

Abstract
Background:
Hamstring injuries are the second most common injury causing missed days in professional baseball field players. Recent studies have shown the preventive benefit of eccentric conditioning on the hamstring muscle group in injury prevention. Specifically, Nordic-type exercises have been shown to decrease the incidence of acute hamstring injuries in professional athletes.
Purpose:
This was a prospective study performed in coordination with a single Major League Baseball (MLB) organization (major and minor league teams) that targeted the effects of Nordic exercises on the incidence of acute hamstring injuries in the professional-level baseball player.
Study Design:
Prospective cohort study; Level of evidence, 2.
Methods:
The daily workouts of 283 professional baseball players throughout all levels of a single MLB organization were prospectively recorded. The intervention group participated in the Nordic exercise program and was compared with a randomly selected control group of professional athletes within the organization not participating in the exercise program. The incidence of hamstring injuries in both groups was compared, and the total number of days missed due to injury was compared with the 2 previous seasons.
Results:
There were 10 hamstring injuries that occurred during the 2012 season among the 283 professional athletes that required removal from play. There were no injuries that occurred in the intervention group (n = 65, 0.00%; P = .0381). The number needed to treat (NNT) to prevent 1 hamstring injury was 11.3. The average repetitions per week of the injured group were assessed at multiple time points (2, 4, 6, and total weeks) prior to injury. There were significantly fewer repetitions per week performed in the injured group at all time points compared with overall average repetitions per week in the noninjured group (P = .0459, .0127, .0164, and .0299, respectively). After beginning the Nordic exercise program, there were 136 total days missed due to a hamstring injury during the 2012 season. This number was less than the 2011 season (273 days missed) and the 2010 season (309 days missed).
Conclusion:
Study results indicate the initiation of Nordic hamstring exercises may decrease the incidence of acute hamstring injuries and potentially decrease the total number of days missed due to injury in professional baseball players.
Clinical Relevance:
The financial and competitive interest in professional baseball players is of large importance to the player, team, and fans. Prevention of injuries is as important to all parties involved as the treatment and rehabilitation following an injury. This prospective study shows the initiation of a simple, free exercise can reduce the incidence of hamstring injury in the professional-level baseball player.
Keywords: hamstring injury, injury prevention, professional-level athlete, baseball
An injury to a professional baseball player causing missed days and time on the disabled list is of large competitive and financial interest for professional baseball organizations. For the athlete, the injury can be devastating, with prolonged down time and potential for chronic impairment. Hamstring injuries represent an exceedingly common proportion of professional baseball injuries. In the top level of Major League Baseball (MLB), hamstring injuries are the fourth leading cause of days on the disabled list for all players, regardless of position (8.0% of injuries), and the second leading cause of days on the disabled list for field position players (13.7% of injuries).14 Despite these high numbers, very little preventive techniques to decrease the incidence of hamstring injury in the professional baseball player have been investigated in a prospective manner.
The function of the hamstring muscle group is hip extension and knee flexion. During walking, the force requirements of the hamstring group are significantly less than the requirement during sprinting activities.5,16 Furthermore, neuromusculoskeletal models have demonstrated peak hamstring force and stretch occur during the late-swing phase of the running gait cycle. It is at this point, when the hamstring muscles are generating tension while lengthening (eccentric contraction) to decelerate knee extension, where the hamstring muscle group is at high risk of injury.5,10,16,19 As a result, eccentric conditioning of the hamstring muscle group has been proposed as a method to prevent hamstring injuries.3,6,9,17 The majority of hamstring injuries that occur during baseball play occur during high-intensity sprinting, seemingly during this late-swing phase of the gait cycle.14 Baseball players may be at particular risk due to prolonged periods of standing with intermittent quick acceleration.
