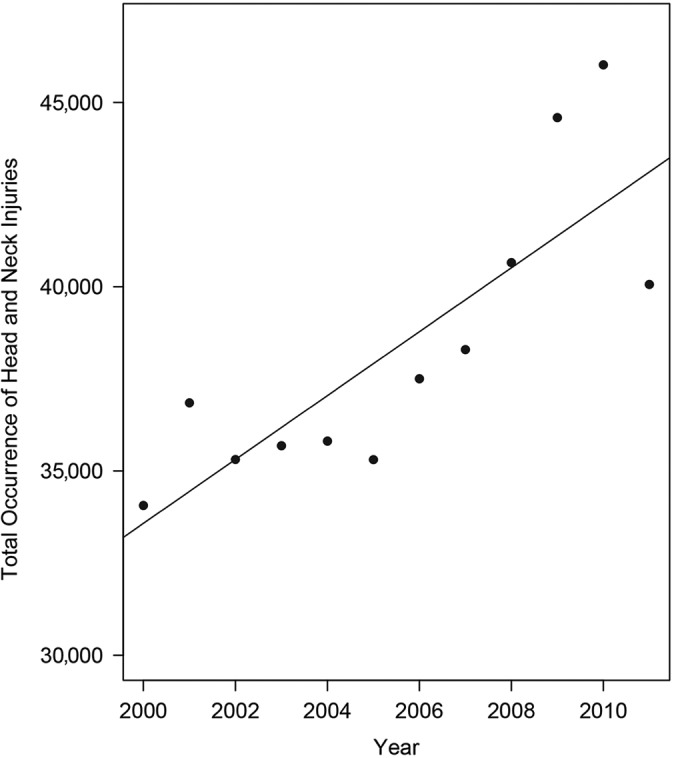
Head and neck injuries in 7 extreme sports between 2000 and 2011.
TABLE 1.
Common Head and Neck Injuries in Extreme Sports (2000-2011)
| Summer Sports, n (%) | ||||
|---|---|---|---|---|
| Surfing | Mountain Biking | Motocross | Skateboarding | |
| Head injuries | ||||
| Concussion | 3242 (8.2) | 4530 (29.7) | 22,788 (29.1) | 28,328 (21.9) |
| Contusion/abrasion | 2097 (5.3) | 1080 (7.1) | 5164 (6.6) | 14,703 (11.3) |
| Fracture | 173 (0.4) | 115 (0.8) | 961 (1.2) | 3544 (2.7) |
| Laceration | 14,990 (37.7) | 1182 (7.8) | 3211 (4.1) | 17,189 (13.3) |
| Total | 20,502 (51.6) | 6907 (45.3) | 32,124 (41.1) | 63,764 (49.2) |
| Neck injuries | ||||
| Contusion/abrasion | 344 (0.9) | 221 (1.5) | 1321 (1.7) | 442 (0.3) |
| Fracture | 1209 (3.0) | 527 (3.5) | 1452 (1.9) | 42 (0.0) |
| Laceration | 187 (0.5) | 69 (0.5) | 825 (1.1) | 151 (0.1) |
| Strain/sprain | 10,112 (25.4) | 2059 (13.5) | 10,626 (13.6) | 6637 (5.1) |
| Total | 11,852 (29.8) | 2876 (18.9) | 14,224 (18.2) | 7272 (5.6) |
| Other head and neck injuries | 7404 (18.6) | 5450 (35.8) | 31,888 (40.8) | 58,564 (45.2) |
| Total, summer sports | 39,758 (100) | 15,233 (100) | 78,236 (100) | 129,600 (100) |
| Winter Sports, n (%) | ||||
| Snowboarding | Snowmobiling | Snow Skiing | ||
| Head injuries | ||||
| Concussion | 42,811 (43.9) | 4054 (24.6) | 34,897 (41.9) | |
| Contusion/abrasion | 6963 (7.1) | 1290 (7.8) | 4488 (5.4) | |
| Fracture | 403 (0.4) | 162 (1.0) | 625 (0.8) | |
| Laceration | 6514 (6.7) | 992 (6.0) | 5507 (6.6) | |
| Total | 56,691 (58.1) | 6498 (39.5) | 45,517 (54.6) | |
| Neck injuries | ||||
| Contusion/abrasion | 375 (0.4) | 581 (3.5) | 230 (0.3) | |
| Fracture | 784 (0.8) | 206 (1.3) | 1039 (1.2) | |
| Laceration | 88 (0.1) | 349 (2.1) | 181 (0.2) | |
| Strain/sprain | 13,645 (14.0) | 3886 (23.6) | 14,009 (16.8) | |
