

Introduction
The neurobiological continuum linking the two psychotic illnesses – schizophrenia and bipolar disorder - is elusive despite two decades of rapid advance in neuroscientific methods (Keshavan et al. 2011; Kaur et al. 2012). In the past, neuroimaging studies have mostly focused on trying to differentiate between schizophrenia spectrum and bipolar disorder, by aiming to identify disease-specific mechanisms in each of these disorders (Curtis et al. 2001; Whalley et al. 2009; Costafreda et al. 2009; Hall et al. 2010). Current evidence suggests that these two disorders share a significant overlap in genetic susceptibility (Craddock et al. 2005; Berrettini, 2011), pharmacological treatment responses (Murray et al. 2004), neuropsychological deficits (Hill et al. 2009), and epidemiological features and hence possibly a common pathophysiology, thereby challenging the so called Kraepelinian dichotomy (Kraepelin, 1919). In light of this, an emphasis on identifying the similarities and shared neural mechanisms between these two illnesses could aid the understanding of the pathophysiological basis of the clinical continuum of psychosis.
Along with functional imaging and grey matter alterations, studying changes in the white matter microstructure have provided valuable insights into the possible pathophysiology or course of these disorders. White matter abnormalities, observed using Diffusion Tensor Imaging (DTI) suggesting altered connectivity have been consistently reported in both bipolar disorder (Chan et al. 2010; Heng et al. 2010; Benedetti et al. 2011; Benedetti et al. 2011) and schizophrenia (Chan et al. 2010; Kunimatsu et al. 2012; Mandl et al. 2013; Levitt et al. 2012). However, the literature on DTI-based direct comparison between schizophrenia and bipolar disorder is scarce. Four studies exist (McIntosh et al. 2008; Sussman et al. 2009; Lu et al. 2011; Cui et al. 2011) but have examined samples that differ in important respects. Two studies did not exclude patients without psychosis (McIntosh et al. 2008; Sussmann et al. 2009). The other two studies (Lu et al. 2011; Cui et al. 2011) have examined patients with first episode psychosis and hence might be biased against observing a dichotomy as the chronic time course that was a key feature of Kraepelin’s concept of dementia praecox is less clearly discernible during the first episode.
The majority of DTI studies employ the measure of Fractional Anisotropy (FA) to study WM integrity. Though FA is a sensitive index of white matter microstructure, the neuronal interpretation of this measure is limited due to its composite nature. Pathological changes in FA can occur due to either axonal damage or myelin degradation and in order to decipher their relative contributions to FA change, along with calculating FA, it is necessary to also derive measures of Axial (AD) and Radial Diffusivity (RD) (Alexander et al. 2007; Seal et al. 2008). Secondly, FA alone cannot provide enough information about the microstructural architecture of the WM tracts. A newly developed tensor index called Mode of Anisotropy (MoA) can detect the predominance of crossing-fibre orientation in the white matter, thereby allowing for a more meaningful interpretation of FA results (Ennis & Kindmann, 2006; Jolapara et al. 2009). Although these indices have been employed in a number of recent DTI studies, a comprehensive analysis using multiple indices of WM integrity to identify the neural basis of psychotic continuum has not been reported yet.
Thus, to address these issues, we studied a sample representative of the two ‘poles’ of the ‘Kraepelinian axis’, with a focus on localizing brain regions which share altered white matter connectivity across the psychotic disorders. Such abnormalities, if identified, would represent the structural underpinnings of the putative Kraepelinian axis itself, rather than the correlates of one of the two poles of this axis. We aimed to delineate the WM abnormalities that are common to both poles of the axis initially by undertaking an exhaustive search for FA changes in the entire patient group when compared to non-psychotic healthy controls, followed by a comprehensive measurement of AD, RD and MoA in the regions showing a shared WM dysconnectivity. A prominent feature of Kraepelin’s concept of dementia praecox was poor outcome (Heckers, 2008). Nonetheless, while outcome is generally better in bipolar disorder, the evidence indicates a continuum of symptomatic, cognitive and functional outcome (Johnstone et al. 1992). This suggests that the pathological process common to both disorders might be more strongly expressed in schizophrenia but nonetheless associated with indices of poor outcome across the spectrum psychotic disorders. We there predict that the severity of WM dysconnectivity would be related to the functional ability and persistent symptom burden in individuals with psychosis.
