

Abstract
Background:
Previous studies investigating the windmill softball pitch have focused primarily on shoulder musculature and function, collecting limited data on elbow and forearm musculature. Little information is available in the literature regarding the forearm. This study documents forearm muscle electromyographic (EMG) activity that has not been previously published.
Purpose:
Elbow and upper extremity overuse injuries are on the rise in fast-pitch softball pitchers. This study attempts to describe forearm muscle activity in softball pitchers during the windmill softball pitch. Overuse injuries can be prevented if a better understanding of mechanics is defined.
Study Design:
Descriptive laboratory study.
Methods:
Surface EMG and high-speed videography was used to study forearm muscle activation patterns during the windmill softball pitch on 10 female collegiate-level pitchers. Maximum voluntary isometric contraction of each muscle was used as a normalizing value. Each subject was tested during a single laboratory session per pitcher. Data included peak muscle activation, average muscle activation, and time to peak activation for 6 pitch types: fastball, changeup, riseball, curveball, screwball, and dropball.
Results:
During the first 4 phases, muscle activity (seen as signal strength on the EMG recordings) was limited and static in nature. The greatest activation occurred in phases 5 and 6, with increased signal strength, evidence of stretch-shortening cycle, and different muscle characteristics with each pitch style. These 2 phases of the windmill pitch are where the arm is placed in the 6 o’clock position and then at release of the ball. The flexor carpi ulnaris signal strength was significantly greater than the other forearm flexors. Timing of phases 1 through 5 was successively shorter for each pitch. There was a secondary pattern of activation in the flexor carpi ulnaris in phase 4 for all pitches except the fastball and riseball.
Conclusion:
During the 6 pitches, the greatest muscular activity was in phases 5 and 6. Flexor carpi ulnaris activity was greatest among the muscles tested. The riseball had the highest peak activity, but the curveball and dropball had the highest average signal strength. This muscle activity correlates with increasing distraction in the elbow, suggesting that flexor muscles act to counterdistract the elbow as they do for the baseball pitch.
Clinical Relevance:
Windmill pitchers are unique among overhead athletes as they throw, on average, more pitches per overhead athlete. Understanding the mechanics and physiology of the elbow in windmill pitchers is crucial to prevention and treatment of these increasingly common elbow injuries. This study establishes baseline data that will be useful to further prevent windmill pitch elbow injury.
Keywords: windmill, fastpitch, softball, forearm musculature, women
The mechanics and function of the windmill pitch in collegiate women’s fast-pitch softball has been studied in some detail. However, the majority of studies have focused on shoulder musculature and function—specifically the deltoid muscle, rotator cuff musculature, the pectoralis major, the serratus anterior, the biceps brachii muscle, the latissimus dorsi, and the triceps muscle.2,4 While these studies have provided insight into the shoulder musculature during windmill pitching, there have not been any studies evaluating the musculature of the forearm.2,5,6 Argo et al1 published a series of elbow injuries and surgeries in female athletes. Their study included softball players, one of which was a pitcher who had ulnar collateral and medial elbow injuries. An injury survey by Hill et al5 found that younger, or more novice, female collegiate pitchers relied on the upper arm and forearm muscles to increase their pitch velocity. Meyers et al8 found that there were large forces carried by the elbow during the windmill pitch, but did not focus on the musculature of the forearm. Tanabe et al13 described 3 cases of ulnar stress fractures in windmill softball pitchers illustrating the potential for injury due to the biomechanical forces generated by the windmill pitch.
This study was designed to investigate forearm muscle activity during the windmill softball pitch. Some have the belief that the underhand motion of the softball pitch places little stress on the arm, and pitching-related injuries are rare in softball.6 It has been shown that over a 3-day tournament, the best pitcher on the team can throw as many as 1200 to 1500 pitches compared with an average of 100 to 150 pitches for a baseball pitcher over that same period of time.15 Unlike baseball, the Amateur Softball Association has no rules limiting the number of pitches thrown at any level of play.16
Werner et al,16 in their study of the kinematics of the windmill pitch, provided an understanding of large distraction forces at the elbow during the windmill pitch, in which they used regression analysis. However, their study did not use any electromyographic (EMG) data to calculate the signal intensity of the muscles in the forearm. Maffet et al7 were the first to define the 6 phases of the pitching motion (Figure 1). They showed that varying positions of the arm generate significant muscular forces that act on the shoulder. There are many studies that define the shoulder muscle firing patterns in the windmill softball pitch, as well as overhand throwing. We believe our study is the first to define the EMG muscle activity level of the forearm, other than the biceps, during the windmill softball pitch.