Brockett et al3 first developed a simple eccentric hamstring strength training program that was further adapted by Mjølsnes et al12 and is known as the Nordic Hamstring Exercise. Mjølsnes et al12 demonstrated the simplicity of the Nordic exercise without the need for special equipment and the ability to increase the eccentric strength in the hamstring muscles of male soccer players.12 The most widely accepted international application of the Nordic exercise has been documented in professional soccer and rugby. Petersen et al,13 in a large cluster-randomized control trial throughout all levels of professional and amateur soccer in Denmark, demonstrated that the addition of Nordic exercises decreased the rate of overall, new, and recurrent acute hamstring injuries. Brooks et al4 and Gabbe et al8 also showed that the addition of Nordic hamstring exercises reduced the incidence and severity of hamstring muscle injuries sustained in professional rugby players.
To the best of our knowledge, no investigation of the Nordic exercise in a professional baseball organization is available in the literature. Prospective examination of the Nordic exercise and its application to professional baseball is warranted. Therefore, we designed a prospective study, in coordination with a single MLB organization, examining the preventive effects of Nordic exercises on the incidence of acute hamstring injuries in the professional-level baseball player.
Materials and Methods
Participants and Study Period
Participants for this study included individuals throughout all levels of competition in a single MLB organization (major and minor league teams) for a single season. For the purposes of this study, 1 season consisted of the regular season (162 games) as well as all spring training activities prior to the season. The levels of competition included 1 MLB team, 1 AAA team, 1 AA team, 1 High A team, 1 A team, and 3 Rookie League teams. Players who were traded, released, or who had an incomplete workout data set were excluded from the study. A small subset of players that were drafted in the 2012 MLB draft during the middle of the season were included in the study as they were subjected to a minicamp with Nordic exercises initiated prior to participating in games. The ramp-up period during the rookie minicamp was the same as the ramp-up period for existing players during spring training, approximately 6 weeks. This study was approved by the institutional human subjects committee prior to the intervention or data collection.
Intervention
Prior to the beginning of the season, all strength and conditioning coaches were instructed to initiate Nordic hamstring exercises in the daily workouts of all players throughout the organization during the 2012 season excluding the 40-man roster. The 40-man roster, which includes all players signed to a major league contract who can be “called up” during the course of the season, was used as a control group in this study. The Nordic exercise could be done either with a partner or using specialized equipment. The athlete begins the exercise on his knees with his torso perpendicular to the ground, while his partner/ankle-holder applies pressure to his heels/ankles to ensure the athlete’s feet stay in contact with the ground throughout the motion of the exercise (Figure 1). The athlete then resists a forward-falling motion by eccentrically engaging the hamstring muscles (Figure 2). The athlete is instructed to resist forward-fall as long as possible, attempting to reach a position parallel to the floor. The athlete then allows his body to fall using his hands and arms to cushion the impact and quickly push up to the starting position (Figure 3). All athletes were supervised by organization strength and conditioning coaches who dictated when the exercise was performed during the training session and ensured that it was performed properly. All players were instructed to perform adequate warm-up prior to initiation of training sessions.
Figure 1.

Example of Nordic exercise starting position with athlete’s feet held in place with ankle holder. Athlete begins exercise with torso perpendicular to the floor.
Figure 2.

Example of Nordic exercise as athlete begins controlled, eccentric contraction of the hamstring muscle group lowering his body from the perpendicular to parallel position relative to the floor.
Figure 3.

Example of Nordic exercise as athlete has eccentrically lowered his body parallel to the floor preparing to push up to the starting position.
Using a standardized report form, the individual workouts of 283 professional players were prospectively recorded for the entire 2012 season, including spring training activities. All strength and conditioning coaches were contacted to ensure the accuracy of the daily workout reports at the end of the season. For this analysis, the intervention group was further separated into compliant and noncompliant groups. The compliant intervention group consisted of any player completing an average of 3.5 repetitions of the Nordic exercise per week throughout the entire season.
