

Abstract
Background:
Anterior cruciate ligament (ACL) rupture is a significant injury in male National Hockey League (NHL) players.
Purpose:
To determine (1) the return to sport (RTS) rate in the NHL following ACL reconstruction, (2) performance on RTS, and (3) the difference in RTS and performance between players who underwent ACL reconstruction and controls.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
NHL players undergoing ACL reconstruction were evaluated. All demographic data were analyzed. Matched controls were selected from the NHL during the same years as those undergoing ACL reconstruction. The “index year” (relative to the number of years of experience in the NHL) in controls was the same as the year that cases underwent ACL reconstruction. RTS and performance in the NHL were analyzed and compared between cases and controls. Student t tests were performed for analysis of within- and between-group variables. Bonferroni correction was used in the setting of multiple comparisons.
Results:
A total of 36 players (37 knees) meeting the inclusion criteria underwent ACL reconstruction while in the NHL. Thirty-five players were able to RTS in the NHL (97%), and 1 player returned to the international Kontinental Hockey League. Of the players who RTS in the NHL, 100% were able to RTS the season after ACL reconstruction (mean, 7.8 ± 2.4 months). Length of career in the NHL after ACL reconstruction was 4.47 ± 3.3 years. The revision rate was 2.5%. There were significantly more cases playing in the NHL at 3 (P = .027) and 4 (P = .029) years following surgery compared with controls (index year). After ACL reconstruction, player performance was not significantly different from preinjury performance. Following ACL reconstruction (or index year in controls), cases played significantly more minutes, took more shots, had better shooting percentages, and scored more goals and points than did controls (P < .01 for all). Control players did not significantly outperform cases after ACL reconstruction in any performance measure.
Conclusion:
There is a high RTS rate in the NHL following ACL reconstruction. All players who RTS did so the season following surgery. Performance following ACL reconstruction was not significantly different from preinjury. Cases performed better than did controls in several performance measures. Controls did not outperform cases in any measured performance variable.
Keywords: anterior cruciate ligament, National Hockey League, return to sport, tear, knee injury
Anterior cruciate ligament (ACL) tears are one of the most common injuries in both contact and noncontact sports.5 Although the incidence of ACL tears in football and basketball players has been well identified,14 there have been no studies on the incidence of ACL tears in hockey players at any level. There is currently no reported incidence of ACL tears in athletes playing for the National Hockey League (NHL) in North America. It is estimated that there will be up to 200,000 ACL tears annually in the United States,3 more than half of which will be reconstructed surgically.7 ACL reconstruction is the standard of care in young athletes.
Although many studies report a high success rate following an ACL reconstruction,9 there are no data concerning NHL players and their return to sport (RTS) after ACL tear. Harris et al8 found an 86% RTS rate in NBA players after ACL reconstruction, while Erickson et al6 found a 77% RTS rate in Major League Soccer (MLS) players after ACL reconstruction. However, Ardern et al2 performed a systematic review of all athletes who underwent ACL reconstruction and found that while 82% RTS, only 63% RTS at their preinjury level. McCullough et al10 found similar results in high school– and college-level football players who underwent ACL reconstruction, in that 63% and 69%, respectively, RTS, while only 43% reported they were able to return to their preinjury level. With approximately 690 active NHL players, the popularity of the NHL has been growing over the past several years. This is evidenced by record total revenue for the NHL in each season from 2007 to 2011, with the highest revenue to date, US$2.9 billion, in 2011.13
The primary purposes of this study were to determine (1) RTS rate to the NHL following ACL reconstruction, (2) performance on RTS, and (3) the difference in RTS and performance between players who underwent ACL reconstruction and controls. The authors hypothesized that NHL players who sustained an ACL tear and underwent reconstruction will have (1) a >90% RTS rate; (2) no statistically significant difference in in-game performance parameters; and (3) no difference between age-, sex-, position-, and experience-matched control players.
Methods
Thirty-nine NHL players who tore their ACLs and underwent reconstructive surgery between 1990 and 2013 were identified. These players were discovered through NHL team websites, publicly available Internet-based injury reports, player profiles/biographies, and press releases. This method of player selection has been used in multiple publications in high-level evidence orthopaedic journals.1,4,6,8,11,12 The search was conducted by an orthopaedic surgery resident and a board-eligible orthopaedic surgeon in sports medicine fellowship training. All players who met the inclusion criteria were included in this study as it related to RTS rate. A player was deemed to have RTS if he played in any NHL game after surgery or if he is less than 12 months out from date of injury but is expected to RTS. A player did not RTS if he failed to meet any of the aforementioned criteria.