Methods
Participants
Patients undergoing treatment for psychotic disorders were referred by the Early Intervention in Psychosis teams and other community-based mental healthcare teams in Nottinghamshire and Leicestershire, England. Upon referral clinical information was collected using retrospective review of case notes, discussion with referring clinicians and a video-recorded clinical interview using standardized symptom assessment procedure (Signs and Symptoms in Psychotic Illness Scale – SSPI) (Liddle et al. 2002). The clinical diagnosis was made in a consensus meeting in accordance with the best estimate procedure described by Leckman et al. (Leckman et al. 1982). Patients aged 18 to 50 years satisfying the DSM IV criteria for schizophrenia or schizoaffective disorder (SCZ), or bipolar disorder with psychotic features (BPP) were included in the study, provided they satisfied the following inclusion criteria: 1) IQ of at least 65 assessed using the Quick Test (Ammons & Ammons, 1962), 2) No lifetime history of substance dependence or harmful use in the past 6 months, 3) No history of significant head trauma or medical conditions likely to have appreciable neurological or psychiatric effects 4) No contraindications for MRI safety assessed by a standardized safety screening questionnaire.
All patients were in a stable phase of illness, defined as a change of no more than 10 points in their ‘Global Assessment of Function’ (GAF) (GAF, DSM-IV) (APA, 1994) score between assessment 6 weeks prior to and immediately prior to study participation. 55 out of 64 patients were receiving psychotropic medications. The median Defined Daily Dose (WHO-CCDSM, 2003) was calculated separately for antipsychotics, mood stabilizers including lithium and antidepressants and no patient had a change in any of these medications six weeks prior to participating in this study.
Healthy controls were recruited from the local community via advertisements and participants were recruited and group-matched to the patient group for age and parental socio-economic status (Rose & Pevalin, 2003). Controls satisfied the same inclusion and exclusion criteria as the patients, as specified above, and in addition did not have a personal or family history of psychotic disorders. A clinical interview by a research psychiatrist was employed to ensure that the controls were free from current axis 1 disorder and a history of either psychotic illness or neurological disorder. Handedness was assessed for both patients and healthy controls using the 12-items Annett scale (Annett, 1970). Social and occupational functioning in patients was evaluated using the SOFAS - Social and Occupational Functioning Assessment Scale (SOFAS - DSM IV) (APA, 1994). The clinical and demographic features of the sample are presented in Table 1.
Table 1. Clinical and Demographic Features.