Injury Assessment
The athletic trainers for this MLB organization reported the occurrence of all hamstring injuries sustained, including specific details and mechanism of injury, on a standardized injury report form throughout the season. The definition of a hamstring injury for the purpose of this study was any injury to the hamstring muscle group that caused a player to be removed from the line-up for at least 1 day. Injury diagnosis was based on clinical examination, and no further imaging or diagnostic investigation was required. Recurrent hamstring injuries were not included in the study; however, the sentinel injury for a player was included for data analysis. A player was deemed to have returned to play when he was removed from the disabled list and able to participate in full baseball activities. The total number of days spent out of the line-up as a direct result of a hamstring injury for the entire organization during the 2012 season was also recorded. This was compared with similar data from the 2010 and 2011 seasons.
Statistical Analysis
All data were recorded utilizing a single Excel spreadsheet (Microsoft Corp). A Fisher exact test was used to identify proportional differences of hamstring injuries between intervention and control groups. The number needed to treat (NNT) was calculated. Differences in mean repetitions between injured and noninjured groups were calculated using the Student t test at multiple time points (total, 6, 4, and 2 weeks) prior to date of injury.
Results
A total of 283 athlete workout schedules were recorded throughout the 2012 MLB season. After subjects were excluded due to being traded, released, or having an incomplete data set, there were 243 total players included in this study. The control group was composed of those athletes on the organization’s 40-man roster. Two players on the 40-man roster were traded during the season and were not included. Four other players had nonhamstring injuries during the 2012 season that caused them to be sent to rehab assignments within the intervention group. These 4 players were subjected to Nordic exercises during the time they were playing at lower levels. As a result, these players were included in the intervention group. Any player in the intervention group who was noncompliant with the intervention exercises (performed <3.5 repetitions/week on average) was removed from the group. The final number of players in the control group was 34, and there were 65 compliant athletes within the intervention group (Figure 4). Consequently, the control group (40-man roster) had no participation in Nordic exercises, and the non–40-man roster had both a partial participation group (noncompliant, <3.5 mean repetitions/week) and the intervention group (compliant, >3.5 mean repetitions/week). Demographics and position types were evaluated and found to be similar between groups with the exception of age (Table 1).
Figure 4.
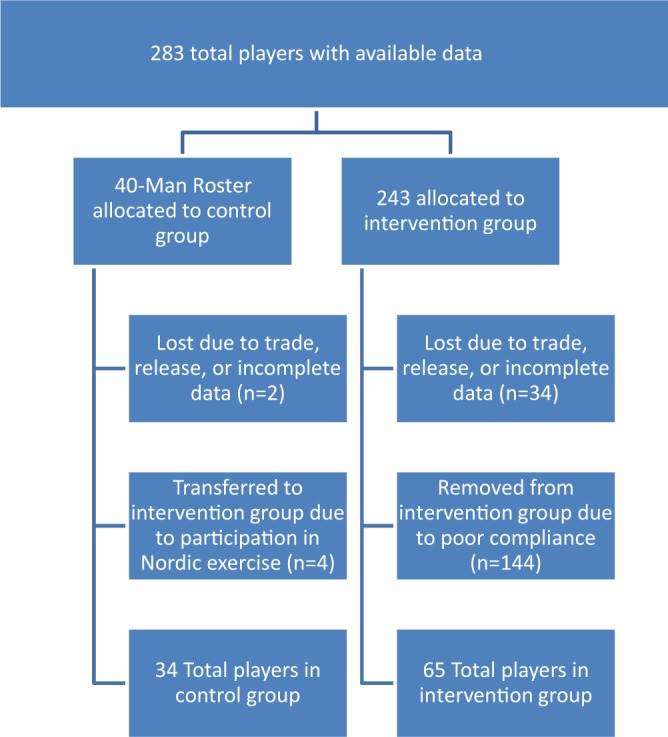
Flow diagram of intervention and control groups.
TABLE 1.
