

Abstract
Background:
There are little published data on factors relating to low back pain in the younger athletic population.
Hypothesis:
Independent predictors of recovery and return to participation in sports could be determined by event analysis, which investigates the impacts of covariates, including age, position, and injury type, on the risk of delayed recovery after injury.
Study Design:
Descriptive epidemiology study.
Methods:
This study examined 41 English Premiership soccer academy squads consisting of 12,306 player seasons for the incidence of lower back injury, injury severity, and investigated time to recovery in relation to potential risk factors. Injury risk was assessed for different times in a match and season, mechanism of injury, player position, player age, and competitive compared with noncompetitive play.
Results:
A total of 310 (3.0% of all injuries sustained in the population) lumbar spine injuries were recorded. Overall, 10,265 training days (median, 14 days; interquartile range, 8-30 days) were lost. The risk of injury increased as the first half progressed and was maintained throughout the second half with a contact mechanism and with increasing age. Neither competitive play compared with noncompetitive play nor player position had an effect on injury incidence. Prognostic factors for poor recovery were bony injuries and increasing age.
Conclusion:
These findings indicate that prolonged absence from training after a back injury is seen, especially in bony injuries and in older adolescents. It is suggested that there should be a low threshold for investigation of adolescent patients with back pain in the hope of early appropriate management of more severe diagnoses.
Keywords: lower back pain, LBP, youth, adolescence, soccer, risk factors, recovery, outcomes, spondylolysis
Lower back pain (LBP) is a common and potentially debilitating problem almost exclusively thought to affect the adult population.7 However, closer scrutiny reveals an incidence as high as 28% among athletic adolescents,26 with a reported lifetime prevalence of LBP ranging from 30% to 74%.1,2,13,25 Known risk factors for LBP in adolescence include rapid growth rate, smoking, and thigh muscle imbalance.8 Participation in competitive sports in youth may also predispose to LBP,11,13,15,26 with 1 study estimating that athletes are 4 times more likely to complain of such symptoms compared with nonathletes.11 However, this is not a consistent complaint, and other authors have found no evidence of such effect.8,16,19 Epidemiological work suggests that lower back injuries in this adolescent population contribute 1.8% to 14%17,22,27,28 of the total injury burden, with symptoms also being reported in adulthood.12 Despite this, there remains a lack of understanding of factors influencing recovery from low back complex symptoms in the active youth population. Access to earlier intervention in those most at risk of delayed recovery may offer an improved outcome.
Soccer is the most popular sport worldwide, and globally, there has been an expansion of dedicated soccer academies to accommodate the increasing desire to participate at a high level. The incidence, demographics, and risk factors for back injuries in a prospectively studied cohort of youth academy soccer players were evaluated. Our hypothesis was that independent predictors of recovery and return to participation in sports could be determined by event analysis, which investigated the impacts of covariates, including age, position, and injury type, on the risk of delayed recovery after injury.
Methods
Data Collection
Between November 1998 and January 2006, the English Football Association required all 41 English soccer youth professional academies to prospectively collect injury data for their players aged between ages 8 and 19 years. The player or their legal guardians gave consent for data collection. The data were collected locally on a standardized pro forma by qualified medical personnel and were made anonymous before being forwarded on a weekly basis to the FA’s headquarters in Lilleshall, United Kingdom. The data included the following: personal player information, including a unique identification code, the mechanism (player-to-player contact vs noncontact), timing and nature of the injury, the time to return to full participation, and any further clinical investigations that were required.
These prospective data were analyzed for players aged between 8 and 16 years for the 5 complete seasons beginning in May 2000 and ending in May 2005. There were 12,306 players included in this study, at an average of 2461 players per season. The number of players at risk by year and age group are shown in Table 1. For the purposes of this study, we only analyzed injuries affecting the lumbar spine, as identified by the unique injury code from the data set.
TABLE 1.