Only players who returned to the NHL and had played at least 1 full season were included in the pre- and postinjury in-game statistical analysis. After implementation of this criterion, 35 individual players remained whose pre- and postinjury in-game performance could be analyzed and compared (Figure 1). Of these 35 players, 1 player tore his reconstructed ACL 4 years after surgery and then returned the season after revision ACL reconstruction. Players were excluded if they tore both cruciate ligaments or if they tore 2 or more major knee ligaments (ACL, posterior cruciate ligament, medial collateral ligament, and lateral collateral ligament). No player was excluded based on concomitant injuries. Therefore, the total number of ACL tears analyzed in this portion of the study was 36.
Figure 1.

Flowchart of selection process for inclusive National Hockey League (NHL) players. ACL, anterior cruciate ligament.
Demographic data (age at injury, body mass index [BMI], position, months from injury to return to play, side of injury, period of the game in which the injury occurred, years played before and after the injury, and whether the player returned to the NHL the season after the injury) as well as average in-game performance data per season (games played, goals, assists, points, +/– goal differential, penalty minutes, even-strength goals, power play goals, short-handed goals, shots, shooting percentage, total time on ice, and average time on ice per game) were collected and analyzed. In-game performance variables were analyzed as an average over the pre- and postinjury course of the players’ careers. In addition, in-game performance variables were analyzed separately in each of the first 5 subsequent seasons the player returned to the NHL following the injury.
A control group was selected to compare the data with the case (ACL reconstruction) group. Controls were matched to cases based on sex, age, BMI, years of experience in the NHL, position, and all measured performance variables (Table 1). ACL reconstruction occurred at a mean of 6.61 ± 4.18 years into a player’s career. An “index year” was designated for controls, analogous to ACL reconstruction year in cases, as a matched reference year (relative to years experience in NHL) to compare post-ACL reconstruction or post–index year performance. Hence, if a player tore his ACL 4 years into his career, a control was selected with an index year of 4 years into his career. Demographic data (BMI, age, years in the NHL) and in-game performance data were collected and analyzed over the course of their careers before and after the index year (each season analyzed individually and collectively).
TABLE 1.
Comparison of Cases and Controls Before Anterior Cruciate Ligament Reconstruction (Index Year in Controls)a
| Cases | Controls | P Valueb | 95% CIc | |
|---|---|---|---|---|
| Age, y | 27.1 ± 4.05 | 27.1 ± 1.55 | .971 | –1.5 to 1.5 |
| Experience in NHL, y | 6.61 ± 4.18 | 6.61 ± 4.20 | .999 | –2.2 to 2.2 |
| Body mass index, kg/m2 | 27.1 ± 1.75 | 27.1 ± 1.19 | .924 | –0.61 to 0.68 |
| Games played per season, n | 391 ± 319 | 364 ± 276 | .696 | –113 to 168 |
| Goals per season, n | 12.9 ± 10.5 | 8.70 ± 8.70 | .068 | –0.33 to 8.8 |
| Assists per season, n | 17.7 ± 12.2 | 12.8 ± 11.3 | .081 | –0.62 to 10 |
| Points scored per season | 31.1 ± 22.0 | 21.6 ± 20.0 | .056 | –0.24 to 19 |
| +/– goal differential per seasond | 1.05 ± 6.08 | –0.236 ± 6.62 | .415 | –1.9 to 4.4 |
| Penalty time per season, min | 41.9 ± 30.4 | 40.7 ± 29.9 | .868 | –13 to 15 |
| Even-strength goals per season, n | 8.95 ± 6.09 | 6.88 ± 5.96 | .167 | –0.89 to 5.0 |
| Power play goals per season, n | 4.27 ± 3.83 | 2.41 ± 2.67 | .026 | 0.23 to 3.5 |
| Short-handed goals per season, n | 0.697 ± 0.840 | 0.640 ± 1.58 | .854 | –0.56 to 0.68 |
| Shots per season, n | 120 ± 63.0 | 91.4 ± 58.8 | .060 | –1.2 to 59 |
| Shooting percentage per season, % | 10.5 ± 5.50 | 8.92 ± 3.84 | .187 | –0.77 to 3.9 |
| Time on ice per season, min | 983 ± 421 | 861 ± 371 | .231 | –79 to 323 |
| Time on ice per game, min | 17.0 ± 3.90 | 14.5 ± 4.27 | .021 | 0.38 to 4.5 |
aValues are expressed as mean ± SD.
bPaired-samples Student t test with Bonferroni correction (statistical significance, P < .01).
c95% CI of the difference between cases and controls.
dA measure of how the player’s team did when he was on the ice. If the player has a positive number, more goals were scored by his team when he was on the ice than allowed; if he has a negative number, his team allowed more goals than they scored when he was on the ice.
