

Abstract
Healthy teeth and gums make a person feel confident and fit. As people go about their daily routines and with different eating and drinking habits, the tooth enamel turns yellowish or gets stained. Polishing traditionally has been associated with the prophylaxis procedure in most dental practices, which patients know and expect. However, with overzealous use of polishing procedure, there is wearing of the superficial tooth structure. This would lead to more accumulation of local deposits. Also, it takes a long time for the formation of the fluoride-rich layer of the tooth again. Hence, now-a-days, polishing is not advised as a part of routine oral prophylaxis procedure but is done selectively based on the patients’ need. The article here, gives an insight on the different aspects of the polishing process along with the different methods and agents used for the same.
Keywords: Abrasives, mechanical aids, polishing, tooth staining
INTRODUCTION
Tooth polishing is a procedure carried out as a part of oral prophylaxis in most dental practices. It is an act of smoothening the tooth surfaces to make it glossy and lustrous. Although the term polishing has been used to describe the professional removal of soft deposits and stains from the tooth surfaces, in reality, this includes both cleaning and polishing.[1] During polishing, plaque, biofilm, stains and acquired pellicle are removed.
It is important to understand the patients’ expectations when considering tooth polishing. They simply like the look and feel of polished teeth. Taste and smell are the next important factors from the patient's point of view. Patients prefer this procedure over debridement with instruments for many reasons. An important factor is that patients respond positively to the smooth and clean feel that polishing produces. Furthermore, it is less painful and stressful than scaling; and easier for the patient to understand and tolerate. Polishing produces tangible benefits, which the patients can see and feel.
Though, the history of tooth polishing was mentioned in the Roman and Greek writings, it was only with Pierre Fauchard, the Father of Modern Dentistry, who introduced it for removal of dental stains with the use of finely ground coral, egg shells, ginger, or salt.[2] The techniques and modalities for tooth polishing have evolved over the years. Dr. Fones, the Founder of Dental Hygiene, started training his auxiliaries to provide coronal tooth polishing in the last century. It was observed that stains were not the etiologic factor for any destructive process and hence, removal of stains was for esthetic, not for health reason.[3] Hence, polishing was then used as a selective process by Wilkins.[3] Before 1970s, patients expected polishing as a necessary part of the dental appointment.[4] During the 1990s and 2000s, further evidence has supported the adoption of selective polishing.[5] However, the concept of full mouth polishing is still used in many – if not most – dental hygiene practices. But worldwide, many dental hygiene schools now recommend selective polishing as a standard protocol instead of including polishing at every professional maintenance appointment.
Several terms are being used in relation to the practice of cleansing and polishing teeth. However, when oral health professionals use the word “polishing,” they are typically referring to the dual process known as “cleaning” and “polishing.” The American Dental Hygienists Association position paper on polishing procedures sufficiently distinguishes between these closely related terms-defining “cleansing” as “the ability to remove debris and extraneous matter from the teeth,” and “polishing” as “the implementation of making the tooth surface smooth and lustrous.” The American Academy of Periodontology defines tooth polishing (in relation to oral prophylaxis) as “the removal of plaque, calculus and stains from the exposed and unexposed surfaces of the teeth by scaling and polishing as a preventive measure for the control of local irritational factors.”[6,7]
Other terms, which are commonly used are:
Therapeutic polishing - Refers to “the polishing of the root surfaces that are exposed during surgery to reduce endotoxin and microflora on the cementum.”[7]
Coronal or cosmetic polishing - Is defined as “a procedure designed to make the tooth free of plaque and extrinsic stains.”[7] The process of achieving a smooth, mirror-like enamel or material surface that reflects light and is characterized as having a high luster; accomplished with a fine to extra fine grit abrasive agent so that the surface scratches are smaller than the wavelength of visible light (<0.05 μm). The term coronal polishing may also encompass cleansing.[7]
Superficial polishing - it is a term related to the polishing of the crown of the tooth. It is now considered as a cosmetic procedure with minimal therapeutic benefit.