Number of Participants at Risk for Each Year of the Study by Age Group
| Season | Age Group, y | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|
| <9 | <10 | <11 | <12 | <13 | <14 | <15 | <16 | ||
| 1 (as of May 1, 2001) | 274 | 290 | 323 | 331 | 357 | 413 | 326 | 323 | 2637 |
| 2 (as of May 1, 2002) | 265 | 298 | 300 | 353 | 321 | 397 | 305 | 336 | 2575 |
| 3 (as of May 1, 2003) | 267 | 297 | 316 | 313 | 333 | 362 | 272 | 304 | 2464 |
| 4 (as of May 1, 2004) | 274 | 298 | 306 | 320 | 309 | 339 | 269 | 237 | 2352 |
| 5 (as of May 1, 2005) | 249 | 273 | 299 | 330 | 309 | 329 | 257 | 232 | 2278 |
| Total | 1329 | 1456 | 1544 | 1647 | 1629 | 1840 | 1429 | 1432 | 12,306 |
| Mean (standard deviation) | 266 (10) | 291 (11) | 309 (10) | 329 (15) | 326 (20) | 308 (36) | 286 (29) | 286 (49) | |
Ethical approval for the use of these data was obtained from the local ethics committee.
Definitions
The Union of European Football Associations (UEFA) and the Federation Internationale de Football Association (FIFA) Medical Assessment and Research Centres (F-MARC) models for calculating the injury rate per 1000 hours of exposure and definitions of time-loss injury, injury severity, training exposure, and match exposure were applied to the data set.9,10 An injury was defined as an absence from participating in full training and matches for 48 hours or longer. Moderate injuries were defined as an 8- to 28-day absence, and severe injuries as an absence ≥28 days, as classified by the UEFA model for defining injury severity.10 Absences through illness or injury sustained outside of the academy were not included.
Statistical Analysis
A multivariate analysis of factors associated with injury to the lower back was not possible because of poor conditioning; specifically, the cell counts for certain combinations of factors were zero or near zero. Instead, Wilcoxon and Fisher exact tests were used to examine the relationship between time of injury, contact versus noncontact injury mechanism, age of player, competitive play versus noncompetitive play, and player position on the number of injuries in each class. All analyses were performed in R (R Development Core Team, Vienna, Austria).24
Event Analysis
Event analysis was used to investigate the factors that had an impact on the time to recovery from different injuries. We investigated the extent to which time to recovery (the event) was dependent on various risk factors using Cox proportional hazard models following the approach of Therneau.21,29 The risk factors considered as covariates were as follows: age at injury or age class, nature of injury or grouped nature of injury (fractures, bony tissue injuries, soft tissue injuries, and other; Table 2), body side (dominant, nondominant, bilateral, not recorded), activity at injury (competitive, noncompetitive), injury mechanism (contact, noncontact), playing position (goalkeeper, defense, midfield, attack), and time category (22.5-minute intervals labeled as early first half, late first half, early second half, late second half, other). We used stepwise reduction to identify the parsimonious model from a full model with all covariates. To do this, we progressively removed nonsignificant covariates from the model until only significant covariates were left. We used a threshold for removal of P > .05. We tested assumptions of proportionality in the parsimonious models in 2 ways. First, we plotted time-dependent coefficients for each covariate against time and assessed the change in coefficients with time visually. Second, we undertook a formal test correlating the scaled Schoenfeld residuals for each model with time for each covariate and assessed significance with a 2-sided test (significance denoting evidence for deviation from a constant hazard of infection in relation to that covariate through time). All models were fitted with the Survival library of Therneau in R.24
TABLE 2.
Injury Diagnoses
| Nature of Injury | Frequency | % | Group |
|---|---|---|---|
| Low back pain | 153 | 49.4 | Soft tissue |
| Strain | 47 | 15.2 | Soft tissue |
| Not recorded | 21 | 6.8 | Other |
| Other diagnosis | 14 | 4.5 | Other |
| Spondylolysis | 13 | 4.2 | Bony tissue |
| Tissue bruising | 12 | 3.9 | Soft tissue |
| Muscular contusion | 11 | 3.5 | Soft tissue |
| Inflammatory synovitis | 10 | 3.2 | Bony tissue |
| Sprain | 9 | 2.9 | Bony tissue |
| Spondylolysthesis | 5 | 1.6 | Bony tissue |
| Fracture | 4 | 1.3 | Fracture |
| Neural | 4 | 1.3 | Other |
| Periostitis | 4 | 1.3 | Bony tissue |
| Capsular tear | 1 | 0.3 | Bony tissue |
| Chondral lesion | 1 | 0.3 | Bony tissue |
| Dislocation | 1 | 0.3 | Bony tissue |
| Total | 310 | 100 |
The response was the time taken to return to sport following injury. Because of the low numbers of injuries in the ages 9, 10, and 11 years (n = 1, 1, and 3, respectively), only the players younger than 12 years and older age groups were included in the event analysis.