Single-variable analyses for all continuous variables (performance measures) within groups were performed using paired-sample Student t tests. One-sample Kolmogorov-Smirnov goodness-of-fit tests for Gaussian data distribution were performed and confirmed normality of all data. Comparisons between case and control groups were made using Student t tests. Comparisons were made between cases and controls for survival in the NHL, each individual parameter’s overall mean (all years before and all years after ACL reconstruction [or index year]), and each individual year (up to 4 years) following ACL reconstruction (or index year in controls). Bonferroni correction was used to determine significance in the setting of multiple comparisons. Two-proportion Z tests with equal variance and α = 0.05 were used to compare left- versus right-hand shooters and left- versus right-side ACL tear distributions. All statistical analysis was performed using PASW Statistics student version 18.0.0.
Results
A total of 36 players (37 ACL tears) with ACL tears who underwent reconstruction between 1990 and 2013 met the inclusion criteria and were analyzed (Figure 1). Thirty-five players (36 knees) were able to RTS in the NHL (97% rate of RTS). However, the 1 player unable to return to NHL was able to successfully return to professional international hockey in the Kontinental Hockey League. Players returned to the NHL at a mean of 7.8 ± 2.4 months following ACL tear. Length of career in the NHL following ACL reconstruction up to and including the 2012-2013 season was 4.47 ± 3.33 years. One player of 36 underwent revision ACL reconstruction. Nineteen of these players (53%) remained active in the NHL. There were significantly more players in the NHL at years 2 and 3 after ACL reconstruction (vs index year in controls) (Figure 2). Left-handed shooters made up 68% of cases with ACL tears (P = .002; Z = 3.1), and 55% of ACL tears occurred in the right knee (P = .39; Z = 0.86). ACL tears by year are listed in Figure 3.
Figure 2.
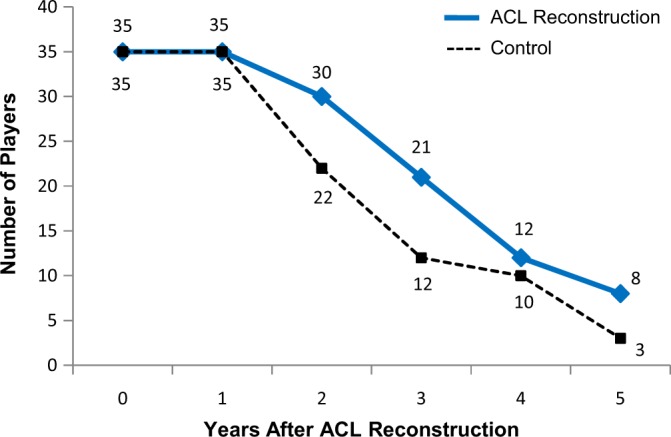
Survival curve. There was a significant difference in survival in the National Hockey League at years 2 (P = .0273; 95% CI, 0.0258-0.4342; Z = 2.21) and 3 (P = .0293; 95% CI, 0.0262-0.4938; Z = 2.18).
Figure 3.
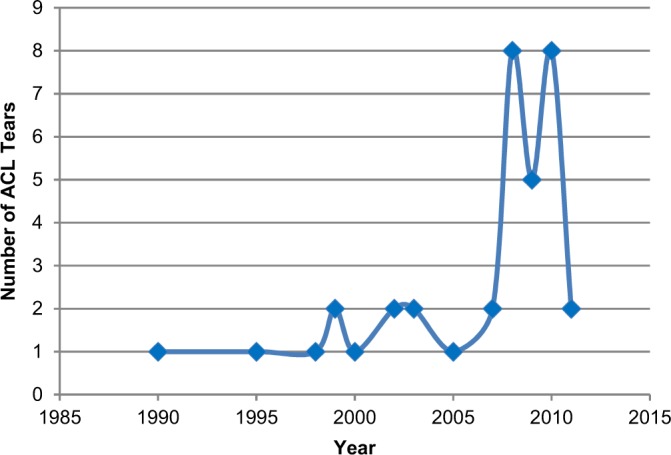
Anterior cruciate ligament (ACL) tears by year in National Hockey League players.