Selective polishing - is another word often used by hygienists. It is used to indicate that cleansing and polishing procedures are only provided when justified by the tooth surfaces that have visible stains after scaling, and oral debridement is complete. Selective polishing is also known as extrinsic stain removal or selective stain removal. The most accurate term for all of these procedures is selective stain removal, which indicates the removal of extrinsic stains after professional scaling, using a rubber cup, bristle brush, and/or an air-powder polishing system; though everything depends on the assessed needs of the patient. It means cleansing and polishing are omitted on surfaces already stain free.[7]
Today the focus of tooth polishing is to give a highly polished and aesthetic appearance by removing bacterial plaque biofilms and extrinsic stains. But before we do polishing, one needs to identify the type of stains and also understand the contraindications for tooth polishing.
Identifying stain
It is very important to identify the type of stain so as to determine which stains can be removed and which product to use. Stains can be broadly classified into-endogenous and exogenous stains. Endogenous stains can be further divided into developmental, drug induced, environmental or due to enamel hypoplasia. The exogenous stains are due to various foods and harmful habits and are usually seen as different colors: Green, orange, brown and black. The endogenous stains cannot be removed by simple polishing. However, the exogenous stains can be removed by scaling and polishing.
Contraindications for use of oral prophylaxis polishing paste[8,9]
Absence of extrinsic stains
Acute gingival and periodontal infection
Esthetic restorations
Allergy to paste ingredients
Dental caries
Decalcification
Enamel hypoplasia
Exposed dentin or cementum
Hypomineralization
Newly erupted teeth
Patients with respiratory problems
Recessions
Tooth sensitivity
Xerostomia.
During the process of tooth polishing, following things have to be taken care of:
Use proper technique to reduce unnecessary abrasion on the exposed enamel and dentine surfaces
Select a least abrasive polishing agent that will remove plaque biofilm and stain
Control the time, speed and pressure during the procedure
When polishing a restorative material, care has to be taken to use a softer abrasive particle than the restorative material.[1]
CHOOSING A PROPHYLAXIS PASTE
As prophylaxis paste can cause incidental damage while removing the dental stains, they should be chosen carefully. Those with a larger particle size, that is, coarse or medium, are very effective in extrinsic stain removal, but they can also cause the most abrasion and damage to the tooth surface. In fact, excessive abrasion scratches the enamel, resulting in a less polished appearance and ultimately, contributing to an increased rate of exogenous stain reformation and bacterial plaque retention.[4] In contrast, prophylaxis paste with a smaller particle size, such as those found in fine paste, will increase tooth surface cleanliness, luster and smoothness, making the surface more resistant to subsequent stain, plaque and calculus formation.[4] Some professionals consider polishing with fine prophylaxis paste to be less effective as they have to apply more pressure and invest more time to remove the same stains than when using coarse prophylaxis pastes.
The factors that contribute to the overall efficiency of stain removal from the tooth surfaces include:
Rotations per minute (rpm) of the rubber cup polisher
Prophy paste coarseness
Rubber cup-to-tooth pressure or load, and
The time spent polishing each stained area.[10]
Unfortunately, each of these factors contributes directly to the tooth enamel and dentin damage via abrasion.
ABRASIVE AGENTS
The purpose of the abrasive agent is to clean and to make the tooth surfaces smooth. The abrasive agents present in the polishing paste are usually the same as those in dentifrices. However, the major difference being the particle size of the abrasive; where the size is more in professional prophylaxis pastes as compared to dentifrices. Prophylaxis polishing pastes available in the market usually combine abrasives with a binder, humectants, coloring agent, preservative, and flavoring agent.[3] They are available in varying sizes of abrasive particles, ranging from coarse, medium to fine. Harder, rough-shaped, large, particle size compounds produce more abrasive action than particles that are soft, smooth-shaped and small.