Results
During the 5-year study period, there were 12,306 academy players across all age groups (age <9 to age <16 years) at risk of injury. These players incurred a total of 10,225 musculoskeletal injuries between them. Of these, 310 (3.0%) were lumbar spine injuries. The majority of these were classified as LBP (49%; n = 153), with strains (15%; n = 47) and spondylolysis (4%; n = 13) being the second and third most common diagnoses, respectively (Table 2). The diagnosis was not recorded in 21 (6.8%) cases. Analysis by recorded anatomical site (Table 3) showed that 138 (45%) cases occurred in the lumbar region, 37 (12%) in the erector spinae muscles, and 18 (6%) in the quadratus lumborum muscles. Anatomical site was not recorded in 63 (20%) cases.
TABLE 3.
Injury by Anatomical Site
| Anatomical Site | Frequency | % |
|---|---|---|
| Lumbar | 138 | 44.5 |
| Not recorded | 63 | 20.3 |
| Erector spinae | 37 | 11.9 |
| Quadratus lumborum | 18 | 5.8 |
| Facet joint | 15 | 4.8 |
| Sacro-iliac | 14 | 4.5 |
| Coccyx | 7 | 2.3 |
| Sacrum | 7 | 2.3 |
| Ilium | 4 | 1.3 |
| Nerve related | 2 | 0.6 |
| Multifidi | 2 | 0.6 |
| Thoracic | 2 | 0.6 |
| Oblique | 1 | 0.3 |
| Total | 244 | 99.8 |
After the different injuries were grouped (described in Methods), certain diagnoses were associated with longer absences from soccer, as measured by the median (Table 4). Fractures resulted in the longest absence from training (median, 149 days), followed by bony type injuries (pain from a bony structure without definite radiological evidence of a fracture) (median, 15.5 days) and soft tissue injuries (median, 13 days). More than three quarters of these bony injuries and fractures were classified as either moderate (51%; n = 158) or severe (24%; n = 73); the remaining injuries were minor (21%; n = 64) or slight (2%; n = 7), and the duration of 8 injuries was not recorded. Overall, 10,265 training days (median, 14 days; interquartile range [IQR], 8-30 days) were lost due to lumbar spine injuries (Figure 1).
TABLE 4.
Recovery Time by Diagnosis
| Diagnosis | Recovery Time, d | |
|---|---|---|
| Median | Interquartile Range | |
| Fracture (n = 4) | 148.5 | 98.5-191 |
| Bony tissue (n = 44) | 15.5 | 8-82 |
| Soft tissue (n = 223) | 13 | 7-24 |
| Not recorded (n = 39) | 17.5 | 9-32 |
Figure 1.
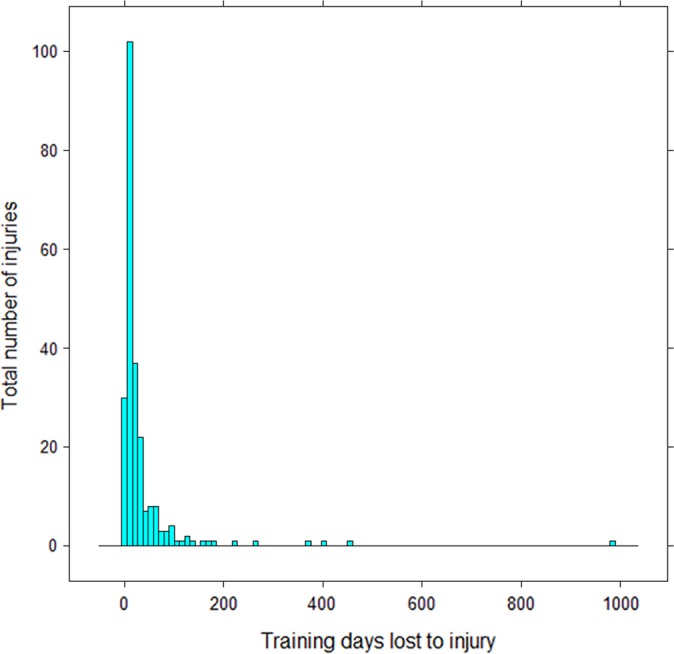
Frequency distribution of number of training days lost to muscle injuries.