Study Baseline Characteristics: Control (40-Man) Versus Intervention Group
| Control Group | Intervention Group | P Value | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Position | |||||
| Pitcher | 17 | 50.00 | 109 | 52.15 | .48 |
| Catcher | 3 | 8.82 | 22 | 10.53 | .52 |
| Infielder | 8 | 23.53 | 43 | 20.57 | .42 |
| Outfielder | 6 | 17.65 | 35 | 16.75 | .53 |
| Age,a y | 26.618 ± 2.719 | 22.818 ± 3.083 | <.001 | ||
aAge is expressed as mean ± standard deviation.
Of the 243 athletes in this study, 10 sustained hamstring injuries during the 2012 season that required removal from play. Of the players injured, 8 were field position players and 2 were pitchers. All but 1 injury occurred during competitive play (Table 2). There were no hamstring injuries that occurred in the intervention group (n = 65, 0.00%), and 3 hamstring injuries that occurred in the control group (n = 34, 8.82%; P = .0382). The NNT for preventing 1 hamstring injury was 11.3 (Table 3). Comparing the intervention group with the control and noncompliant groups, there were significantly less injuries within the intervention group (P = .041) (Table 4). When comparing the intervention and noncompliant group versus the control group, there was a trend toward fewer injuries; however, it did not achieve significance (P = .150) (Table 5). No injuries occurred while performing the Nordic exercises.
TABLE 2.
Profiles of Injured Playersa
| Player No. | Date of Injury | Position | Injury Activity | Session | Side | Level of Play at Injury | Member of 40-Man Roster |
|---|---|---|---|---|---|---|---|
| 1 | Q3 | P | Pitching | Game | Left | Rookie | No |
| 2 | Q1 | C | Base running | Game | Left | AAA | No |
| 3 | ST | IF | Base running | Practice | Left | Rookie | No |
| 4 | Q3 | IF | Base running | Game | Right | High A | No |
| 5 | Q3 | IF | Base running | Game | Right | AA | No |
| 6 | Q2 | IF | Base running | Game | Left | Rookie | No |
| 7 | ST | P | Pitching | Game | Left | Rookie | No |
| 8 | Q4 | OF | Fielding | Game | Right | MLB | Yes |
| 9 | Q1 | IF | Base running | Game | Left | MLB | Yes |
| 10 | Q4 | OF | Base running | Game | Right | MLB | Yes |
aC, catcher; IF, infielder; MLB, Major League Baseball; OF, outfielder; P, pitcher; Q, season quarter; ST, spring training.
TABLE 3.
Acute Hamstring Injuries in Intervention Versus Control Groupa
| Group | No. of Injuries | Injury Rate, % | NNT | P Value |
|---|---|---|---|---|
| Intervention (n = 65) | 0 | 0.000 | 11.333 | .038 |
| Control (n = 34) | 3 | 8.824 |
aNNT, number needed to treat to prevent a single hamstring injury.
TABLE 4.
Acute Hamstring Injuries in the Intervention Group Versus Control and Noncompliant Groupsa
| Group | No. of Injuries | Injury Rate (%) | NNT | P Value |
|---|---|---|---|---|
| Intervention (n = 65) | 0 | 0.000 | 17.8 | .041 |
| Control + noncompliant group (n = 178) | 10 | 5.618 |
aAverage repetitions per week: >3.5 for the intervention group, <3.5 for the noncompliant group. NNT, number needed to treat to prevent a single hamstring injury.
TABLE 5.
Acute Hamstring Injuries in the Intervention and Noncompliant Groups Versus Controla
| Group | No. of Injuries | Injury Rate (%) | NNT | P Value |
|---|---|---|---|---|
| Intervention and noncompliant group (n = 209) | 7 | 3.349 | 18.267 | .150 |
| Control (n = 34) | 3 | 8.824 |
aNNT, number needed to treat to prevent a single hamstring injury.