The most commonly used abrasives in polishing pastes are flour of pumice and calcium carbonate. Other abrasive particles used in commercial prophylaxis polishing pastes include aluminum oxide (alumina), silicon carbide, aluminum silicate, silicon dioxide, carbide compounds, garnet, feldspar, zirconium silicate, zirconium oxide, boron, and calcium carbonate. Others include the emery, silica, and perlite.
Pumice is a light gray, highly siliceous material produced by volcanic activity. The flour of pumice is a very finely grounded derivative which is used for polishing of tooth enamel, gold foil, dental amalgam and acrylic resins.[11] Calcium carbonate, commonly known as chalk is less abrasive then pumice. It produces minimal scratches and results in a highly reflective surface.[1] Zirconium silicate is also used for polishing and is available as an off-white mineral on abrasive disks and strips. However, it is frequently used as a component of dental prophylaxis paste. Manufacturers generally do not disclose the amount of ingredients in their polishing pastes. However, it is generally known that pumice and glycerin are the most commonly used ingredients in commercially prepared polishing pastes. Some commercially prepared polishing pastes may contain fluorides, while some may have added advantages [Table 1].
Table 1.
Some ready-to-use prophy pastes are
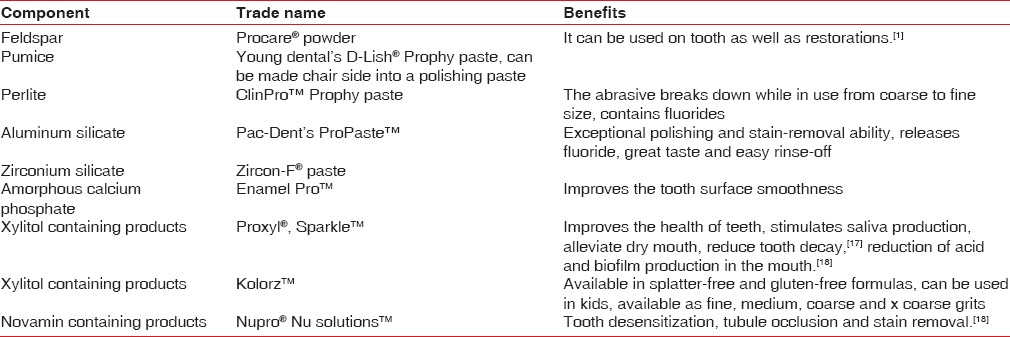
Pumice flour has been tested for its effectiveness in stain removal on enamel. The mean abrasive depth of enamel with pumice flour is significant (12.1 μm on a scale ranging from 15.6 μm to 1 μm) and it has an average polishing score when compared with other agents like Nupro Fine, Procare, Zircate, etc.[12] Calcium carbonate produces minimal scratches and results in a smooth, polished surface.[13] Very few agents are available which initially function as cleansing agent and then alters to become a polishing agent e.g., cleanic and zircate. These abrasives have been compared to conventional abrasive agents. Lutz et al.[14] in 1993 reported that all the three ideal requirements of a polishing paste, that is, good cleansing ability, minimal abrasion, and simultaneous polishing, which are fulfilled by perilite containing polishing paste. Similarly, it was reported that a paste containing perlite can polish teeth by removing surface stains without causing damage to either the tooth structure or to the soft tissues.[15]
The process of polishing has to proceed from coarse abrasion (cleaning) to fine abrasion (polishing), with the use of a series of finer and finer abrasives. Fine grit is used routinely; medium or coarse pastes are only needed in situations of heavy stain. As the polishing process proceeds from coarse to fine abrasion, scratches smaller than 0.5 mcm are produced. These scratches appear smooth and shiny as they are smaller than the wavelength of visible light.[1] Even then, the degree of abrasiveness is dependent on clinicians’ technique and tooth surface integrity.[13]
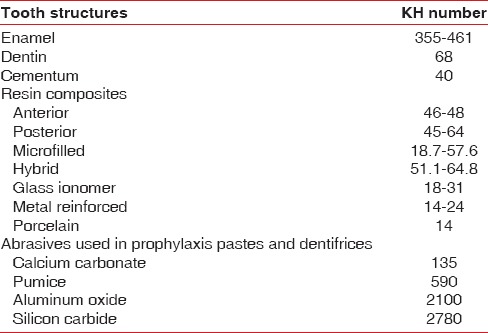
A single polishing agent cannot be used for all surfaces like tooth enamel, root surfaces or restorations, as they all have different hardness values. A polishing agent should be selected on the basis of their hardness in such a way that the hardness of the polishing agent should be less than that of the surface to be polished [Table 2]. However, many of the abrasives used in prophylaxis pastes are 10 times (or more) harder than the surfaces they are used to polish.[1]
Table 2.