Figure 1.

High-speed videography depiction of the individual phases during the windmill softball pitch.
Materials and Methods
Two separate institutional review board approvals were obtained for this study, one from each participating institution. We also verified that there was no violation of National Collegiate Athletic Association (NCAA) rules for participating in the research and that eligibility would not be affected by a travel expense stipend.
Ten female collegiate-level pitchers from 3 different colleges participated in this study. Separate written consents were obtained for study participation and for dissemination of audiovisual images. Pre- and postparticipation questionnaires were completed for basic demographic information and to exclude anyone with pitching-related injuries within the past year.
Participants had bipolar surface EMG sensors placed over the muscle belly of each of the specific muscles being investigated, slightly distal to the midpoint of the muscle, as described by Cram et al3 and Perotto et al11 (Figure 2).
Figure 2.
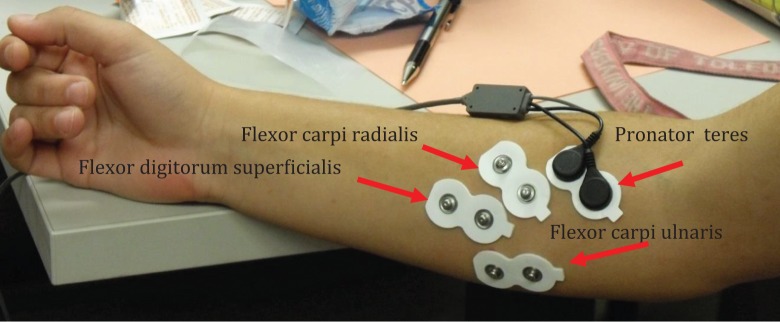
Placement of bipolar surface electrodes over the muscle bellies of the muscles of interest.
A reference electrode was attached over the olecranon process. EMG data were collected using a Telemyo 2400 EMG system (Norazon) operating at a sampling rate of 2000 Hz. To capture the motion via high-speed video, each pitcher had reflective markers placed at 24 predefined anatomic locations (Figure 3). A 12-camera Eagle motion capture system (Motion Analysis Inc) operating at a rate of 200 Hz was used to record the pitcher’s movements. This system tracked 24 reflective video markers placed on the upper extremity, trunk, and lower extremity body segments. A standard video camcorder was used to capture overall activity.
Figure 3.

Placement of reflective markers for high-speed camera sensors.
Ground reaction force data from the pitchers lead foot were recorded at 2000 Hz through an AMTI force platform (Advanced Mechanical Technology).
Recording, time matching, and processing of all data were done through a personal computer running version 2.5.1 of the Cortex Motion Analysis software (Motion Analysis Inc).
The maximum voluntary isometric contraction (MVIC) of each muscle was determined as described previously.12 This was measured by placing the pitching arm with the elbow in 90° of flexion and the hand underneath a stationary countertop (Figure 4). We performed 3 timed series of measurements. These trials were averaged to give a single MVIC value for each of the 4 muscles being tested, which was then used to determine the overall percentage of muscle activity during each pitch.
Figure 4.

Placement of the hand for the calculation of maximum voluntary isometric contraction (MVIC).
Procedure
After arriving at the laboratory and completing the approved institutional review board informed consent forms, the subjects were given as much time as necessary to warm up using their normal pregame or prepractice warm-up procedure.
Each subject was prepped for electrode placement by cleaning and slightly abrading the skin surface at the electrode sites. Electrodes were attached with their self-adhesive backing and then secured in place to the athlete’s arm by overwrapping the electrodes with flexible athletic tape. The wires from the electrodes were then connected to a wireless transmitter that was worn at the subject’s waist. The reflective video markers were attached to the designated positions with double-sided tape, and these were secured in place with flexible athletic tape.
Before the pitching trials started, each pitcher was allowed to throw several trial pitches at full speed to become comfortable with the electrodes and high-speed sensors and to reinforce any sensors that loosened or became detached with the pitcher’s full effort.