Prior to ACL reconstruction (or index year in controls), players who tore their ACLs and controls had no statistically significant differences in any demographic or performance variable (Table 1). After ACL reconstruction, NHL players who tore their ACLs performed significantly better (vs controls) in mean goals and points per season, mean power play and even-strength goals per season, and mean shots and shooting percentage per season (Table 2). Compared with preinjury, there were no significant differences in any performance measure in players who underwent ACL reconstruction (Table 3). Following the index year, controls played fewer games after their index season (Table 4). In years 3 and 4 after ACL reconstruction in cases (or index year in controls), the cases scored significantly more goals and had significantly more points than controls.
TABLE 2.
Comparison of Cases and Controls After Anterior Cruciate Ligament Reconstruction (Index Year in Controls)a
| Cases | Controls | P Valueb | 95% CIc | |
|---|---|---|---|---|
| Games played per season, n | 256 ± 234 | 217 ± 142 | .473 | –68 to 145 |
| Goals per season, n | 13.9 ± 13.2 | 6.82 ± 7.00 | .009 | 1.8 to 12 |
| Assists per season, n | 18.1 ± 12.6 | 11.7 ± 9.47 | .035 | 0.47 to 12 |
| Points scored per season | 32.5 ± 25.1 | 18.3 ± 15.7 | .009 | 3.7 to 25 |
| +/– goal differential per seasond | –0.265 ± 8.75 | –0.815 ± 4.59 | .761 | –3.1 to 4.2 |
| Penalty time per season, min | 41.0 ± 29.7 | 36.6 ± 24.8 | .550 | –10 to 19 |
| Even-strength goals per season, n | 10.3 ± 8.84 | 5.20 ± 4.82 | .007 | 1.5 to 8.8 |
| Power play goals per season, n | 4.43 ± 4.23 | 1.84 ± 2.14 | .004 | .86 to 4.3 |
| Short-handed goals per season, n | 0.487 ± 0.789 | 0.235 ± 0.308 | .104 | –0.05 to 0.56 |
| Shots per season, n | 138 ± 75.5 | 87.1 ± 52.0 | .007 | 14 to 87 |
| Shooting percentage per season, % | 9.94 ± 4.64 | 6.96 ± 3.35 | .007 | 0.84 to 5.1 |
| Time on ice per season, min | 1172 ± 437 | 860 ± 359 | .007 | 89 to 535 |
| Time on ice per game, min | 17.5 ± 4.11 | 14.6 ± 4.37 | .014 | 0.63 to 5.3 |
aValues are expressed as mean ± SD. Values in bold and italics indicate statistically significant differences between groups.
bPaired-samples Student t test with Bonferroni correction (statistical significance, P < .01).
c95% CI of the difference between cases and controls.
dA measure of how the player’s team did when he was on the ice. If the player has a positive number, more goals were scored by his team when he was on the ice than allowed; if he has a negative number, his team allowed more goals than they scored when he was on the ice.
TABLE 3.
Performance Comparison Before and After Anterior Cruciate Ligament Reconstruction (Cases)a
| Before | After | P Valueb | 95% CIc | |
|---|---|---|---|---|
| Goals per season, n | 12.9 ± 10.5 | 13.9 ± 13.2 | .733 | –6.6 to 4.6 |
| Assists per season, n | 17.7 ± 12.2 | 18.1 ± 12.6 | .904 | –6.2 to 5.5 |
| Points scored per season | 31.1 ± 22.0 | 32.5 ± 25.1 | .805 | –12 to 9.7 |
| +/– goal differential per seasond | 1.05 ± 6.08 | –0.265 ± 8.75 | .482 | –2.4 to 5.0 |
| Penalty time per season, min | 41.9 ± 30.4 | 41.0 ± 29.7 | .899 | –13 to 15 |
| Even-strength goals per season, n | 8.95 ± 6.09 | 10.3 ± 8.84 | .459 | –5.1 to 2.3 |
| Power play goals per season, n | 4.27 ± 3.83 | 4.43 ± 4.23 | .875 | –2.1 to 1.8 |
| Short-handed goals per season, n | 0.697 ± 0.840 | 0.487 ± 0.789 | .298 | –0.19 to 0.61 |
| Shots per season, n | 120 ± 63.0 | 138 ± 75.5 | .300 | –52 to 16 |
| Shooting percentage per season, % | 10.5 ± 5.50 | 9.94 ± 4.64 | .667 | –2.0 to 3.0 |
| Time on ice per season, min | 983 ± 421 | 1172 ± 437 | .088 | –407 to 29 |
| Time on ice per game, min | 17.0 ± 3.90 | 17.5 ± 4.11 | .599 | –2.6 to 1.5 |
aValues are expressed as mean ± SD.