Knoop hardness values[1]
MECHANICAL DEVICES FOR POLISHING
Different polishers are available: Manual and engine driven. The manual polishers are hand-held devices whereas; the engine driven uses hand pieces to do polishing. The most commonly used method of tooth polishing is with the use of a mechanical device along with the polishing agent.
Many polishers available are:
Porte polisher
It is a hand-held device with an orange-wood point. This instrument can be used on various aspects of teeth. It rubs the abrasive agent against the tooth surface with a wedge-shaped, tapered, or pointed wooden point.[1]
Advantages
Portable
Can be accessible to malpositioned tooth surfaces
Generates minimal thermal heat
Does not produce noise like rotary instruments
Minimal bacterial aerosol.[1]
Drawbacks
It requires more hand strength for instrumentation and takes a longer time for polishing teeth.[16]
Polishing strips
They are a good option for interproximal areas and line angles. However, they are highly abrasive. Care has to be taken to avoid cutting or abrading the surrounding soft tissues during polishing.[16]
Engine-driven polishers
These are widely used amongst dental professionals and dental hygienists for their efficiency and efficacy. These polishers are attached to the appropriate hand piece or prophy-angle, which has either straight or contra-angled shanks. They can be either disposable or reusable after sterilization. A rubber cup or brush is attached to the prophy-angle. The handpiece should always be used at a steady slow pace of 2500–3000 rpm.[16] Christensen and Bangerter reported in an in vivo clinical study that the average speed used by dental hygienists was 2500 rpm.[10] Because it is difficult to estimate the rpm in clinical practice, the slow speed handpiece is always rotated at the lowest rpm possible. The rpm is too great if “whining” or high pitched sound occurs.[13] Most of the surfaces can be polished in 2–5 s with the use of a light, steady speed in a patting motion. Christensen and Bangerter identified that the rubber cup contacted each tooth surface for an average of 4.5 s.[10] It was reported by Miller and Hodges that it took 10 min (3.4 s per tooth) to treat the entire mouth when standardizing polishing time in a research study comparing rubber cup and air-polishing.[13] The pressure applied should be approximately 20 psi.[1] When a rubber cup does not adequately remove occlusal stains, a brush should be used taking care not to traumatize the soft tissue as they are difficult to control.
Indications
They can be used in most clinical applications as patient compliance and acceptance are high.
Contraindications
In patients having allergies to latex or fluorides; rubber-cup latex free products, prophy pastes and pumice slurry without fluoride should be used.
Air-powder polisher
Nowadays, air powder polishing devices have overcome conventional rubber cup polishing paste systems for supragingival plaque removal as it reaches surfaces that are inaccessible to a rotary device.[19,20] These polishers use slurry of water and sodium bicarbonate under air and water pressure. Abrasives like aluminum trihydroxide, calcium sodium phosphosilicate, calcium carbonate and glycine are also used in air polishers.