| Features | Patients (N = 62) | Controls (N = 41) Mean/N (SD) |
|
|---|---|---|---|
| SCZ (N = 40) Mean/N (SD) |
BPP (N = 22) Mean/N (SD) |
||
|
| |||
| Gender (Male/Female) | 30/10 | 15/7 | 30/11 |
| Handedness (R/L) | 35/5 | 19/3 | 37/4 |
| Age | 33.5 (9.02) | 34.72 (10.51) | 33.24 (9.04) |
| Parental NS-SEC | 2.47 (1.50) | 1.70 (1.17) | 1.97 (1.29) |
| Quick Test (IQ) | 95.76 (13.48) | 102.80 (14.59) | 105.78(11.72) |
| Mean Illness Duration (Years) | 9.92 (7.57) | 10.68 (8.35) | - |
| Number of Episodes | 2.36 (1.51) | 3.40 (1.69) | - |
| DDD Antipsychotics | 1.29 (1.09) | 0.47 (0.59) | - |
| DDD Mood Stabilizers | 0.06 (0.24) | 0.91 (0.63) | - |
| DDD Antidepressants | 0.32 (0.66) | 0.07 (0.32) | - |
| DDD (all psychotropics) | 1.67 (1.33) | 1.46 (0.97) | - |
| SOFAS Score | 53.75 (12.32) | 61.04 (13.14) | - |
| Reality Distortion | 2.50 (2.62) | 0.57 (1.46) | - |
| Psychomotor Poverty | 2.80 (3.48) | 0.42 (1.20) | - |
| Disorganization | 1.57 (1.87) | 1.14 (1.98) | - |
| Anxiety/Depression | 2.05 (1.99) | 1.23 (1.48) | - |
| Psychomotor Excitation | 1.15 (1.33) | 3.23 (3.44) | - |
| SSPI Total Score | 11.5 (7.53) | 8.57 (8.12) | - |
NS-SEC: National Statistics Socio-Economic Classification; SSPI: Signs and Symptoms of Psychotic Illness; DDD: Defined Daily Dose; SOFAS: Social and Occupational Functioning Assessment Scale.
The issue of appropriate matching to minimise risk of group differences in brain development unrelated to the pathophysiology of schizophrenia remains a subject of debate. There is consistent evidence that moderate lowering of IQ is related to the pathophysiology of schizophrenia and in particular, current IQ is influenced by factors such as age at onset of the disease, illness duration, severity of symptoms (Aylward et al. 1984; Woodberry et al. 2008). Therefore we did not match for IQ. Nonetheless, to avoid inclusion of cases with IQ deficits greater than those typically observed in schizophrenia, we excluded individuals with a proxy estimate of current IQ lower than 65, as measured by the Quick Test.
We used parental socio-economic status as a matching variable in this study. Parental occupational status might be expected to predict brain development (Noble et al. 2005; Farah et al. 2006). Although there is evidence that parental occupational status is at last weakly predictive of risk of schizophrenia or of severity of illness, the evidence is ambiguous (Parrott & Lewine, 2005). We therefore consider that matching groups for parental occupational status is the most appropriate way to minimise risk of group differences in brain development that are not directly related to the pathophysiology of schizophrenia.
The original sample consisted of 37 patients with schizophrenia, 6 with schizoaffective disorder, 22 patients with bipolar disorder and 41 controls, but 2 subjects with schizophrenia were excluded due to movement artefacts in the DTI scans, while 1 subject with schizophrenia did not complete the DTI acquisition protocol as planned, providing a final sample of 103 subjects (34 with schizophrenia, 6 with schizoaffective disorder, 22 with bipolar disorder and 41 controls). Functional connectivity findings from this sample have already been reported (Palaniyappan & Liddle, 2014).
Due to the small number of subjects with schizoaffective disorder, this group was included with schizophrenia group for further analysis; when undertaking direct comparison between BPP and SCZ, we conducted sensitivity analysis by excluding the schizoaffective patients from SCZ. The study was approved by the National Research Ethics Committee, Derbyshire, UK. Written informed consent was obtained from all study participants in accord with the procedure approved by the Ethics Committee.
Image Acquisition
All scans were conducted at Sir Peter Mansfield Magnetic Resonance Centre, University of Nottingham using 3T Philips Achieva MR Scanner ({Philips Medical Systems, Best, The Netherlands). Diffusion-weighted images were acquired using a single-shot, spin-echo, echo planar imaging (EPI) sequence in alignment with the anterior commissure - posterior commissure (AC-PC) plane. The acquisition parameters were as follows: Repetition Time (TR) = 8.63 s, Echo Time (TE) = 56.9 ms, voxel size = 2mm isotropic, 112 × 112 matrix, Field of View (FoV) = 224 × 224 × 104, flip angle = 90°, 52 slices, 32 directions with a b-factor of 1000s/mm2, EPI Factor = 59, total scan time = 6.29 min. Scans were inspected immediately after each acquisition, and if motion was detected, scans were repeated.