All pitches were thrown from a designated starting position in the middle of the video capture field of vision, at a target area on a net in front of the pitcher, approximately 20 feet from the simulated mound. Subjects had an unlimited amount of time to complete their pitches, and threw a total of 30 pitches: 5 trials of each of the 6 designated pitch types (fastball, curveball, changeup, riseball, dropball, and screwball). Each pitch was used to calculate the average EMG signal for that pitch style. The order of the pitch types was consistent across all subjects.
Once the pitching trials were completed, the subject completed 3 trials each of 3 different MVIC exercises, intended to elicit an MVIC for each of the muscles being tested. These MVIC trials involved a 5-second isometric contraction at the approximate midpoint of the subject’s total range of motion for that movement. The EMG data from the MVIC trials were processed in the same manner as those of the throwing trials. The MVIC was selected as a normalizing value (100%).
Data Processing and Statistical Analysis
All motion capture video data were smoothened using a Butterworth low-pass filter with a cutoff at 20 Hz before being used to identify the 7 segment positions that defined the 6 phases of the throwing motion. The times of these 7 positions were then used to identify the corresponding phases within the EMG data. Prior to analysis, the raw EMG data were band-pass filtered with cutoffs of 10 Hz and 500 Hz, after which it was full-wave rectified.
For every pitch and for each of the phases within the throws, the average EMG values were determined for each muscle. These data were then normalized using the MVIC values for the muscle; thus, the EMG measurement units are %MVIC. All data were then averaged across each subject’s trials, and these values averaged across the 10 subjects. Thus, the results reflect group means for each phase of each of the 6 types of pitches.
Once the EMG data were recorded, the signal strengths were used to generate a ratio with the MVIC previously described. The signals from each of the 6 pitches from the selected pitch style (fastball, changeup, curveball, etc) were first averaged and then the %MVIC was calculated.
Demographic Characteristics of Research Volunteers
Demographic characteristics are presented in Table 1. None of the subjects reported a current injury, softball-related surgeries, or joint injections. No subject reported a history of shoulder injuries, but 2 (20%) reported previous elbow injuries. Sixty percent reported the use of pitch counts during games to track the number of pitches thrown in a single game. Pitch counts are frequently used to determine when to bring in a relief pitcher to avoid risking a fatigue-related injury. None of the subjects reported pain before or after the testing period.
TABLE 1.
Study Demographics (N = 10 Participants)
| Age, y, mean (range) | 18.5 (18-19) |
| Height, in, mean (range) | 68 (66-69) |
| Weight, lb, mean (range) | 160 (140-175) |
| Pitching hand, n (%) | |
| Right | 9 (90) |
| Left | 1 (10) |
| Academic level, n (%) | |
| Freshman | 5 (50) |
| Sophomore | 3 (30) |
| Junior | 1 (10) |
| Senior | 1 (10) |
| White, n (%) | 10 (100) |
| Played softball in grade school, n (%) | 10 (100) |
| Years pitching, mean (range) | 7 (6-8) |
| Played softball in high school, n (%) | 10 (100) |
| Years pitching, mean (range) | 4 (4-4) |
| Played softball in college, n (%) | 10 (100) |
| Years pitching, mean (range) | 1.5 (1-2) |
| Had private lessons | 8 (80) |
| Years with private lessons | 5.5 (3-8) |
| Subject effort during testing period (1 = low, 10 = high), n (%) | |
| 7 | 1 (10) |
| 8 | 1 (10) |
| 9 | 2 (20) |
| 10 | 6 (60) |
Subjects were asked to rate their level of effort while pitching during the data collection testing period (not the warm-up or cool-down period) compared with the same intensity they would use pitching in a real game. Minimal effort was scored as a 1 and maximum intensity was a 10 (Table 1).
Results
Muscle activity in the forearm showed a consistent increase across the successive phases (Figures 5 –10). The lowest average activity was seen in phase 3, with an average signal strength below 50% of the MVIC. The signal strength markedly increased during phases 4 through 6. Flexor carpi ulnaris (FCU) contraction reached an average of nearly 500% of MVIC during phase 6 of the riseball pitch. Pronator teres, flexor carpi radialis, and flexor digitorum superficialis also increased but with a variable pattern based on pitch type. Each of these muscles did have an increase in average peak activity to at least 150% of MVIC. The breaking pitches (dropball, curveball, screwball) had a more rapid increase in FCU activation during phase 4 that plateaued in phase 5 and then a second rapid rise in peak activity through phase 6. The riseball and fastball pitches showed a more consistent rise through phases 4 and 5, with a rapid increase through phase 6. The changeup pitch did show a decrease in pronator teres activity between phases 5 and 6.
