

Abstract
Gumma is a characteristic lesion of tertiary syphilis that is rare nowadays, but still rarer is squamous cell carcinoma (SCC) arising from it. A 74-year-old male presented with throat pain and nasal twang with a past history of genital ulcer. Examination revealed a well-defined ulcer with a perforation of 1.5 cm over the hard palate with induration and nodularity at the margins. This patient also had leukoplakia over the ventral aspect of the tongue. His treponema pallidum hemagglutination assay was positive, and biopsy revealed well-differentiated SCC from the lesion over the palate and leukoplakia with dysplasia from the lesion over the tongue. Patient is on treatment from radiotherapy. To conclude, this is a unique presentation of syphilitic gumma with palatal perforation with SCC and syphilitic leukoplakia with Ca in situ over tongue. Thus, serology for syphilis should be done in all patients with SCC of the oral cavity.
Keywords: Palatal perforation, squamous cell carcinoma, syphilitic gumma, syphilitic leukoplakia
INTRODUCTION
Syphilitic gummas are rare, but squamous cell carcinoma (SCC) occurring on it would be still rarer. Gumma is the characteristic and most frequent lesion of tertiary syphilis. The word Gumma is derived due to the gummy consistency of the necrotic stringy mass formed as a result of coagulation necrosis. It is a deep granulomatous process usually occurring 2-40 years from onset of infection. Syphilitic leukoplakia is due to friction with teeth while eating and talking. It is as a result of impaired blood supply to mucous membrane due to gummatous infiltration leading on to inadequate repair.[1] SCC can occur on a syphilitic gumma as well as on a leukoplakia but is very rare. Here, we report a male patient with SCC on a syphilitic gumma and a syphilitic leukoplakia with dysplasia.
CASE REPORT
A 74-year-old man presented to our department with a history of nasal twang and nasal regurgitation since many years. He also had a swelling over the palate that ulcerated since 1 month. He gives a history of penile ulcer at the age of 18 following a premarital exposure. On examination, there was a white patch of 1 cm × 1 cm over the ventral aspect of the tongue [Figure 1]. There was also a perforation of 1.5 cm × 1 cm over the hard palate with induration and sloughing at the margins [Figure 2]. An atrophic scar of 2 cm × 2 cm was present over the prepuce. There was a firm to hard cervical lymphadenopathy. Neurological evaluation revealed features suggestive of bilateral pyramidal signs. His erythrocyte sedimentation rate was raised, venereal disease research laboratory (VDRL) was 1:1 and treponema pallidum hemagglutination assay was positive. His cerebrospinal fluid VDRL and HIV were negative. Biopsy from palatal lesion showed squamous cells with nuclear hyperchromasia and high mitotic index extending beyond the basement membrane [Figure 3a]. Epithelial pearl/keratin whorl/malignant pearl was seen as concentric squames of keratin within an epithelial island [Figure 3b]. There was also areas of necrosis with surrounding lymphocytic infiltrate [Figure 3c]. Biopsy from the leukoplakia of the tongue showed marked epithelial dysplasia with an intact basement membrane. There was cellular atypia with hyperchromatic nuclei [Figure 4]. Patient was treated with doxycycline twice a day for 28 days and was referred to surgery and radiotherapy for further management.
Figure 1.
Leukoplakia over the ventral aspect of the tongue
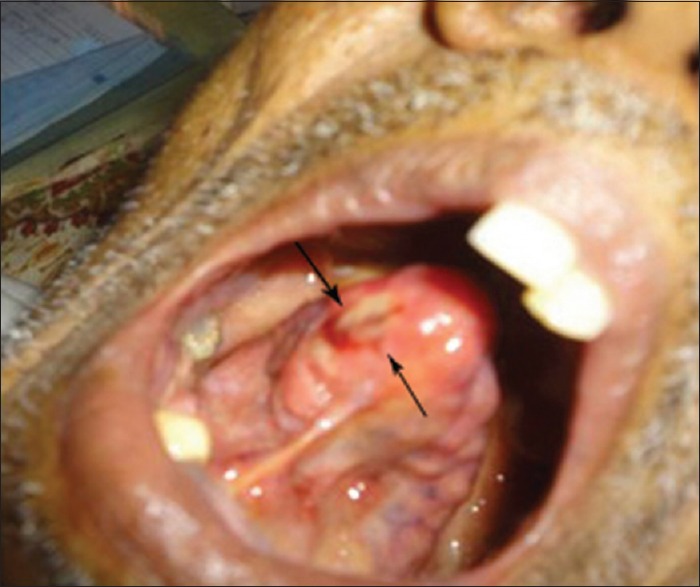
Figure 2.

Perforation of the hard palate with induration and necrotic tissue at the margins
Figure 3.