The risk of injury increased in the second half of competitive matches compared with the first half, just reaching statistical significance (Wilcoxon rank sum test with continuity correction, W = 21; P = .05). Injury risk also increased in the second part of the first half, and this risk persisted throughout the second half (Figure 2C). There were also 2 peaks in injury incidence during the year: one at the beginning of the season in September and another after the winter break, in January.
Figure 2.

Descriptive statistics of the data. (A) Average monthly incidence of injury by severity. (B) Annualized injury incidence/1000 hours of exposure for age groups <9 to <16 years. (C) Number of injuries/year for the 4 periods during the match. (D) Average monthly incidence of injury by competitive environment. (E) Average monthly incidence of injury by mechanism. (F) Number of injuries/year by position played. Box-and-whisker plots in B, C, and F: the dot indicates the median and the box indicates the interquartile range (IQR).
Contact with another player accounted for a higher number of injuries compared with a non-contact mechanism (W = 131, P < .001) (Figure 2E), and there was a clear trend of increasing injury incidence per 1000 hours of exposure time with increasing age, which peaked in the <15-year age group (Figure 2B). This trend was confirmed with generalized linear modeling, with ordered factors categorizing age classes; the incidence of injury in age groups <14, <15, and <16 years was significantly higher than in the younger age groups (Table 5).
TABLE 5.
Results of a Generalized Linear Model With Incidence of Injury per 1000 Hours of Exposure as the Response and Age Class as an Ordered Predictora
| n | Estimate | SE | t Value | Pr(>|t|) | |
|---|---|---|---|---|---|
| Intercept | 0.020 | 0.050 | 0.402 | 0.691 | |
| Age class, y | |||||
| <10 | 3 | –0.001 | 0.058 | –0.018 | 0.986 |
| <11 | 3 | –0.002 | 0.058 | –0.035 | 0.972 |
| <12 | 4 | 0.007 | 0.056 | 0.132 | 0.896 |
| <13 | 4 | 0.068 | 0.056 | 1.215 | 0.237 |
| <14 | 5 | 0.171 | 0.055 | 3.104 | 0.005 |
| <15 | 5 | 0.268 | 0.055 | 4.847 | <0.001 |
| <16 | 5 | 0.159 | 0.055 | 2.871 | 0.009 |
aThe age class of players <9 years (n = 1) was omitted because of low cell counts. SE, standard error.
Neither competitive play compared with noncompetitive play (W = 968.5, P = .70) (Figure 2D) nor player position (Fisher exact test for count data, P = .68; Pearson χ2 test = 1.62, df = 3, P = .65) (Figure 2F) had an effect on injury incidence.
Event Analysis
The return to sport following injury was modeled as an event, and survival curves describing the probability of returning to sport with time were produced. Cox proportional hazards were used to identify those risk factors or covariates that influenced the probability of returning to sport. As expected, risk of not returning to sport was very high immediately after the injury but decreased as healing progressed (Figures 3 and 4). Nature of injury was a significant risk factor influencing time to recovery, with fractures and bony tissue injuries both found to have a lower risk of recovery (reduction of 76% and 44%, respectively) and hence, an extended time to recovery compared with soft tissue injuries (Table 6). Risk of recovery was dependent on the age at which the injury occurred, with each year of age reducing the risk of recovery by 13%, indicating that older players took longer times to recover. These risks are illustrated in Figures 3 and 4, which present predicted survival curves (ie, probability of returning to sport with time) for each type of injury in a 12-year-old and 16-year-old. Inclusion of year as a covariate was nonsignificant (P = .32), indicating that there was no significant trend in improvement of recovery since the beginning of the study. There was no violation of the assumption that hazards were proportional with time.
Figure 3.

Survival curves representing the probability of not returning to sport as time from injury increases for all combinations of significant covariates at injury age 12 years. Dashed line, 95% confidence intervals.
Figure 4.

Survival curves representing the probability of not returning to sport as time from injury increases for all combinations of significant covariates at injury age 16 years. Dashed line, 95% confidence intervals.