Figure 5.
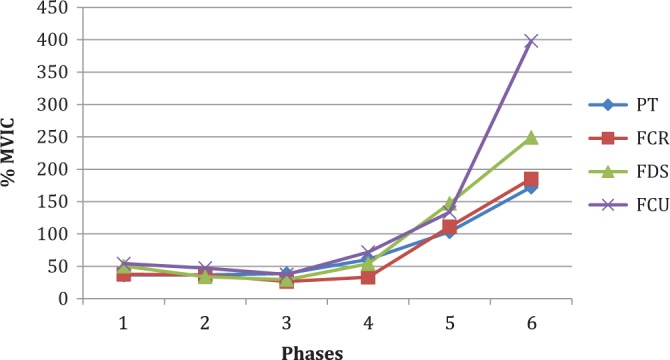
Surface electromyography chart of the fastball pitch. MVIC, maximum voluntary isometric contraction; PT, pronator teres; FCR, flexor carpi radialis; FDS, flexor digitorum superficialis; FCU, flexor carpi ulnaris.
Figure 6.

Surface electromyography chart of the changeup pitch. MVIC, maximum voluntary isometric contraction; PT, pronator teres; FCR, flexor carpi radialis; FDS, flexor digitorum superficialis; FCU, flexor carpi ulnaris.
Figure 7.

Surface electromyography chart of the curveball pitch. MVIC, maximum voluntary isometric contraction; PT, pronator teres; FCR, flexor carpi radialis; FDS, flexor digitorum superficialis; FCU, flexor carpi ulnaris.
Figure 8.
Surface electromyography chart of the screwball pitch. MVIC, maximum voluntary isometric contraction; PT, pronator teres; FCR, flexor carpi radialis; FDS, flexor digitorum superficialis; FCU, flexor carpi ulnaris.
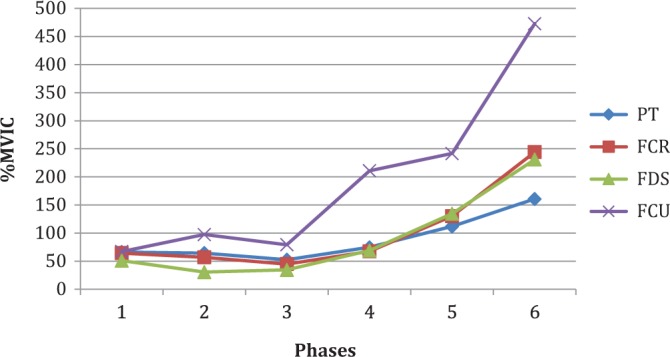
Figure 9.

Surface electromyography chart of the riseball pitch. MVIC, maximum voluntary isometric contraction; PT, pronator teres; FCR, flexor carpi radialis; FDS, flexor digitorum superficialis; FCU, flexor carpi ulnaris.
Figure 10.

Surface electromyography chart of the dropball pitch. MVIC, maximum voluntary isometric contraction; PT, pronator teres; FCR, flexor carpi radialis; FDS, flexor digitorum superficialis; FCU, flexor carpi ulnaris.
The pronator teres had the lowest average peak signal strength of all the muscles tested, reaching a peak of approximately 172% MVIC. Flexor digitorum superficialis and flexor carpi radialis had similar activation patterns across all phases of each pitch. The flexor digitorum superficialis reached an average peak of 248% MVIC in the fastball pitch. The flexor carpi radialis reached an average peak signal strength of 284% MVIC with the dropball pitch.
When the signal strengths were averaged for each individual muscle across all pitchers, the curveball and screwball had higher FCU signal strengths compared with the riseball. When looking at just the peak muscle activity, however, the riseball shows the highest FCU peak activity.