Data Pre-processing
Diffusion weighted data were converted from DICOM in order to analyze images. FSL (FMRIB) was used for all data pre-processing and analysis (www.fmrib.ox.ac.uk/fsl). FSL’s Diffusion Toolbox (FDT) was used in order to correct for head motion and eddy current distortions (Behrens et al. 2003). In order to remove non-brain voxels, the Brain Extraction Tool (BET) was used to create a binary mask from the non-diffusion weighted data (Smith, 2002). Diffusion tensor and associated parameters such as Fractional Anisotropy, Axial and Radial Diffusivity and Mode were then calculated by applying a single tensor model using the DTIFIT tool in FSL. In preparation for tractography, the data was also run through the program BEDPOSTX to build probability distributions on diffusion parameters and model for crossing fibres at each voxel (Behrens et al. 2007).
FA ranges from 0 to 1, where 0 indicates regions with isotropic diffusion and 1 indicates perfect linear diffusion that is expected along the WM fibers. Radial diffusivity is considered to represent the integrity of myelin while axial diffusivity is considered to represent axonal integrity. MoA varies from −1 to +1, with values closer to −1 indicate regions where high number of crossing fibers can be expected and +1 indicate regions where one fiber orientation predominates (Douaud et al. 2011). Lower MoA values observed within a specific WM region in group comparisons may indicate that the underlying architecture of the WM fibers in this region may be ‘disorganised’ in one group compared to the other.
Tract-Based Spatial Statistics
Tract-Based Spatial Statistics (TBSS) (Smith et al. 2006) was used in order to analyze the DTI data. First, the FA data were pre-processed in order to remove likely outliers from the diffusion tensor fitting. Non-linear transformation and affine registration was then performed in order to align all FA images to a standard space (Andersson et al. 2007; Andersson et al. 2007). Following registration, the mean FA image and skeleton which represents the centres of all tracts common to the group were created. The mean FA skeleton was then thresholded at 0.2, after which each subject’s aligned FA data was projected onto this skeleton, allowing for further voxelwise statistical analysis. A similar approach for transformation and registration followed by projection on to the TBSS skeleton was applied for the AD, RD and MoA images.
Statistical Analysis
Voxelwise statistical analysis were conducted using TBSS, in order to compare whole brain group level differences in FA between the two groups – all patients with psychosis (PSY) and healthy controls (HC). A t-test was used for the comparison with age and gender as covariates. A Threshold-Free Cluster Enhancement (TFCE) approach was adopted with 10,000 permutations to correct for multiple comparisons without having to specify an initial cluster-forming threshold, with equal weighting for the peak height and extent of clusters (Smith et al. 2006). We also used this statistical design to directly compare the two diagnostic groups: SCZ and BPP. We repeated this comparison initially by excluding the 6 subjects with schizoaffective disorder from the SCZ group, and then by including these 6 subjects in the BPP group.
Clusters surviving TFCE corrected p=0.05 from PSY vs. HC comparison were used to obtain individual binary masks to extract cluster specific mean FA, RD, AD and MoA values for each subject. FA, RD, AD and MoA from the clusters were compared using separate ANOVAs with diagnosis (HC, SCZ or BPP) as the independent variable and age and gender as covariates. Holm-Sidak corrected follow-up t-tests were applied to detect differences among the three diagnostic groups (Sidak, 1967). Multiple regression analyses used to predict symptom scores, number of episodes and functional outcome measured using SOFAS is described in the Results section below.