| Total | 14,892 (15.3) | 5022 (30.5) | 15,459 (18.6) | |
| Other head and neck injuries | 25,944 (26.6) | 4928 (30.0) | 22,337 (26.8) | |
| Total, winter sports | 97,527 (100) | 16,448 (100) | 83,313 (100) | |
There was a wide range of injury rates for HNI between individual extreme sports (Figure 2). The 4 sports with the highest total number of reported HNIs during the 12-year period were skateboarding (129,600), snowboarding (97,527), skiing (83,313), and motocross (78,236) (Table 1). The sports with the lowest reported number of HNIs were mountain biking (15,233), snowmobiling (16,448), and surfing (39,758). There were 140,650 concussions (31% of HNIs, 3.4% of all injuries) reported over the 12-year period for extreme sports. Snowboarding had the most concussions (42,811), accounting for 30% of all reported concussions, while snow skiing had the second most occurrences (34,897), accounting for 25% of all reported concussions (Figure 3). Snowmobiling and surfing had the fewest reported concussions (2.9% [4054] and 2.3% [3242], respectively).
Figure 2.
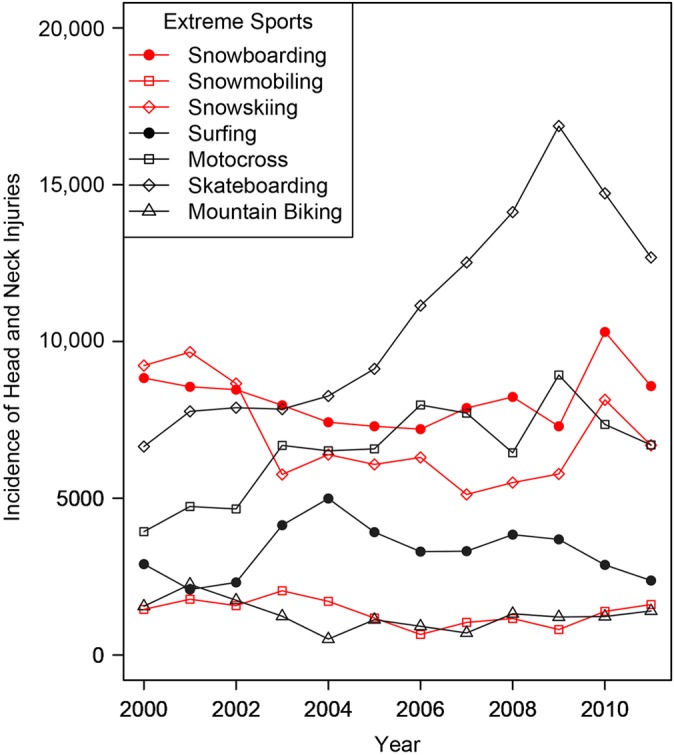
Distribution of injuries in individual extreme sports from 2000 to 2011.
Figure 3.

Distribution of severe injuries and concussions in individual extreme sports. (A) Occurrence of concussions and (B) occurrence of severe injuries.
Severe HNI (classified as either a cervical or skull fracture) had a total occurrence of 11,242, which accounted for 2.4% of HNIs. Skateboarding and motocross had the greatest number of severe HNIs (3586 and 2413, respectively) (Figure 3). Furthermore, skateboarding had the highest reported number of skull fractures (3544), accounting for 59.2% of all reported skull fractures for extreme sports, and motocross had the highest incidence of neck fractures (1452), which accounted for 27.6% of all reported neck fractures.