TABLE 6.
Event Analysis of Back Injuries Relative to the Base Chance Represented by Muscular Injuriesa
| Event Analysis | Proportionality of hazard | |||||||
|---|---|---|---|---|---|---|---|---|
| Coeff | Exp(Coeff) | SE(Coeff) | z | Pr(>|z|) | ρ | χ2 | Pr(<|ρ|) | |
| Age at injury | –0.133 | 0.875 | 0.053 | –2.531 | 0.011 | 0.073 | 1.760 | 0.185 |
| Nature of injury | ||||||||
| Bony Tissue | –0.581 | 0.559 | 0.181 | –3.219 | 0.001 | –0.105 | 3.280 | 0.070 |
| Fracture | –1.429 | 0.239 | 0.510 | –2.802 | 0.005 | 0.092 | 2.240 | 0.135 |
| Other | –0.181 | 0.834 | 0.177 | –1.021 | 0.307 | 0.130 | 4.900 | 0.027 |
aThe exponent of the coefficient (Exp[Coeff]), if significant, is indicative of the proportional change in hazard due to the variable. For the proportionality of hazard test, rho (ρ) is the correlation coefficient between survival time and the Schonfield residuals. Coeff, coefficient; SE, standard error.
Discussion
This study has provided a detailed analysis of the patterns and risk factors for poor recovery following traumatic back injury in male youth soccer players studied prospectively over a 5-year period from a national academy program. The key findings were an increased risk of lower back injury with increasing player age (peaking in the <15-year age group), with a contact mechanism, in the second part of the first half (a risk that was maintained throughout the second half), and with peaks of injury during the months of September and January (beginnings of both halves of the season). In contrast to previous studies examining injury to the thigh muscle complex and ankle, the risk of back injury was not influenced by competitive play or player position.5,6 A higher risk of delayed recovery was significantly associated with fractures and bony type injuries. Older players were both at higher risk of injury and required longer time to recovery. However, it may be suggested that older (more competitive) players may have a higher threshold for presenting with injury, thus the severity of injuries in the older group may have been greater.
While low back pain is believed to be a common clinical problem, the etiology of such and associated factors in the athletic population remain unclear. Sato et al26 demonstrated that 28.8% of youths similar in age to our cohort had experienced LBP in their lifetimes. In our work, back injuries contributed to 3% of the overall injury burden, a figure similar to other studies, which found rates ranging from 1.8% to 4%.22,28 This was lower than the 9.8% found in a 10-year study by Le Gall et al,17 who prospectively studied 528 elite French academy soccer players aged 14 to 16 years. The differences between our findings and other authors may be attributable to varying injury definitions, training schedules, ages, and cultures between the player cohorts. Despite only forming a small proportion of injuries recorded, back injuries result in a significant loss of time from participation in sport (median, 14 days; IQR, 8-28 days). This is a longer absence than that experienced with thigh muscle injuries within the same cohort (median, 13 days; IQR, 7-22 days).5
In our cohort, approximately three quarters of all back injuries were categorized as muscular in nature. This is at odds with results from smaller existing studies where up to 47% of LBP cases in adolescent athletes are a result of structural problems, for example, spondylolysis.18 We believe this reflects closer observation in our academy-supervised cohorts. In the current study, bony type injuries accounted for only 13% of the total. This may be because of fewer hyperextension and rotation movements of the lumbar spine (known risk factors for spondylolysis) during soccer compared with other sports.23 The analysis showed that structural problems such as fractures and bony type injuries were significantly associated with the poorest outcomes.