We used probabilistic tractography to visualise the connectivity of clusters showing significant group differences. The maxima of clusters surviving TFCE correction for the PSY vs. HC comparison in the TBSS analysis of FA were used to generate 3-mm radius spherical seed regions of interest (ROI). Probabilistic tractography (seed to rest of the brain) was carried out for each ROI using the FSL’s PROBTRACKX2 tool (5000 samples from each seed voxel; step length = 0.5 mm; curvature threshold = 0.2). The resulting connectivity maps were thresholded at 10% of the total generated tracts to remove voxels that showed extremely low connectivity, and to retain the major white matter pathway passing through the seed regions. Each subject’s FA map was transformed to standard space using the FMRIB Non-Linear Image Registration Tool (FNIRT).
Results
TBSS Voxelwise Statistical Analysis – Group Differences
Patients with psychosis had 5 significant clusters with reduced FA compared to controls. Clusters were located at diverse locations embracing longitudinal and interhemispheric tracts. These results are presented in Table 2 and Figure 1. In all of these regions both SCZ and BPP had reduced FA when compared with controls, with BPP vs. HC comparisons reaching statistical significance at clusters A, B and D (corrected p<0.05), and showing a trend towards significance in clusters C and E (corrected p=0.06). FA reduction was accompanied by an increase in RD and a reduction in MoA in both patient groups, but reaching statistical significance only in patients with schizophrenia. However, inspection of the values for FA in each diagnostic group at the local maxima within each of the 5 clusters reveals no consistent trend for the abnormalities to be greater in SCZ, indicating that the greater statistical significance in the contrast of SCZ with HC compared with the contrast of BPP with HC is due to the greater statistical power in the larger sample of SCZ. The spread of FA values in the three groups is shown in Figure 2.
Table 2. Regions showing FA reduction in patients with psychosis.
| Index | A | B | C | D | E | |
|---|---|---|---|---|---|---|
| MNI co-ordinates of COG in x, y, z | −7, 14, 21 | −27, −65, 17 | 17, −26, 36 | 23, −63, 29 | −17, −39, 39 | |
| WM tract labels a | Body of the Corpus Callosum | Left Posterior Thalamic (optic) Radiation, Forceps Major | Body of the Corpus Callosum | Right Inferior Fronto-occipital Fasciculus | Left Cingulate Gyrus Corona Radiata | |
| Cluster Extent | 3212 | 1585 | 1428 | 822 | 110 | |
| FA | Mean (SD) CTRLS | 0.697 (0.025) | 0.649 (0.025) | 0.572 (0.032) | 0.574 (0.025) | 0.506 (0.038) |
| Mean (SD) SCZ | 0.682 (0.025) | 0.624 (0.025) | 0.555 (0.032) | 0.548 (0.025) | 0.479 (0.038) | |
| Mean (SD) BPP | 0.679 (0.028) | 0.627 (0.028) | 0.548 (0.028) | 0.542 (0.023) | 0.481 (0.038) | |
| Diagnosis | F = 6.903 * | F = 15.970 * | F = 5.614 * | F = 10.930 * | F = 4.649 * | |
| AD | Mean (SD) CTRLS | 0.150 (0.006) | 0.143 (0.006) | 0.128 (0.006) | 0.129 (0.006) | 0.117 (0.006) |
| Mean (SD) SCZ | 0.151 (0.006) | 0.141 (0.006) | 0.129 (0.006) | 0.126 (0.006) | 0.118 (0.006) | |
| Mean (SD) BPP | 0.151 (0.004) | 0.141 (0.004) | 0.129 (0.004) | 0.126 (0.004) | 0.118 (0.004) | |
| Diagnosis | F = 0.231 | F = 1.800 | F = 0.773 | F = 2.900 | F = 0.474 | |
| RD | Mean (SD) CTRLS | 0.380 (0.006) | 0.420 (0.006) | 0.460 (0.006) | 0.460 (0.006) | 0.500 (0.006) |
| Mean (SD) SCZ | 0.410 (0.006) | 0.460 (0.006) | 0.500 (0.006) | 0.500 (0.006) | 0.540 (0.006) | |
| Mean (SD) BPP | 0.400 (0.004) | 0.440 (0.004) | 0.490 (0.004) | 0.490 (0.004) | 0.530 (0.004) | |
| Diagnosis | F = 6.070 * | F = 6.887 * | F = 4.667 * | F = 4.373 * | F = 3.165 * | |
| MoA | Mean (SD) CTRLS | 0.885 (0.032) | 0.728 (0.051) | 0.685 (0.064) | 0.594 (0.077) | 0.559 (0.115) |
| Mean (SD) SCZ | 0.870 (0.031) | 0.685 (0.050) | 0.648 (0.063) | 0.540 (0.076) | 0.495 (0.113) | |
| Mean (SD) BPP | 0.873 (0.032) | 0.708 (0.051) | 0.646 (0.061) | 0.539 (0.075) | 0.530 (0.117) | |
| Diagnosis | F = 3.235 * | F = 6.691 * | F = 4.644 * | F = 7.050 * | F = 2.277 | |
All clusters survived FWE corrected p value <0.05.