The duration of the phases was calculated by time matching the defined phases of the windmill pitch from the high-speed videography with the timing sequence of the EMG signals. The time duration of phases 1 through 5 showed a gradual decrease in all pitches (Table 2). The duration of phase 1 in the curveball was markedly longer, reaching almost 50% longer duration of the time in phase 1 of the other pitches. Phase 6 was of the longest duration, while, in contrast, phase 5 was the shortest (Figures 11 and 12). In our study, we included a short 1- to 2-ms extension of phase 6 timed to just after ball release to include the extended duration of maximum muscle contraction.
TABLE 2.
Comparison of Phase Duration
| Pitch | Phase Duration, ms | |||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | |
| Riseball | 17.56 | 15.63 | 12.85 | 11.03 | 8.96 | 33.97 |
| Screwball | 17.2 | 15.38 | 12.43 | 11.67 | 9.42 | 33.9 |
| Curveball | 25.94 | 13.92 | 11.66 | 10.42 | 7.57 | 30.49 |
| Dropball | 16.42 | 15.92 | 12.72 | 11.86 | 9.49 | 33.6 |
| Fastball | 16.85 | 16.19 | 12.61 | 11.16 | 8.59 | 34.59 |
| Changeup | 15.94 | 14.92 | 12.42 | 12.36 | 10.34 | 34.04 |
Figure 11.

Phase duration of pitches (in milliseconds).
Figure 12.

Average of %MVIC (percentage maximum voluntary isometric contraction) across all pitchers. FCR, flexor carpi radialis; FCU, flexor carpi ulnaris; FDS, flexor digitorum superficialis; PT, pronator teres.
Discussion
The data reveal a large and rapid rise in the activity of the forearm muscles during the windmill softball pitch. In the early phases, we see a rather quiescent and low-level activity of the EMG signals. The strength of the EMG signal seen in the FCU, with the progression from phase 3 to 4 through phase 6, allows us to understand what is occurring in the forearm. We know the muscles will help position the wrist at release, but what the strength of the EMG signal leads us to understand is the secondary function of the forearm flexors.
We notice that all the forearm muscles we tested have a characteristic rise across all phases of the windmill pitch. The signals show variance in how the muscles are functioning in wrist and hand position as well as stabilization of the elbow. Among all muscles tested, the FCU is consistently shown to have the highest EMG signal strength (Table 3). It has been shown in cadaveric studies that the FCU is a secondary stabilizer of the medial elbow under valgus loading.10,14 Our study data confirm that idea by showing the FCU has the highest EMG activity in the latter phases when the distraction forces at the elbow are greatest. The FCU is anatomically aligned with the longitudinal axis of the forearm and runs superficial and parallel to the anterior band of the ulnar collateral ligament. This places the FCU in alignment to counter the distraction forces that are created at the elbow joint with the windmill pitching motion.
TABLE 3.
Peak FCU Comparison (%MVIC)a
| Pitch | FCU Peak |
|---|---|
| Riseball | 494.87 |
| Screwball | 472.79 |
| Curveball | 467.61 |
| Dropball | 399.34 |
| Fastball | 398.45 |
| Changeup | 282.85 |
aFCU, flexor carpi ulnaris; MVIC, maximum voluntary isometric contraction.
Looking at Figures 5 through 10, these show specific differences in the pattern of how the muscles are firing. The riseball (see Figure 9) had the highest peak of EMG activity at just below 500% MVIC. The screwball and curveball (Figures 7 and 8, respectively) both had EMG activity higher than the fastball, reaching a peak just above 450% MVIC. These so-called breaking pitches appear to result in higher stress across the elbow, which would place that joint at risk for fatigue injury.
Noting that when the signal strengths are averaged for all pitchers in the study, it reveals that across all phases, the curveball and dropball have the highest signal strength. In comparison, the peak FCU signal strength in isolation is highest for the riseball. This would lead us to believe that as an individual pitch, the riseball has the greatest peak strength, but when all the pitches are averaged for all pitchers, the curveball and dropball begin to generate the greatest peak signal strength.