The air powder polisher handpiece attaches either directly to the air/water connector on the dental unit or as a separate unit or in combination with ultrasonic scalers. By activating the foot control, the handpiece nozzle would propel the slurry on the tooth surface. The nozzle should be held 3–4 mm from the tooth surface. Holding the nozzle farther from the tooth surface minimizes the abrasive action and increases the aerosol. The tip should be angled diagonally, with the spray directed towards the middle one third of the exposed tooth, using a constant circular motion, interproximal to interproximal sweeping or paint brush motion.[1] For anterior teeth, the tip should be directed at a 60° angle; for posterior teeth, 80° angle and for occlusal surfaces a 90° angle is appropriate.[1] Most of the equipment are operated using inlet air pressure between 40 and 100 psi and inlet water pressure between 20 and 60 psi.[3] However, Francis and Barnes mention that the psi produced depends on the type of air powder polisher being used.[1] These are usually safe to use and effective methods for extrinsic stain removal and plaque removal. However, studies have reported that exposed cementum and dentin structures are vulnerable to loss with the use of air powder polisher.[21,22] By adjusting the amount of water flow and the distance of the instrument to the tooth, the abrasive forces can be reduced. Petersilka et al. has noted that by changing the physical properties of air-polishing agents, the abrasive effects on the root surfaces can be reduced along with complete removal of extrinsic stains.[23]
Earlier, air dent machine which uses alumina or dolomite was used. However, currently the redesigned air-polishing device (APD), the prophy-jet, which uses a pressurized slurry of sodium bicarbonate with tri-calcium phosphate (added up to 0.8% of weight to improve flow characteristics) in warm water on to the tooth surface, at a suggested distance of 4–5 mm and angulations of around 60° is used.[22] Powder-water setting, the distance of the jet from the treated surface and the shape and size of the particles used, control the effectiveness of the device.[20] APD is an effective means for removal of plaque from orthodontically bracketed teeth as it does not disturb the wires or rubber bands and also is not detrimental to the zinc phosphate or resin cement which are used to attach brackets and bands.
Advantages
It minimizes the operator and patient fatigue.
It is time saving and effective.
Dentinal sensitivity is diminished following the use of prophy-jet, which may be explained by the fact that bicarbonate crystals may block the tubular opening
It removes plaque from areas that are otherwise difficult to reach like furcations, flutings and close root proximities.[19]
Disadvantages
They should be cautiously used in patients with restricted sodium diets, respiratory, renal or metabolic disease, infectious disease, children, diuretics or long term steroid therapy, and those having titanium implants. Owing to the limitation of prophy-jet in individuals with sodium restricted diets, nonsodium prophy powder, containing aluminum trihydroxide (cavitron, jet-fresh) instead of sodium bicarbonate can be used
Another drawback is the aerosols generated by air-polishing may present an infection control hazard. Hence, a preprocedural rinse is always recommended along with aerosol reduction devices. Subcutaneous emphysema can also occur whenever compressed air is employed intra-orally. This highlights the iatrogenic potential and reinforces the need to follow manufacturer's instructions appropriately.[19]
Recent introduction of glycine powder air-polishing in removing sub-gingival biofilm abridge periodic sub-gingival instrumentation and serve as an alternative to conventional techniques that result in less gingival erosion along with 80% reduction in abrasiveness on root surface than hand instrumentation or sodium bicarbonate air-polishing.[24]
Comparison of rubber cup polishing and air-polishing methods
Result of studies comparing the effectiveness of air-polishing to the rubber cup polishing for bacterial plaque and stain removal demonstrate that either method is equally effective.[25] They reported that both methods caused some gingival trauma.[25] However, Garcia-Godoy and Medlock have reported air polishers to be more effective for plaque and stain removal in pits and fissures.[26]
Vector system
The vector system uses a polishing fluid to polish the teeth. It removes plaque and endotoxin with minimal removal of the cementum surface. Braun et al. demonstrated the use of a polishing fluid containing hydroxyapatite or an abrasive fluid containing silicon carbide which has a resonating device that deflects vibrations directed toward the tooth surface, thereby minimizing the forces that remove tooth substance. Thus, less force is directed at the tooth surface as fluid dynamics removes the plaque. This can provide effective control of inflammation after thorough debridement of calculus and before new deposits of calculus begin to form.[27]
EVALUATION OF COMPLETION OF POLISHING PROCEDURE
At the end of polishing procedure, the teeth have to be inspected thoroughly using a mouth mirror, intra-oral light, compressed air and disclosing solution.[1] Remaining biofilm or stains has to be removed by either re-instrumentation or re-polishing the surface. Finishing strips or dental tape rubbed with a small amount of prophy paste before flossing assists in the removal of residual interproximal stains.[1]
CONCLUSION
Tooth polishing used to be a standard part of a dental cleaning appointment. The dentists used to smoothen teeth so that plaque and bacteria which cause gingivitis, periodontitis or cavities do not stick to the tooth easily. However, it is now known that within 30 min, the bacteria colonize on the tooth surface irrespective of whether teeth are polished or not. Also, polishing removes the outer layer of tooth enamel, which takes a period of 3 months to rebuild the fluoride-rich layer. Hence, selective polishing is recommended. Each patient should be assessed individually for polishing of teeth. Teeth are polished only if stains are present which scaling was unable to remove. This means that during cleaning procedures either some, all or none of the teeth may be polished.