The mean repetitions per week of the injured group was assessed at multiple time points (2 weeks, 4 weeks, 6 weeks, and total weeks) prior to injury (Table 6). There were significantly fewer repetitions per week performed in the injured group at all time points compared with the overall mean repetitions per week in the noninjured group (P = .0459, .0127, .0164, and .0299, respectively).
TABLE 6.
Average Repetitions Per Week Before Hamstring Injury
| Player | Average Repetitions per Week | |||
|---|---|---|---|---|
| 2 Weeks Prior to Injury | 4 Weeks Prior to Injury | 6 Weeks Prior to Injury | Total Weeks Prior to Injury | |
| 1 | 0 | 0 | 0 | 0 |
| 2 | 10 | 5 | 3.333 | 1.818 |
| 3 | 0 | 0 | 0 | 0 |
| 4 | 0 | 0 | 0 | 1 |
| 5 | 0 | 0 | 0 | 0.909 |
| 6 | 0 | 0 | 2.667 | 4.667 |
| 7 | 0 | 0 | 0 | 0 |
| 8 | 0 | 0 | 0 | 0 |
| 9 | 0 | 0 | 0 | 0 |
| 10 | 0 | 0 | 0 | 0 |
| Total | 1 | 0.500 | 0.600 | 0.839 |
In the 2012 season, 136 total days were missed due to hamstring injury in the intervention and control groups combined, compared with 273 days missed in 2011 and 309 days missed in 2010 (Table 7).
TABLE 7.
Total Days Missed Due to Hamstring Injury by Season
| Season | Total Days Missed |
|---|---|
| 2012 | 136 |
| 2011 | 273 |
| 2010 | 309 |
Discussion
This is the first prospective trial documenting a reduction in the incidence of hamstring injury in the professional-level baseball player after the implementation of eccentric strengthening exercise. The current literature regarding hamstring injuries in professional baseball players is scarce. The majority of publications regarding lower extremity injuries in elite-level baseball players (professional and collegiate) are limited to epidemiological surveys.7,11,14
The current literature on the preventative effects of eccentric conditioning of the hamstring muscle group was performed with soccer and rugby athletes, where, similar to baseball, there is a high incidence of hamstring injury.1,4,12,13 These studies indicate that the initiation of eccentric conditioning has a beneficial effect on injury prevention.
Eccentric muscle exercises are defined as active lengthening of muscle fibers while contracting. Proske et al showed the hamstring muscle group is maximally loaded and lengthened during the rapid, late-swing phase of the gait cycle.15 It is at this point in the gait cycle where the athlete is at greatest risk of injury to the hamstring muscle group. Mjølsnes et al12 revealed that muscle adaptation is mode specific, meaning eccentric training increases eccentric strength and concentric training increases concentric strength. Therefore, eccentric conditioning serves to potentially prevent hamstring injury. Subsequent bouts of eccentric muscle training have shown to have a cumulative, protective effect on further eccentric exercise–induced injury.18 These repeat bouts of eccentric overload produce a beneficial and protective adaptation in the length-tension curve of the muscle by recruiting more sarcomeres to allow a stronger and less injury prone contraction at longer muscle lengths.3
For the purposes of this study, a hamstring injury was defined as an injury significant enough to remove a player from the lineup for at least 1 day. This clear definition is similar to that used by Petersen et al13 and allows for appropriate legitimization of when the threshold of a debilitating injury has been crossed. Certainly, hamstring injury severity is a spectrum, and some players will compete with more severe injuries while other players will be unable to compete with relatively small injuries. We feel that utilizing imaging to assess hamstring injury severity is often unnecessary and inaccurate in predicting an athlete’s ability to play or a timeline for return to sport. We have found that the clinical assessment and physical exam are the best predictors of return to play, and utilizing the days missed due to injury is an appropriate way to document the direct financial implications to a professional team. Since these data were taken directly from the injury reports and the collective documentation by the athletic trainers and physical therapists employed by the participating major league organization, there were likely a low number of missed injuries. The low number of missed injuries combined with the completeness of the data, which included all injuries and workouts performed throughout the entire season, is considered a strength of the trial.