The changeup (see Figure 6) had the lowest signal of all pitches. This is likely due to the static position of the hand and wrist through the final phase of the windmill pitch motion. The shoulder is maintaining a constant speed to give the appearance of a high-speed pitch, but at release, the hand and wrist have very little motion, which does not impart a large amount of speed to the ball. These low-signal strengths would also lead us to believe that there is less distraction occurring at the elbow with the changeup pitch due to less rotational velocity of the entire upper extremity. Also noted was the relatively low pronator teres signal across all pitches, which is likely due to the internal rotation of the shoulder imparting more rotational velocity with the elbow extended than the pronator teres acting to pronate the forearm.
As you look across the graphs analyzing the other muscles, they too have a characteristic rise in their %MVIC from as early as phase 4 through phase 6. We believe not only are they contributing to hand and wrist position for ball control, they also cross the joint and contribute to stabilization of the elbow, but to a somewhat lesser degree.
The historical ideas behind the underhand pitching motion led early participants to believe that this motion caused little to no damage to the arm, in comparison with what overhead athletes experienced during their pitching motions. However, as early as 1992, Loosli et al6 published an article on injuries to elite pitchers in fast-pitch softball. They surveyed all pitchers from the teams participating in the 1989 NCAA College World Series. They detected injuries that resulted in either no time loss from play, altered playtime, or lost time from play. Of a total 24 pitchers surveyed, there was a total of 26 injuries or complaints, with almost a third of these being upper extremity injuries (31%) occurring at or distal to the level of the elbow.6 Hill et al5 also showed in their survey of collegiate level pitchers that there were several injuries to the upper extremity. Meyers et al8 reported in their review article that nearly 32% of injuries reported in softball pitchers are related to the upper arm, elbow, and wrist. Oliver et al9 performed a kinematic study comparing motion analysis between advanced, intermediate, and novice pitchers. The purpose of their study was to describe what variability the kinetic chain had among the 3 groups. They showed the upper extremity is a large portion of the kinetic chain, but less experienced pitchers relied on their upper extremity for more kinetic input than the other more experienced groups. This may lead us to believe that pitching mechanics education is as important in youth softball as it has been in youth baseball. Rojas et al12 performed a surface EMG study of the biceps muscle during the windmill pitch and compared it to the activity of the biceps in overhand pitching. They reported that the muscle activity is higher in the windmill pitch, likely related to the counterbalance of the distraction forces generated. These studies underscored our suspicions that the underhand pitching style is not as benign as has been previously suggested, and our study supports the risk of overuse injuries due to mechanical stresses imposed on the forearm musculature.
Limitations
In this study, we used adhesive surface electrodes instead of invasive fine wire electrodes for the signal collection of the muscle activity. Needle electrodes would have given a more accurate reading of the muscle activity during the pitching motion and eliminated the potential signal cross-talk and interference. However, the physical discomfort and psychological fears of an invasive procedure would have made it difficult to recruit subjects.
Another weakness was the distance the net was from the release point. In competitive softball, the pitching distance from the mound is 43 feet. The distance in our study was 20 feet from the simulated mound to the safety net. This could have led to pitchers not throwing at 100% for each of their trials. As documented in our demographic table, 40% of pitchers felt they did not give their maximum effort, as measured by a score of 10 on a 1 to 10 Likert-type scale.
Another weakness was that this study was performed in a controlled laboratory environment and not in game-type settings. This study was designed to delineate muscle activity as an initial investigation into forearm muscle activity during the windmill softball pitch. Overuse injuries will occur in environments where fatigue will play a role; however, in this study, we were not delineating muscle activity in a fatigue setting. The information from our study will be used to determine what exactly is happening during the windmill softball pitch, and hopefully allow programs to be developed to focus on arm strength in the right areas to prevent fatigue injuries that commonly occur in windmill softball pitchers.
Finally, the number of pitchers we used was at the lower end for accepted statistical significance. We attempted to recruit 20 pitchers; however, several collegiate coaches did not want their pitchers participating in this study, even though we had prior NCAA clearance for student athlete participation.
Eighty percent of our study population was composed of freshman- and sophomore-level pitchers. While these younger pitchers may allow us to more closely relate to what high school pitchers are experiencing, we are not able to offer a strong generalization of our results to collegiate pitchers at the junior or senior level who have more experience with their technical skills.
Conclusion
This study documented muscle activation patterns that may be helpful in differentiating the stress on the upper extremity, specifically the elbow, due to pitch selection. There is a concern for risk of fatigue injury in the upper extremity during the windmill softball pitch. Further studies will be necessary to confirm and expand on these results.