Currently, the dentists and hygienists have varied options regarding the abrasive/polishing agents and type of polishers used. They can now use different polishers and abrasives based on the patients’ acceptance and condition, thereby providing good care by selectively designing the treatment according to the patients’ need and with minimum concern about the loss of tooth structure.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Francis B, Barnes CM. Cosmetic and therapeutic polishing. In: Daniel SJ, Harfst SA, Wilder R, editors. Mosby's Dental Hygiene: Concepts, Cases and Competencies. Missouri: Elsevier; 2008. pp. 599–622. [Google Scholar]
- 2.Ring ME. History of dental prophylaxis. J Am Dent Assoc. 1967;75:892–5. doi: 10.14219/jada.archive.1967.0306. [DOI] [PubMed] [Google Scholar]
- 3.Barnes CM. Extrinsic stain removal. In: Wilkins EW, editor. Clinical Practice of the Dental Hygienist. Philadelphia: Lippincott Williams and Wilkins; 2009. pp. 724–40. [Google Scholar]
- 4.Putt MS, Kleber CJ, Muhler JC. Enamel polish and abrasion by prophylaxis pastes. Dent Hyg (Chic) 1982;56:38–40-3. [PubMed] [Google Scholar]
- 5.Redford-Badwal DA, Nainar SM. Assessment of evidence-based dental prophylaxis education in postdoctoral pediatric dentistry programs. J Dent Educ. 2002;66:1044–8. [PubMed] [Google Scholar]
- 6.4th ed. Chicago: American Academy of Periodontology; 2001. American Academy of Periodontology. Glossary of Periodontal Terms; p. 42. [Google Scholar]
- 7. [Last accessed on 2014 Aug 12]. Available from: http://www.aaoshconnect.org/issue/julyaug-2012/article/an-evidence-based-approach-to-cleansing-andpolishing-teeth .