Another strength of the current study is the exclusion of recurrent injuries. There has been previous documentation of a high recurrence of hamstring injuries in athletes who have had a previous hamstring injury; consequently, all recurrent hamstring injuries were not included in this study.13 Recording recurrent injuries of a player that has already sustained a hamstring injury in previous seasons would likely magnify the difference between groups and lead to an incorrect conclusion.
An athlete was deemed compliant with the Nordic workout schedule if he completed an average of 3.5 repetitions per week or more during the intervention period. This allowed a more accurate representation of the intervention, when performed appropriately. When comparing both compliant and noncompliant athletes (n = 209) with the control group, hamstring injury rates were still higher in the control group (3/34 [8.82%] vs 7/209 [3.35%], respectively), favoring those athletes who performed even a small number of Nordic exercises throughout the season (Table 5); this difference did not reach significance (P = .150). When evaluating the intervention group, no injuries occurred in players with adequate compliance to the Nordic exercise. When the injury incidence of the intervention group (0/65; 0%) was compared with the injury incidence of the control group (3/34; 8.82%), the rate of hamstring injuries was significantly lower in the intervention group (P = .0382) (Table 3). Also, when the intervention group was compared with both the control and the noncompliant athletes who participated in very few Nordic exercises (n = 178), the incidence of hamstring injuries was significantly less in the intervention group (0/65 [0%] vs 10/178 [5.52%], respectively; P = .041) (Table 4).
We believe that an overall average of 3.5 repetitions per week spread throughout the entire year was an adequate level of intervention that one would begin to see therapeutic benefit. Previous studies utilizing Nordic exercises in other sports have shown significance with similar repetitions per week.4,13 Certainly, arguments could be made for either greater or less repetitions per week requirements in the intervention group. Since there are no preceding publications to quantify what the appropriate level of repetitions should be, the data were analyzed for trends and significance. It was determined that the critical number of repetitions per week needed to avoid injury was >3.5 repetitions per week on average. Consequently, this value was used to present the current data. This may be used as a guideline for future participation level in athletes who are trying to avoid injury.
Previous studies have documented the prolonged effects of eccentric training of the hamstring muscles with preseason intervention, while others indicate a need for continued training throughout the season.1,2,4,13 We felt the time points used (2, 4, 6, and total weeks prior to injury) were appropriate in determining acceptable exercise intervention to prevent injury. In our study, of the 10 injured players, none performed Nordic exercises for 6 weeks or greater during the 2012 season. Two players who had hamstring injuries had limited Nordic exercise participation. One player injured was performing the Nordic exercise at a level that one would expect benefit at 2 and 4 weeks prior to his injury. However, this was the only time throughout the season the player actually performed any Nordic exercises. The only other injured player to perform the Nordic exercises at a level of perceived benefit was a player performing the exercise adequately only during spring training. After spring training, he did not perform the exercise at all. His injury occurred near the end of the season, suggesting that performing the Nordic exercises at an adequate level may have a preventive effect that lasts for an extended period of time. The remaining 8 of the 10 injured players never performed a single repetition of the intervention exercise throughout the year. These 2 injured player profiles suggest it may be advantageous to initiate Nordic exercise in the preseason and continue at a maintenance level of participation throughout the season. Further investigation into the timing of Nordic exercise participation is warranted.