This study supports the contention that LBP is a significant cause of musculoskeletal dysfunction in this active, adolescent population. Earlier diagnosis allows for prompt initiation of appropriate management, and it is our contention that this group should have access to routine plain radiograph investigation followed by magnetic resonance imaging (MRI), if indicated. Consequently, it has been recommended that back pain in adolescent athletes lasting longer than 3 weeks should undergo radiological investigation to rule out underlying structural damage.4,23 This would initially involve anteroposterior, lateral, and left and right oblique radiographs so as to not miss the 20% of cases involving unilateral defects.30 Campbell et al3 showed that MRI is equally effective and reliable as combined computed tomography and single photon emission computed tomography in the diagnosis of juvenile spondylolysis. However, MRI has the added benefits of allowing early detection of acute stress reactions in the pars before they develop into fractures and the ability to identify other pathologies that could potentially cause LBP.3
The risk of injury increased after the first part of the first half of competitive play. This risk was maintained throughout the second half, which suggests that the half-time break was not long enough for sufficient muscle recovery from fatigue.14 This pattern is similar to our previous work on the thigh muscle complex5; however, it is different from work on the ankle6 and knee,20 where the risk of injury was greatest in the second part of each half but reduced directly after halftime. It has been suggested that longer halftime breaks or substituting fatigued players may be useful strategies to avoid injury in this situation, but clearly this has limitations due to player numbers.5
There were 2 peaks in the incidence of back injuries: one after summer break, in September, and another after winter break, in January. This is similar to other studies of youth soccer players.5,6,17,20 An increased risk of injury after a prolonged break from soccer suggests that players may be deconditioned and therefore unable to efficiently handle the high demands associated with a return to intense activity. Le Gall et al17 did not experience a peak in injuries after the winter break and proposed that this was because of the shorter but more frequent breaks from soccer their players experienced. A more gradual return to soccer may also avoid such problems.30
We do accept that there were limitations to our study. There may have been variability in diagnosis because of the differing backgrounds of health care professionals across the number of academies involved. Clinical assessment was used to diagnose injury in the majority of cases, and there was limited access to early radiological imaging. This may have resulted in the underreporting of injuries such as spondylolysis. Finally, data for this study were collected before UEFA recommendations on injury definition by time loss of 24 hours (instead the 48-hour definition used) were introduced.10 This may have resulted in some minor injuries being unrecorded.
Conclusion
We have found that the risk of lower back injury increases with age of the adolescent soccer player and is more likely with a contact mechanism, in the second part of the first half, and after the summer and winter breaks. Players who experience LBP with underlying structural damage are at greatest risk of prolonged injury. We would strongly recommend examination by a specialist and radiographs, if necessary, to facilitate recovery. Longer follow-up is required to identify the relationship between these injury patterns and adult lower back dysfunction.
Acknowledgment
The authors acknowledge the English Football Association for their support.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
References
- 1. Balague F, Dutoit G, Waldburger M. Low back pain in schoolchildren. An epidemiological study. Scand J Rehabil Med. 1998;20:175–179. [PubMed] [Google Scholar]
- 2. Balague F, Skovron M, Nordin M, Dutoit G, Pol LR, Waldburger M. Low back pain in schoolchildren. A study of familial and psychological factors. Spine (Phila Pa 1976). 1995;20:1265–1270. [DOI] [PubMed] [Google Scholar]
- 3. Campbell RS, Grainger AJ, Hide IG, Papastefanou S, Greenough CG. Juvenile spondylolysis: a comparative analysis of CT, SPECT and MRI. Skeletal Radiol. 2005;34:63–73. [DOI] [PubMed] [Google Scholar]
- 4. Cassas KJ, Cassettari-Wayhs A. Childhood and adolescent sports-related overuse injuries. Am Fam Physician. 2006;73:1014–1022. [PubMed] [Google Scholar]
- 5. Cloke DJ, Moore O, Shah T, Rushton S, Shirley MD, Deehan DJ. Thigh muscle injuries in youth soccer: predictors of recovery. Am J Sports Med. 2012;40:433–439. [DOI] [PubMed] [Google Scholar]