Acknowledgment
The authors thank Shinichiro Sugiura, MS, ATC, PES, CES, and Jacob Lauver, MS, for their expertise in data collection and processing.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: D.T.R. received funding through an application grant sponsored by the Centers for Osteopathic Research and Education. This grant is affiliated with the Ohio University Heritage College of Osteopathic Medicine for the advancement of research with osteopathic residents and medical students.
References
- 1. Argo D, Trenhaile SW, Savoie FH, Field LD. Operative treatment of ulnar collateral ligament insufficiency of the elbow in female athletes. Am J Sports Med. 2006;34:431–437. [DOI] [PubMed] [Google Scholar]
- 2. Barrentine S, Fleisig G, Whiteside J, Escamilla RF, Andrews JR. Biomechanics of the windmill softball pitching with implications about injury mechanisms at the shoulder and elbow. J Orthop Sports Phys Ther. 1998;28:405–415. [DOI] [PubMed] [Google Scholar]
- 3. Cram JR, Kasman GS, Holtz J. Introduction to Surface Electromyography. Gaithersburg, MD: Aspen; 1998. [Google Scholar]
- 4. Doyle FM. Review of the windmill softball pitch: biomechanics and injuries. J Chir Med. 2004;3:53–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Hill JL, Humphries B, Weidner T, Newton RU. Female collegiate windmill pitchers: influences to injury incidence. J Strength Cond Res. 2004;18:426–431. [DOI] [PubMed] [Google Scholar]
- 6. Loosli AR, Requa RK, Garrick JG, Hanley E. Injuries to pitchers in women’s collegiate fast-pitch softball. Am J Sports Med. 1992;20:35–37. [DOI] [PubMed] [Google Scholar]
- 7. Maffet MW, Jobe FW, Pink MM, Brault J, Mathiyakom W. Shoulder muscle firing patterns during the windmill softball pitch. Am J Sports Med. 1997;25:369–374. [DOI] [PubMed] [Google Scholar]
- 8. Meyers MC, Brown BR, Bloom JA. Fast pitch softball injuries. Sports Med. 2001;31:61–73. [DOI] [PubMed] [Google Scholar]
- 9. Oliver GD, Dwelly PM, Kwon YH. Kinematic motion of the windmill softball pitch in prepubescent and pubescent girls. J Strength Cond Res. 2010;24:2400–2407. [DOI] [PubMed] [Google Scholar]
- 10. Park MC, Ahmad CS. Dynamic contributions of the flexor-pronator mass to elbow valgus stability. J Bone Joint Surg Am. 2004;86A:2268–2274. [DOI] [PubMed] [Google Scholar]
- 11. Perotto AO, Delagi EF, Iazzetti JM. Anatomical Guide for the Electromyographer: The Limbs and Trunk. 4th ed Springfield, IL: Charles C. Thomas; 2005. [Google Scholar]
- 12. Rojas IL, Provencher MT, Bhatia S, et al. Biceps activity during windmill softball pitching: injury implications and comparison with overhand throwing. Am J Sports Med. 2009;37:558–565. [DOI] [PubMed] [Google Scholar]
- 13. Tanabe S, Nakahira J, Bando E, Yamaguchi H, Miyamoto H, Yamamoto A. Fatigue fracture of the ulna occurring in pitchers of fast-pitch softball. Am J Sports Med. 1991;19:317–321. [DOI] [PubMed] [Google Scholar]
- 14. Udall JH, Fitzpatrick MJ, McGarry MH, Leba TB, Lee TQ. Effects of flexor-pronator muscle loading on valgus stability of the elbow with an intact, stretched, and resected medial collateral ligament. J Shoulder Elbow Surg. 2009;18:773–778. [DOI] [PubMed] [Google Scholar]
- 15. Werner SL, Guido JA, McNeice RP, Richardson JL, Delude NA, Stewart GW. Biomechanics of youth windmill softball pitching. Am J Sports Med. 2005;33:552–560. [DOI] [PubMed] [Google Scholar]
- 16. Werner SL, Jones DG, Guido JA, Brunet ME. Kinematics and kinetics of elite windmill softball pitching. Am J Sports Med. 2006;34:597–603. [DOI] [PubMed] [Google Scholar]