The risk of an extreme sport participant suffering an HNI over a 1-year period was 5.16 per 10,000 person-years (motocross was excluded from risk analysis). The average injury incidence rates for the summer and winter extreme sports were 6.10 per 10,000 person-years and 4.23 per 10,000 person-years, respectively, with a calculated incidence rate ratio (IRR) of 1.44 for the summer sports, with the winter sports as the referent group. Skateboarding had the highest risk of HNI for extreme sports participants (10.21 per 10,000 person-years), while mountain bicycling had the lowest risk (1.08 per 10,000 person-years) (Table 2). The HNI incidence rates for snowboarding were much higher than snow skiing (8.6 and 2.45 per 10,000 person-years, respectively), with a calculated IRR of 3.5 for snowboarding compared with snow skiing as the referent group (Table 2).
TABLE 2.
Risk of Head and Neck Injuries in Extreme Sports
| Sport | Incidence Rate per 10,000 Person-Years | Incidence Rate Ratio |
|---|---|---|
| Mountain biking | 1.08 | 1 |
| Snowmobiling | 1.64 | 1.51 |
| Snow skiing | 2.46 | 2.28 |
| Surfing | 7.00 | 6.49 |
| Snowboarding | 8.60 | 7.97 |
| Skateboarding | 10.21 | 9.46 |
Snowboarding had the greatest calculated incidence of concussions (535.7 per 1,000,000 person-years), followed by skateboarding (414.9 per 1,000,000 person-years) (Table 3). Furthermore, a snowboarder was 3.5 times more likely to suffer a concussion compared with a snow skier (152.5 per 1,000,000 person-years). There was a 54 times greater calculated risk of a skull fracture for skateboarding (54.7 per 1,000,000 person-years) compared with snowboarding (0.98 per 1,000,000 person-years) (Table 4). Similarly, there was a 38 times greater risk of suffering a neck fracture while surfing (38.09 per 1,000,000 person-years) compared with skateboarding (1.00 per 1,000,000 person-years) (Table 4). Mountain biking was the second riskiest sport with respect to neck fractures, with an incidence rate of 12.8 per 1,000,000 person-years.
TABLE 3.
Incidence Rate of Concussions in Extreme Sports
| Sport | Incidence Rate per 1,000,000 Person-Years | Incidence Rate Ratio |
|---|---|---|
| Mountain biking | 50 | 1 |
| Snowmobiling | 60 | 1.2 |
| Surfing | 103 | 2.06 |
| Snow skiing | 152 | 3.04 |
| Skateboarding | 415 | 8.3 |
| Snowboarding | 534 | 10.68 |
TABLE 4.
Incidence Rate of Skull and Neck Fractures in Extreme Sports
| Incidence Rate per 1,000,000 Person-Years | Incidence Rate Ratio | |
|---|---|---|
| Skull fractures by sport | ||
| Snowboarding | 1 | 1 |
| Mountain biking | 2 | 2 |
| Snow skiing | 2 | 2 |
| Snowmobiling | 4 | 4 |
| Surfing | 9 | 9 |
| Skateboarding | 55 | 55 |
| Neck fractures by sport | ||
| Skateboarding | 1 | 1 |
| Snow skiing | 5 | 5 |
| Snowmobiling | 6 | 6 |
| Snowboarding | 7 | 7 |
| Mountain biking | 13 | 13 |
| Surfing | 38 | 38 |
Discussion
This study presents previously unknown data and establishes incidence rates of HNIs in extreme sports. Between 2000 and 2011, over 4,000,000 injuries occurred in extreme sports, of which 11.3% were HNIs. Although the risk of HNI while participating in extreme sports was low, there was a significant increase in the number of HNIs from 2000 to 2011. Furthermore, as participation grows in these nontraditional sports, physicians need to be aware of the distribution of injuries specific to extreme sports to implement optimal treatment and prevention programs.