Another positive outcome was the decreased number of days missed during the 2012 season for the entire organization due to hamstring injury (Table 7). The decrease in days missed was reported in aggregate for both intervention and control groups, thus making statistical comparison difficult. However, the decrease in days missed cannot be ignored (136 days in 2012, 273 days in 2011, 309 days in 2010). Certainly, there are confounding variables that may have led to the reduction in days missed, the most obvious being the widespread emphasis of eccentric conditioning. There is also no quantification of the severity of the hamstring injuries sustained in this study beyond number of days missed. Although it could be argued that eccentric conditioning not only decreases the incidence of injuries but also decreases the severity of the injured muscle, the current study design does not allow for this conclusion. Additional trials will be needed to determine the financial benefit of eccentric strengthening to the owners and players of MLB.
When examining the difference between the intervention and control (40-man roster) groups, there was a significant difference between the mean ages of players involved. The 40-man roster typically involves older players with more baseball experience. Some may consider this a weakness. However, in our experience treating professional baseball players, hamstring injuries tend to occur in the younger athletes. The reason for this is unclear and likely multifactorial. This difference in injury incidence could be related to player experience in knowing ones limitations on the field as well as additional career years spent in specific baseball conditioning exercises. Younger, minor league players may push themselves more to fight for a spot or contract with the team, increasing their propensity for injury. The fact that the intervention group consisted of younger players, where injuries may occur at a higher incidence, further strengthens our hypothesis.
One weakness of the study was the low overall compliance of the intervention group (31.1%). One possible reason for the low compliance seen in this study is the high number of games played in professional baseball compared with other professional sports. At the highest level of professional baseball in the MLB, a team will play 162 games during the regular season, which consists of approximately 180 days. This leaves time for additional training scarce. Players do train most days throughout the season; however, eccentric conditioning has been shown to produce delayed-onset muscle soreness at greater levels than most traditional concentric conditioning.12 This increase in delayed-onset muscle soreness may have discouraged some players from performing the exercise during weeks without days off, contributing to low compliance. This is also true during the period of spring training, with as many as 3 games at different levels being played every day.
An additional weakness of the study is the self-selected compliant intervention group. A player who was more likely to perform a prescribed exercise is potentially more likely to perform other activities that could prevent injury, introducing selection bias. These activities could range from other preventive exercises, sufficient sleep regimens, or adequate hydration. The ability to control for all these variables may be futile. However, we do acknowledge this weakness in the current study. It is thought that the current analysis appropriately describes the data collected, and that a player performing a certain quantity of eccentric hamstring strengthening exercises can obtain preventive benefit.
Another limitation of the study was there was no preseason isokinetic exercise testing completed identifying players with potential muscle imbalance. These data were not collected for the purposes of this study but would certainly be important information to have, as muscle imbalance could be a confounding factor for hamstring injury. Future studies would benefit with inclusion of this information.
Conclusion
This prospective controlled trial demonstrates that the appropriate administration of Nordic exercises decreases the incidence of new hamstring injuries in the professional baseball player. Consequently, total days missed from baseball activity may also be decreased. The small time commitment and low cost of this exercise make it ideal for any baseball organization. Future investigations involving baseball players at all levels are required to fully investigate this intervention and the direct benefit to players, coaches, and owners.
Footnotes
The authors declared that they have no conflicts of interest in the publication and authorship of this contribution.