White matter labels are provided in accordance with JHU White Matter Tractography Atlas and the ICBM DTI-81 White Matter Labels Atlas (Mori et al. 2005). Only tracts with >5% probability are included in the labels.
Denotes p<0.05 for F tests.
Figure 1.

Clusters from the voxelwise analysis showing significant reduction in FA in psychotic patients (PSY) (n = 62) compared to healthy controls (HC) (n = 41). Results are shown overlaid on the mean FA image with the mean FA skeleton in green, using the COG co-ordinates, TFCE corrected p < 0.05 and have been thickened using the tbss_fill script in FSL. Left-right orientation is in accordance with radiological convention. Figures in right column shows 3D visualisation of tracts generated from probabilistic tractography overlaid on a standard MNI brain. For visualisation purposes, tracts displayed are those present in at least half of the subjects.
Figure 2.
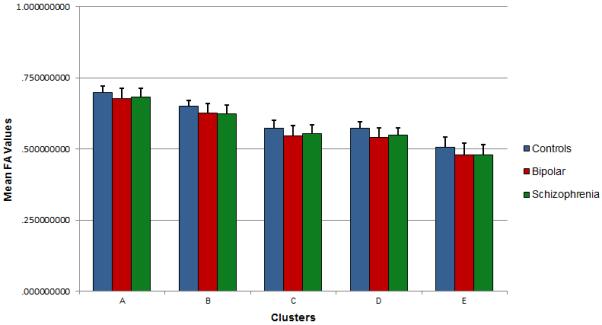
Mean FA values for the 5 clusters obtained from the TBSS analysis for each of the 3 groups – healthy controls (HC), schizophrenia (SCZ) and bipolar disorder (BPP). Error bars represent standard deviation (SD) values.
We did not find any brain regions showing statistically significant differences in FA when directly comparing SCZ and BPP. Even when the significance threshold was lowered to p=0.15, we did not observe differences between the two groups. The inclusion of schizoaffective patients in either SCZ or BPP did not alter this null observation.
WM Integrity Factor
In the PSY group, FA, AD, RD and MoA values for the clusters were all correlated with each other (mean absolute Pearson’s correlation value ∣r∣ = 0.33); this allowed us to extract a general principal component that explained 36.2% of the variance in the WM integrity measures across the clusters using unrotated Principal Component Analysis (Table 3). This component loaded positively on all the FA values of all clusters, and negatively on the RD values; thus the factor scores of this component represented the shared WM integrity across all patients. Patients with higher scores on this factor had intact WM structural integrity characterised by higher FA, MoA, AD and lower RD. This distribution of this factor was not different between SCZ and BPP (t=0.13, p=0.9). 6 separate multiple regression analyses were conducted to predict the SSPI scores of Reality Distortion, Disorganisation, Psychomotor Poverty, Anxiety/Depression, Psychomotor Excitation and the SOFAS scores and number of episodes in the PSY group, using the shared WM integrity factor and diagnostic status (SCZ and BPP) as predictors and age, gender and the combined daily dose of psychotropics (antipsychotics/mood stabilisers or antidepressants) as covariates. All variables (predictors and covariates) were entered in a single step in the regression analyses after ruling out multicollinearity among predictors using Statisstical Package for Social Sciences (version 21) . The results of this analysis are presented in Table 4. WM integrity predicted SOFAS but not the number of episodes or symptom scores. Reality Distortion, Psychomotor Poverty and Excitation were predicted by diagnostic classification (for both symptoms, SCZ > BPP), but not by WM integrity.