Concussions were the most common HNI among extreme sports participants (Table 1). The risk of suffering a concussion was highest in snowboarding and skateboarding. Recently, there has been a lot of media attention placed on the long-term sequelae of concussions suffered in mainstream sports. It is well known that permanent neurological deficits are related to severe and recurrent concussions.12 Most professional and collegiate sports and many high school organizations have adopted time-effective concussion policies12 and implemented use of tools like the SCAT 2 on the sidelines. One of the medical challenges with extreme sports is patient accessibility. Many extreme sports take place in environments where medical care may not be readily available on site, with the exception of participation in professional competitions. Because of these challenges, greater emphasis needs to be placed on proper helmet and safety strategies to prevent participant concussions.
In addition to concussions, severe injuries are another concern in extreme sports. Skateboarders were found to have the highest risk of skull fractures compared with the 5 other extreme sports. Surfers had the highest risk of neck fracture, with a surprising 38 times increased risk compared with skateboarders. While the incidence of severe injuries was low for the studied extreme sports, skull and neck fractures can have devastating effects on quality of life. Physicians need to be aware of these trends in activities with high rates of severe injuries, such as skateboarding, so that they can provide proper patient advice, prevention care, and safety equipment. Additionally, our study found that 12% of motocross injuries were HNIs, similar to previously published studies (14%).11
Head and neck injuries pose serious economic and social threats. The overall cost associated with an HNI in extreme sports has been described in 3 phases.20 The first phase is the cost of the evacuation (transport, acute medical care, etc), the second phase is the cost of rehabilitation (therapy, treatment, etc), and the third phase is the cost to the community (social support, future medical care, etc). The cumulative cost of all 3 phases for HNI for an individual patient can range from $30,000 to $2 million, depending on the severity of the injury.4 Furthermore, the consequences of HNI are not restricted to economics; they can also negatively alter quality of life and interpersonal relationships. Severe concussion or repeat concussion can lead to chronic traumatic encephalopathy, a syndrome that results in a high rate of depression, drug dependence, and possibly, suicide attempt or completion.1 Studies have shown that HNIs have resulted in deteriorated marital relationships, decreased income, and a feeling of loneliness resulting from a lack of social interaction.10,21
Limitations were present in this study. The NEISS database obtains information from only emergency room visits, thus excluding patients who go untreated or are treated in outpatient settings. Furthermore, NEISS data are restricted to the product-code system. The combination of these 2 factors limits how accurately we can predict rates and trends in the general population. Additionally, the population of the study includes both recreational and competitive sports participation; therefore, it may not accurately reflect the risk of individuals participating in an extreme sport. A study using a database that tracks injuries in organized extreme sports competitions (eg, X Games) would be a useful area of future focus.
Conclusion
This study helps educate participants and physicians about the types of HNIs associated with the growing arena of extreme sports. This study offers important data regarding the trends of HNI in extreme sports. HNIs can greatly alter a person’s quality of life, and as participation in these sports increases, understanding the incidence of HNI will assist in implementing effective medical prevention programs and proper safety equipment practices. More research regarding the long-term outcomes of HNI in extreme sports needs to be done to provide sports medicine physicians with a comprehensive clinical picture of these devastating injuries.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