bPaired-samples Student t test with Bonferroni correction (statistical significance, P < .01).
c95% CI of the difference between before and after values.
dA measure of how the player’s team did when he was on the ice. If the player has a positive number, more goals were scored by his team when he was on the ice than allowed; if he has a negative number, his team allowed more goals than they scored when he was on the ice.
TABLE 4.
Performance Comparison Before and After Index Season (Controls)a
| Before | After | P Valueb | 95% CIc | |
|---|---|---|---|---|
| Mean games played per season | 364 ± 276 | 217 ± 142 | .009 | 38 to 255 |
| Goals per season, n | 8.70 ± 8.70 | 6.82 ± 7.00 | .374 | –2.3 to 6.1 |
| Assists per season, n | 12.8 ± 11.3 | 11.7 ± 9.47 | .673 | –4.3 to 6.7 |
| Points scored per season | 21.6 ± 19.6 | 18.3 ± 15.7 | .497 | –6.2 to 13 |
| +/– goal differential per seasond | –0.236 ± 6.62 | –0.815 ± 4.59 | .718 | –2.6 to 3.8 |
| Penalty time per season, min | 40.7 ± 29.9 | 36.6 ± 24.8 | .577 | –10 to 19 |
| Even-strength goals per season, n | 6.88 ± 5.96 | 5.20 ± 4.82 | .269 | –1.3 to 4.7 |
| Power play goals per season, n | 2.41 ± 2.67 | 1.84 ± 2.14 | .400 | –0.78 to 1.9 |
| Short-handed goals per season, n | 0.640 ± 1.58 | 0.235 ± 0.308 | .231 | –0.26 to 1.1 |
| Shots per season, n | 91.4 ± 58.8 | 87.1 ± 52.0 | .782 | –26 to 35 |
| Shooting percentage per season, % | 8.92 ± 3.84 | 6.96 ± 3.35 | .053 | –0.03 to 3.9 |
| Time on ice per season, min | 861 ± 371 | 860 ± 359 | .995 | –200 to 201 |
| Time on ice per game, min | 14.5 ± 4.27 | 14.6 ± 4.37 | .966 | –2.4 to 2.3 |
aValues are expressed as mean ± SD. Values in bold and italics indicate statistically significant differences between groups.
bPaired-samples Student t test with Bonferroni correction (statistical significance, P < .01).
c95% CI of the difference between before and after values.
dA measure of how the player’s team did when he was on the ice. If the player has a positive number, more goals were scored by his team when he was on the ice than allowed; if he has a negative number, his team allowed more goals than they scored when he was on the ice.
Discussion
The study hypotheses were confirmed, as there was a 97% rate of RTS in NHL players, with no statistically significant difference in in-game performance parameters from preinjury to postsurgery and improvement in several in-game performance measures compared with controls.
Two separate case-control studies performed at the authors’ institution6,9 examined RTS and performance in 64 National Basketball Association (NBA) players and 52 MLS players. Those studies demonstrated a lower return to high-level sports (86% to the NBA and all but 1 player [98%] returned to any level of competitive professional basketball, while there was a 77% rate of RTS to MLS) than the current study (97% RTS in NHL). It is unclear exactly what factors play a role in the ability or inability of a professional athlete to RTS after an ACL reconstruction. The demands of each sport, as well as the forces seen by the knees, vary, and because of this, future kinetic and kinematic studies comparing the stresses placed on the knee during various professional sports are necessary to determine if there is a way to improve the RTS rate of these athletes.