(a) Squamous cells with nuclear hyperchromasia and mitotic figures in a biopsy from palatal lesion on (H and E, ×400), (b) malignant pearl with concentric rings of keratin within an epithelial island on (H and E, ×400), (c) areas of necrosis with a background of lymphocytic infiltrate on (H and E, ×100)
Figure 4.

(a) Epithelial dysplasia with basement membrane intact from a biopsy taken from leukoplakia on (H and E, ×100), (b) epithelial dysplasia on (H and E, ×400)
DISCUSSION
Gummas are the characteristic lesion of tertiary syphilis. Spirochetes are difficult to demonstrate at this stage and are a result of hypersensitivity response to endogenous or exogenous treponemal antigen. Mostly (70%) it occurs on the skin. Another 10.3% occur in the mucosa and the rest in the liver, bones, lung and brain. In the skin, it starts as subcutaneous nodules that break down to form punched out ulcers with a yellowish white necrotic tissue attached to the floor and the wall giving a wash leather appearance. It heals with a thin, papery, noncontractile scar known as tissue paper scarring. Oral lesions of the gumma mainly occur on hard palate and tongue.[1] On the palate, it starts as one or more painless nodules that ulcerates leading to bony destruction causing palatal perforation and oronasal fistula formation that was seen in our case was also noted by others.[1,2] Gumma can involve the dorsa of tongue causing chronic superficial glossitis that is a misnomer as there are deeper infiltrations causing scarring and fissuring.
Leukoplakia is any white patch that cannot be due to any known cause. Syphilitic leukoplakia is due to the friction with teeth and the impaired blood supply due to gummatous infiltration rendering the repair inadequate. Leukoplakia affecting large areas of dorsum of the tongue was reported by Hutchinson et al., way back in the 19th century. A large US based study of 16,420 people with syphilis showed an increase in risk of SCC of the tongue.[3] Five out of 63 UK patients with SCC of the tongue had history of syphilis.[4] Malignant transformation can occur in 3–33% of leukoplakia that is more with verrucous, speckled and erythroleukoplakia. Our patient also had dysplastic changes to suggest Ca in situ from the biopsy taken from leukoplakia. The lesion from hard palate had all the features of SCC with nuclear hyperchromasia and mitotic figures with malignant pearls as a result of keratin formed by the malignant cells. About 90% of oral carcinomas are due to SCC mainly affecting the lips and middle 1/3 of the lateral tongue. Sump area or the Coffin corner that is the posterior tongue and floor of mouth requires a special search as these are the prone areas that could be missed. Detection of the biopsy site could be done with in vivo staining with toluidine blue followed by an acetic acid 1% rinse. Oral SCC and Ca in situ have an affinity for toluidine blue. SCC occurring on a gumma is more in males as in our patient. There was a report of 50-year-old man presenting with Syphilitic gumma on left shin turning to SCC by Pavithran and Riyaz[5]. The probable mechanism would be SCC occurring on a chronic scar or chronic ulceration due to gumma. Scar SCC usually begins decades after injury or chronic ulcer. Gradually nodularity and bleeding develop which was also reported by our patient. Presence of scar tissue or necrosis indicates a recurrent disease or sinister scar. Necrosis with a background of inflammatory lymphocytes adjacent to the malignant cells was also seen in the biopsy from the palate. To conclude, serology of syphilis should be done in all patients with SCC of the oral cavity. Unresponsiveness to a specific antisyphilitic treatment, we should always rule out malignancy. This is a very unique case of syphilitic gumma with palatal perforation with SCC on it and syphilitic leukoplakia of the tongue with Ca in situ.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Leão JC, Gueiros LA, Porter SR. Oral manifestations of syphilis. Clinics (Sao Paulo) 2006;61:161–6. doi: 10.1590/s1807-59322006000200012. [DOI] [PubMed] [Google Scholar]
- 2.Ramstad T, Traaholt L. Destruction of the soft palate and nose by tertiary ‘benign’ syphilis. A case report. J Oral Rehabil. 1980;7:111–5. doi: 10.1111/j.1365-2842.1980.tb00426.x. [DOI] [PubMed] [Google Scholar]
- 3.Michalek AM, Mahoney MC, McLaughlin CC, Murphy D, Metzger BB. Historical and contemporary correlates of syphilis and cancer. Int J Epidemiol. 1994;23:381–5. doi: 10.1093/ije/23.2.381. [DOI] [PubMed] [Google Scholar]
- 4.Dickenson AJ, Currie WJ, Avery BS. Screening for syphilis in patients with carcinoma of the tongue. Br J Oral Maxillofac Surg. 1995;33:319–20. doi: 10.1016/0266-4356(95)90046-2. [DOI] [PubMed] [Google Scholar]
- 5.Pavithran K, Riyaz N. Squamous cell carcinoma arising from Gumma. Indian J Dermatol Venereol Leprol. 2000;66:270–1. [PubMed] [Google Scholar]