References
- 1. (CPSC) USCPSC. The NEISS—The National Electronic Injury Surveillance System: a tool for researchers. US Consumer Product Safety Commission; http://www.cpsc.gov/en/Research--Statistics/NEISS-Injury-Data/. Accessed February 13, 2013. [Google Scholar]
- 2. Ackery A, Hagel BE, Provvidenza C, Tator CH. An international review of head and spinal cord injuries in alpine skiing and snowboarding. Inj Prev. 2007;13:368–375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Balthrop PM, Nyland J, Roberts CS. Risk factors and musculoskeletal injuries associated with all-terrain vehicle accidents. J Emerg Med. 2009;36:121–131. [DOI] [PubMed] [Google Scholar]
- 4. Bergeron MF, Engebretsen L. Protecting elite athletes in extreme and challenging environments: advancing the dialogue. Br J Sports Med. 2012;46:769. [DOI] [PubMed] [Google Scholar]
- 5. Brymer E, Schweitzer R. Extreme sports are good for your health: a phenomenological understanding of fear and anxiety in extreme sport. J Health Psychol. 2013;18:477–487. [DOI] [PubMed] [Google Scholar]
- 6. Caine DJ. The epidemiology of injury in adventure and extreme sports. Med Sport Sci. 2012;58:1–16. [DOI] [PubMed] [Google Scholar]
- 7. de Jong P. The health impact of mandatory bicycle helmet laws. Risk Anal. 2012;32:782–790. [DOI] [PubMed] [Google Scholar]
- 8. Goulet C, Hagel BE, Hamel D, Légaré G. Self-reported skill level and injury severity in skiers and snowboarders. J Sci Med Sport. 2010;13:39–41. [DOI] [PubMed] [Google Scholar]
- 9. Graves JM, Whitehill JM, Stream JO, Vavilala MS, Rivara FP. Emergency department reported head injuries from skiing and snowboarding among children and adolescents, 1996-2010. Inj Prev. 2013;19:399–404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Jennum P, Kjellberg J, Ibsen R, Bendix T. Health, social, and economic consequences of neck injuries: a controlled national study evaluating societal effects on patients and their partners. Spine (Phila Pa 1976). 2013;38:449–457. [DOI] [PubMed] [Google Scholar]
- 11. Larson AN, Stans AA, Shaughnessy WJ, Dekutoski MB, Quinn MJ, McIntosh AL. Motocross morbidity: economic cost and injury distribution in children. J Pediatr Orthop. 2009;29:847–850. [DOI] [PubMed] [Google Scholar]
- 12. Ma R, Miller CD, Hogan MV, Diduch BK, Carson EW, Miller MD. Sports-related concussion: assessment and management. J Bone Joint Surg Am. 2012;94:1618–1627. [DOI] [PubMed] [Google Scholar]
- 13. Ogawa H, Sumi H, Sumi Y, Shimizu K. Skill level-specific differences in snowboarding-related injuries. Am J Sports Med. 2010;38:532–537. [DOI] [PubMed] [Google Scholar]
- 14. Osberg JS, Schneps SE, Di Scala C, Li G. Skateboarding: more dangerous than roller skating or in-line skating. Arch Pediatr Adolesc Med. 1998;152:985–991. [DOI] [PubMed] [Google Scholar]
- 15. The Outdoor Foundation. 2013. Outdoor Recreation Participation Report. http://www.outdoorfoundation.org/research.participation.2013.html. Accessed February 13, 2013.
- 16. Pikora TJ, Braham R, Mills C. The epidemiology of injury among surfers, kite surfers and personal watercraft riders: wind and waves. Med Sport Sci. 2012;58:80–97. [DOI] [PubMed] [Google Scholar]
- 17. Rice MR, Alvanos L, Kenney B. Snowmobile injuries and deaths in children: a review of national injury data and state legislation. Pediatrics. 2000;105:615–619. [DOI] [PubMed] [Google Scholar]
- 18. Schroeder T, Ault K. The NEISS sample design and implementation. http://www.cpsc.gov//PageFiles/106617/2001d011-6b6.pdf. Accessed September 29, 2013.
- 19. Sulheim S, Holme I, Ekeland A, Bahr R. Helmet use and risk of head injuries in alpine skiers and snowboarders. JAMA. 2006;295:919–924. [DOI] [PubMed] [Google Scholar]
- 20. Tator CH, Duncan EG, Edmonds VE, Lapczak LI, Andrews DF. Complications and costs of management of acute spinal cord injury. Paraplegia. 1993;31:700–714. [DOI] [PubMed] [Google Scholar]
- 21. Wedcliffe T, Ross E. The psychological effects of traumatic brain injury on the quality of life of a group of spouses/partners. S Afr J Commun Disord. 2001;48:77–99. [PubMed] [Google Scholar]
- 22. Willig C. A phenomenological investigation of the experience of taking part in ‘extreme sports’. J Health Psychol. 2008;13:690–702. [DOI] [PubMed] [Google Scholar]