- 8.Atkinson DR, Cobb CM, Killoy WJ. The effect of an air-powder abrasive system on in vitro root surfaces. J Periodontol. 1984;55:13–8. doi: 10.1902/jop.1984.55.1.13. [DOI] [PubMed] [Google Scholar]
- 9.Augthun M, Tinschert J, Huber A. In vitro studies on the effect of cleaning methods on different implant surfaces. J Periodontol. 1998;69:857–64. doi: 10.1902/jop.1998.69.8.857. [DOI] [PubMed] [Google Scholar]
- 10.Christensen RP, Bangerter VW. Determination of rpm, time, and load used in oral prophylaxis polishing in vivo. J Dent Res. 1984;63:1376–82. doi: 10.1177/00220345840630120701. [DOI] [PubMed] [Google Scholar]
- 11.Trade news – New toothpaste. Br Dent J. 2003;195:112. [Google Scholar]
- 12.Putt MS, Kleber CJ, Muhler JC. Enamel polish and abrasion by prophylaxis pastes. Dent Hyg (Chic) 1982;56(38):40–3. Retraction in: Hodges K, editor Concepts in Nonsurgical Periodontal Therapy. 1st ed. New York: Delmar; 1998. p. 345-66. [PubMed] [Google Scholar]
- 13.Hodges K, editor. New York: Delmar; 1998. Concepts in Nonsurgical Periodontal Therapy; pp. 345–66. [Google Scholar]
- 14.Lutz F, Sener B, Imfeld T, Barbakow F, Schüpbach P. Self-adjusting abrasiveness: A new technology for prophylaxis pastes. Quintessence Int. 1993;24:53–63. [PubMed] [Google Scholar]
- 15.Anusavice KJ, Antonson SA. Finishing and polishing materials. In: Anusavice KJ, editor. Phillips’ Science of Dental Materials. St. Louis: Elsevier Science; 2003. pp. 351–77. [Google Scholar]
- 16.Rethman J. Polishing angles, cups and pastes. Pract Hyg. 1997;1:32–9. Retraction in: Madan C, Bains R, Bains VK. Tooth polishing: Relevance in present day periodontal practice. J Indian Soc Periodontol 2009;13:58-9. [Google Scholar]
- 17.Madan C, Bains R, Bains VK. Tooth polishing: Relevance in present day periodontal practice. J Indian Soc Periodontol. 2009;13:58–9. doi: 10.4103/0972-124X.51899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Petersilka GJ, Ehmke B, Flemmig TF. Antimicrobial effects of mechanical debridement. Periodontol 2000. 2002;28:56–71. doi: 10.1034/j.1600-0757.2002.280103.x. [DOI] [PubMed] [Google Scholar]
- 19.Boyde A. Airpolishing effects on enamel, dentine, cement and bone. Br Dent J. 1984;156:287–91. doi: 10.1038/sj.bdj.4805346. [DOI] [PubMed] [Google Scholar]
- 20.Galloway SE, Pashley DH. Rate of removal of root structure by the use of the Prophy-Jet device. J Periodontol. 1987;58:464–9. doi: 10.1902/jop.1987.58.7.464. [DOI] [PubMed] [Google Scholar]
- 21.Petersilka GJ, Bell M, Häberlein I, Mehl A, Hickel R, Flemmig TF. In vitro evaluation of novel low abrasive air polishing powders. J Clin Periodontol. 2003;30:9–13. doi: 10.1034/j.1600-051x.2003.300102.x. [DOI] [PubMed] [Google Scholar]
- 22.Petersilka G, Faggion CM, Jr, Stratmann U, Gerss J, Ehmke B, Haeberlein I, et al. Effect of glycine powder air-polishing on the gingiva. J Clin Periodontol. 2008;35:324–32. doi: 10.1111/j.1600-051X.2007.01195.x. [DOI] [PubMed] [Google Scholar]
- 23.De Spain B, Nobis R. Comparison of rubber cup polishing and air polishing on stain, plaque, calculus and gingival. Dent Hyg. 1988;62:55. Retraction in: Hodges K, editor. Concepts in Nonsurgical Periodontal Therapy. 1st ed. New York: Delmar; 1998. p. 345-66. [Google Scholar]
- 24.Garcia-Godoy F, Medlock JW. An SEM study of the effects of air-polishing on fissure surfaces. Quintessence Int. 1988;19:465–7. [PubMed] [Google Scholar]
- 25.Braun A, Krause F, Frentzen M, Jepsen S. Removal of root substance with the Vector-system compared with conventional debridement in vitro. J Clin Periodontol. 2005;32:153–7. doi: 10.1111/j.1600-051X.2005.00651.x. [DOI] [PubMed] [Google Scholar]
- 26. [Last accessed on 2014 Aug 12]. Available from: http://www.dentistryiq.com/articles/2010/06/polishing-pastes-html .
- 27. [Last accessed on 2014 Aug 12]. Available from: http://www.rdhmag.com/articles/print/volume-29/issue-5/feature/to-polish-or-not-to-polish-html.