- 6. Cloke DJ, Spencer S, Hodson A, Deehan D. The epidemiology of ankle injuries occurring in English Football Association academies. Br J Sports Med. 2009;43:1119–1125. [DOI] [PubMed] [Google Scholar]
- 7. Deyo RA, Cherkin D, Conrad D, Volinn E. Cost, controversy, crisis: low back pain and the health of the public. Annu Rev Public Health. 1991;12:141–156. [DOI] [PubMed] [Google Scholar]
- 8. Feldman D, Shrier I, Rossignol M, Abenhaim L. Risk factors for the development of low back pain in adolescence. Am J Epidemiol. 2001;154:30–36. [DOI] [PubMed] [Google Scholar]
- 9. Fuller CW, Ekstrand J, Junge A, et al. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Br J Sports Med. 2006;40:193–201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Hagglund M, Walden M, Bahr R, Ekstrand J. Methods for epidemiological study of injuries to professional football players: developing the UEFA model. Br J Sports Med. 2005;39:340–346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Hangai M, Kaneoka K, Okubo Y, et al. Relationship between low back pain and competitive sports activities during youth. Am J Sports Med. 2010;38:791–796. [DOI] [PubMed] [Google Scholar]
- 12. Harreby M, Neergaard K, Hesselsoe G, Kjer J. Are radiologic changes in the thoracic and lumbar spine of adolescents risk factors for low back pain in adults? A 25-year prospective cohort study of 640 school children. Spine (Phila Pa 1976). 1995;20:2298–2302. [DOI] [PubMed] [Google Scholar]
- 13. Harreby M, Nygaard B, Jessen T, et al. Risk factors for low back pain in a cohort of 1389 Danish school children: an epidemiologic study. Eur Spine J. 1999;8:444–450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Hawkins RD, Fuller CW. A prospective epidemiological study of injuries in four English professional football clubs. Br J Sports Med. 1999;33:196–203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Kovacs FM, Gestoso M, Gil del Real MT, Lopez J, Mufraggi N, Mendez JI. Risk factors for non-specific low back pain in schoolchildren and their parents: a population based study. Pain. 2003;103:259–268. [DOI] [PubMed] [Google Scholar]
- 16. Kujala UM, Salminen JJ, Taimela S, Oksanen A, Jaakkola L. Subject characteristics and low back pain in young athletes and nonathletes. Med Sci Sports Exerc. 1992;24:627–632. [PubMed] [Google Scholar]
- 17. Le Gall F, Carling C, Reilly T, Vendewalle H, Church J, Rochcongar P. Incidence of injuries in elite French youth soccer players: a 10-season study. Am J Sports Med. 2006;34:928–938. [DOI] [PubMed] [Google Scholar]
- 18. Micheli LJ, Wood R. Back pain in young athletes. Arch Pediatr Adolesc Med. 1995;149:15–18. [DOI] [PubMed] [Google Scholar]
- 19. Mogensen AM, Gausel AM, Wedderkopp N, Kjaer P, Leboeuf-Yde C. Is active participation in specific sport activities linked with back pain? Scand J Med Sci Sports. 2007;17:680–686. [DOI] [PubMed] [Google Scholar]
- 20. Moore O, Cloke DJ, Avery PJ, Beasley I, Deehan DJ. English Premiership Academy knee injuries: lessons from a 5 year study. J Sports Sci. 2011;29:1535–1544. [DOI] [PubMed] [Google Scholar]
- 21. Pinheiro JC, Bates DM. Mixed effects models in s and s-plus. Stat Comput. 2000;6:289–296. [Google Scholar]
- 22. Price RJ, Hawkins RD, Hulse MA, Hodson A. The Football Association medical research programme: an audit of injuries in academy youth football. Br J Sports Med. 2004;38:466–471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Purcell L, Micheli LJ. Low back pain in young athletes. Sports Health. 2009;1:212–222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. R Development Core Team. R: a language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; 2011. [Google Scholar]
- 25. Salminen JJ, Pentti J, Terho P. Low back pain and disability in 14-year-old schoolchildren. Acta Paediatr. 1992;81:1035–1039. [DOI] [PubMed] [Google Scholar]
- 26. Sato T, Ito T, Hirano T, et al. Low back pain in childhood and adolescence: a cross-sectional study in Niigata City. Eur Spine J. 2008;17:1441–1447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Schimdt-Olsen S, Jorgensen U, Kaalund S, Sorensen J. Injuries among young soccer players. Am J Sports Med. 1991;19:273–275. [DOI] [PubMed] [Google Scholar]
- 28. Schimdt-Olsen S, Bunemann LK, Lade V, Brassoe JO. Soccer injuries of youth. Br J Sports Med. 1985;19:161–164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Therneau TM, Grambsch PM. Modelling Survival Data. Statistics for Biology and Health. New York, NY: Springer; 2000. [Google Scholar]
- 30. Trainor TJ, Trainor MA. Etiology of low back pain in athletes. Curr Sports Med Rep. 2004;3:41–46. [DOI] [PubMed] [Google Scholar]