The current study demonstrated a revision rate of only 2.5% (1/37 ACL reconstructions needed to be revised), while the NBA and MLS studies demonstrated revision rates of 3.1% and 10%, respectively. This is an interesting finding, as many ACL tears in NHL athletes are likely contact injuries because there is no significant jumping involved in hockey and players cleats do not get caught in the ground (in MLS and the NBA, these injuries are often noncontact). This mechanism of injury may predispose these athletes to higher revision rates on RTS, as ACL reconstructions can more reliably withstand contact injuries than noncontact injuries. This begs the question of whether improved proprioceptive training could lead to a decrease in these revision rates in noncontact injuries of MLS and the NBA.
The NBA study showed a significant decline in games played per season versus controls following ACL reconstruction (or index year in controls), while the current study showed no difference in games played between cases and controls. The MLS study, like the current study, did not demonstrate a decline in any in-game performance parameter. Thus, among players in the NBA, MLS, and NHL, those who sustain an ACL tear in the NHL perform the best and have the highest RTS rate after reconstruction. This is a very significant finding for current and future professional NHL players, as an ACL tear does not signify the end of a player’s career, and players can expect to return to their preinjury level of competition. Interestingly, there seemed to be a trend toward an increase in the number of ACL tears in NHL players between 2007 and 2010, although this did not reach statistical significance. As there were no rule changes or other explanations that could have accounted for this spike, it is likely due to chance.
Unlike ACL tears in elite football, soccer, and basketball players, which have been extensively studied,6,9,10 the authors could find no studies to date that have looked at the RTS rate or the performance on RTS in the NHL or other elite-level hockey players. Furthermore, there have not been any studies that evaluated the risk of ACL tear in NHL players. The current study identified 40 ACL tears over a 13-year period, giving an incidence of roughly 3 ACL tears per year in NHL players.
The NHL players reviewed in this study who underwent ACL reconstruction did not see either a decline or improvement in their performance after surgery. This is a reassuring finding as surgeons would not expect to find an improvement in performance after surgery but rather hope to prevent a decline in performance. Also, despite the fact that the NHL players who underwent ACL reconstruction performed better than the control group in some performance variables after surgery, this statistic may be construed as players who have ACL reconstruction do better than those who do not. The players who had ACL reconstruction may have been more elite athletes to begin with and had not had a chance to fully develop prior to their injury. Also, in their recovery period after surgery, they are spared the rigors of playing in game situations, and so when they did return from their injury, their bodies were rested and primed for competition.
A unique finding in the current investigation is that a greater number (68%) of ACL tears in NHL players occurred in left-handed shooters (P = .002), while the number of tears in right versus left knees did not significantly differ (55% vs 45%; P = .39). In the previously reported NBA player case-control study, the side distribution (right vs left) was nearly identical to the current study (51% vs 49%, respectively), while that of the MLS was significantly different, with 68% of tears occurring in the left knee. The exact etiology of this significant increase in tears in left-handed shooters is not clear at this time. It may take origin in shooting mechanics, but without a biomechanical study to verify this, this is simply an observation.
Limitations
The strengths of this study include its case-matched control comparative design and use of sport-specific performance parameters. Limitations include the use of publicly available data, which can be subject to observer bias because of anticipated media and/or public scrutiny. There is the possibility that some cases were missed and that these players did not do well after their ACL reconstructions, thereby leading to a falsely high RTS rate. However, the opposite is also true, in which players who had a successful ACL reconstruction were missed but went on to play well, which would have falsely lowered the RTS rate. Nevertheless, this method of subject selection has been utilized in multiple high–evidence level studies in sports medicine journals.1,4,6,9,11,12 Another limitation was that no subject patient-reported or clinician-measured outcomes were available; this includes general health (eg, Short Form–36) and joint-specific (eg, Knee Society Score [KSS]). Furthermore, postinjury patient satisfaction and personal perception of knee pain, function, and stability versus preinjury were unable to be assessed. These factors may influence RTS performance. Surgical technique information was unobtainable from publicly available sources, although it can be inferred by the treating surgeon based on preferences expressed in publications and/or presentations. Because of the high-profile nature of these athletes, they are unable to be easily contacted to assess these outcome measures. Additionally, the rehabilitation program utilized postoperatively was unavailable. Even though only 1 player was unable to return to play in the NHL following ACL reconstruction, the inability to return cannot solely be attributed to ACL injury and surgery, as other confounders inevitably coexist. Furthermore, although all performance-based measures were used to compare pre- and postoperative outcomes and between cases and controls, other intangibles (team leadership, teammate motivation, etc) cannot be assessed for relationships.