References
- 1. Arnason A, Andersen TE, Holme I, Engebretsen L, Bahr R. Prevention of hamstring strains in elite soccer: an intervention study. Scand J Med Sci Sports. 2008;18:40–48. [DOI] [PubMed] [Google Scholar]
- 2. Askling C, Karlsson J, Thorstensson A. Hamstring injury occurrence in elite soccer players after preseason strength training with eccentric overload. Scand J Med Sci Sports. 2003;13:244–250. [DOI] [PubMed] [Google Scholar]
- 3. Brockett CL, Morgan DL, Proske U. Human hamstring muscles adapt to eccentric exercise by changing optimum length. Med Sci Sports Exerc. 2001;33:783–790. [DOI] [PubMed] [Google Scholar]
- 4. Brooks JH, Fuller CW, Kemp SP, Reddin DB. Incidence, risk, and prevention of hamstring muscle injuries in professional rugby union. Am J Sports Med. 2006;34:1297–1306. [DOI] [PubMed] [Google Scholar]
- 5. Chumanov ES, Heiderscheit BC, Thelen DG. The effect of speed and influence of individual muscles on hamstring mechanics during the swing phase of sprinting. J Biomech. 2007;40:3555–3562. [DOI] [PubMed] [Google Scholar]
- 6. Croisier JL. Factors associated with recurrent hamstring injuries. Sports Med. 2004;34:681–695. [DOI] [PubMed] [Google Scholar]
- 7. Dick R, Sauers EL, Agel J, et al. Descriptive epidemiology of collegiate men’s baseball injuries: National Collegiate Athletic Association Injury Surveillance System, 1988-1989 through 2003-2004. J Athl Train. 2007;42:183–193. [PMC free article] [PubMed] [Google Scholar]
- 8. Gabbe BJ, Branson R, Bennell KL. A pilot randomised controlled trial of eccentric exercise to prevent hamstring injuries in community-level Australian Football. J Sci Med Sport. 2006;9:103–109. [DOI] [PubMed] [Google Scholar]
- 9. Goldman EF, Jones DE. Interventions for preventing hamstring injuries. Cochrane Database Syst Rev. 2010;(1):CD006782. [DOI] [PubMed] [Google Scholar]
- 10. Heiderscheit BC, Hoerth DM, Chumanov ES, Swanson SC, Thelen BJ, Thelen DG. Identifying the time of occurrence of a hamstring strain injury during treadmill running: a case study. Clin Biomech (Bristol, Avon). 2005;20:1072–1078. [DOI] [PubMed] [Google Scholar]
- 11. Janda DH. The prevention of baseball and softball injuries. Clin Orthop Relat Res. 2003;(409):20–28. [DOI] [PubMed] [Google Scholar]
- 12. Mjølsnes R, Arnason A, Osthagen T, Raastad T, Bahr R. A 10-week randomized trial comparing eccentric vs. concentric hamstring strength training in well-trained soccer players. Scand J Med Sci Sports. 2004;14:311–317. [DOI] [PubMed] [Google Scholar]
- 13. Petersen J, Thorborg K, Nielsen MB, Budtz-Jorgensen E, Holmich P. Preventive effect of eccentric training on acute hamstring injuries in men’s soccer: a cluster-randomized controlled trial. Am J Sports Med. 2011;39:2296–2303. [DOI] [PubMed] [Google Scholar]
- 14. Posner M, Cameron KL, Wolf JM, Belmont PJ, Jr, Owens BD. Epidemiology of Major League Baseball injuries. Am J Sports Med. 2011;39:1676–1680. [DOI] [PubMed] [Google Scholar]
- 15. Proske U, Morgan DL, Brockett CL, Percival P. Identifying athletes at risk of hamstring strains and how to protect them. Clin Exp Pharmacol Physiol. 2004;31:546–550. [DOI] [PubMed] [Google Scholar]
- 16. Schache AG, Wrigley TV, Baker R, Pandy MG. Biomechanical response to hamstring muscle strain injury. Gait Posture. 2009;29:332–338. [DOI] [PubMed] [Google Scholar]
- 17. Stanton P, Purdham C. Hamstring injuries in sprinting—the role of eccentric exercise. J Orthop Sports Phys Ther. 1989;10:343–349. [DOI] [PubMed] [Google Scholar]
- 18. Szymanski D. Recommendations for the avoidance of delayed-onset muscle soreness. Strength Cond J. 2001;23(4):7–13. [Google Scholar]
- 19. Thelen DG, Chumanov ES, Best TM, Swanson SC, Heiderscheit BC. Simulation of biceps femoris musculotendon mechanics during the swing phase of sprinting. Med Sci Sports Exerc. 2005;37:1931–1938. [DOI] [PubMed] [Google Scholar]