Conclusion
There is a high RTS rate in the NHL after ACL reconstruction. All players who RTS did so the season following surgery. Performance following ACL reconstruction was not significantly different from preinjury. Cases performed better than controls in several performance measures.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: B.J.C. is a consultant for Zimmer, Arthrex, Carticept, Biomimetic, Allosource, and DePuy; receives speaking fees from Genzyme; receives royalties from Arthex, DJO, and Elsevier; and receives research funding from Regentis, Arthrex, Smith & Nephew, DJO, Zimmer, DePuy, and Johnson & Johnson. B.R.B. receives publishing royalties from Slack Inc. N.N.V. is a consultant for Arthrex and Smith & Nephew; receives speaking fees from Arthrosurface; receives royalties from Smith & Nephew, Vindico Medical-Orthpedics Hyperguide, and Arthroscopy; and holds stock in Omeros.
References
- 1. Amin NH, Old AB, Tabb LP, Garg R, Toossi N, Cerynik DL. Performance outcomes after repair of complete Achilles tendon ruptures in National Basketball Association players. Am J Sports Med. 2013;41:1864–1868. [DOI] [PubMed] [Google Scholar]
- 2. Ardern CL, Webster KE, Taylor NF, Feller JA. Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and meta-analysis of the state of play. Br J Sports Med. 2011;45:596–606. [DOI] [PubMed] [Google Scholar]
- 3. Arendt EA, American Orthopaedic Society for Sports Medicine, American Academy of Orthopaedic Surgeons OKU Orthopaedic Knowledge Update. Sports Medicine 3. 3rd ed Rosemont, IL: American Academy of Orthopaedic Surgeons; 2004. [Google Scholar]
- 4. Cerynik DL, Lewullis GE, Joves BC, Palmer MP, Tom JA. Outcomes of microfracture in professional basketball players. Knee Surg Sports Traumatol Arthrosc. 2009;17:1135–1139. [DOI] [PubMed] [Google Scholar]
- 5. DeHaven KE, Lintner DM. Athletic injuries: comparison by age, sport, and gender. Am J Sports Med. 1986;14:218–224. [DOI] [PubMed] [Google Scholar]
- 6. Erickson BJ, Harris DJ, Cvetanovich GL, et al. Performance and return-to-sport after anterior cruciate ligament reconstruction in male Major League Soccer players. Orthop J Sports Med. 2013;1 (2) doi:10.1177/2325967113497189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Frank CB, Jackson DW. The science of reconstruction of the anterior cruciate ligament. J Bone Joint Surg Am. 1997;79:1556–1576. [DOI] [PubMed] [Google Scholar]
- 8. Harris JD, Erickson BJ, Bach BR, Jr, et al. Return-to-sport and performance after anterior cruciate ligament reconstruction in National Basketball Association players. Sports Health. 2013;5:562–568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Lohmander LS, Englund PM, Dahl LL, Roos EM. The long-term consequence of anterior cruciate ligament and meniscus injuries: osteoarthritis. Am J Sports Med. 2007;35:1756–1769. [DOI] [PubMed] [Google Scholar]
- 10. McCullough KA, Phelps KD, Spindler KP, et al. Return to high school- and college-level football after anterior cruciate ligament reconstruction: a Multicenter Orthopaedic Outcomes Network (MOON) cohort study. Am J Sports Med. 2012;40:2523–2529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Namdari S, Baldwin K, Anakwenze O, Park MJ, Huffman GR, Sennett BJ. Results and performance after microfracture in National Basketball Association athletes. Am J Sports Med. 2009;37:943–948. [DOI] [PubMed] [Google Scholar]
- 12. Namdari S, Scott K, Milby A, Baldwin K, Lee GC. Athletic performance after ACL reconstruction in the Women’s National Basketball Association. Phys Sportsmed. 2011;39:36–41. [DOI] [PubMed] [Google Scholar]
- 13. NHL.com. Best-ever business year highlighted by record revenue. 2011. http://www.nhl.com/ice/news.htm?id=559630. Accessed August 12, 2014.
- 14. Prodromos CC, Han Y, Rogowski J, Joyce B, Shi K. A meta-analysis of the incidence of anterior cruciate ligament tears as a function of gender, sport, and a knee injury-reduction regimen. Arthroscopy. 2007;23:1320.e6–1325.e6. [DOI] [PubMed] [Google Scholar]