Table 3. Factor loading on the principal component (first unrotated factor) relating to WM integrity in patients with psychosis (PSY).
| Variables | Factor loading | Interpretation of the principal factor based on major components (variables with loading >0.4) |
|---|---|---|
| WM integrity (36.2% of variance) | Higher factor scores seen in patients with more anisotropic diffusion (higher FA), more prominent single fiber orientation (higher MoA), and uncompromised myelin integrity (lower RD). |
|
| FA Cluster A | +0.75 | |
| FA Cluster B | +0.79 | |
| FA Cluster C | +0.73 | |
| FA Cluster D | +0.80 | |
| FA Cluster E | +0.59 | |
| RD Cluster A | −0.83 | |
| RD Cluster B | −0.80 | |
| RD Cluster C | −0.84 | |
| RD Cluster D | −0.84 | |
| RD Cluster E | −0.82 | |
| AD Cluster A | −0.12 | |
| AD Cluster B | +0.34 | |
| AD Cluster C | −0.10 | |
| AD Cluster D | +0.33 | |
| AD Cluster E | −0.10 | |
| MoA Cluster A | +0.43 | |
| MoA Cluster B | +0.46 | |
| MoA Cluster C | +0.37 | |
| MoA Cluster D | +0.48 | |
| MoA Cluster E | +0.33 | |
FA: Fractional Anisotropy, RD: Radial Diffusion, AD: Axial Diffusion, MoA: Mode of Anisotropy.
Table 4. Multivariate analysis predicting functional status (SOFAS), SSPI syndrome scores and number of episodes in patients with psychosis.
| Independent Variables | ||||||
|---|---|---|---|---|---|---|
| WM Integrity |
Diagnosis (BPP = 0, SCZ =1 ) |
Age | Gender | DDD Psychotropics |
||
| Dependent Variables |
SOFAS score R2=0.25 β (p value) |
0.31(0.02) | −0.25(0.04) | 0.02 (0.89) | 0.34(0.01) | −0.07(0.93) |
|
Reality Distortion R2=0.18 β (p value) |
−0.08(0.56) | 0.29(0.03) | −0.12(0.41) | −0.05(0.69) | 0.19 (0.15) | |
|
Disorganization R2=0.05 β (p value) |
−0.11(0.45) | 0.01(0.97) | −0.08(0.58) | −0.19(0.18) | −0.08(0.59) | |
|
Psychomotor Poverty R2=0.20 β (p value) |
−0.25(0.08) | 0.32(0.02) | −0.19(0.18) | −0.11(0.39) | −0.07(0.62) | |
|
Anxiety/Depression R2= 0.14 β (p value) |
−0.26(0.06) | 0.13(0.32) | −0.22(0.13) | −0.18(0.89) | 0.22(0.10) | |
|
Psychomotor Excitation R2= 0.27 β (p value) |
−0.13(0.30) | −0.49(0.0001) | −0.26(0.05) | −0.12(0.32) | 0.07(0.54) | |
|
Number of Episodes R2= 0.29 β (p value) |
−0.12(0.36) | −0.11(0.35) | 0.41(0.003) | 0.17 (0.15) | −0.05(0.68) | |
No correlation was noted between the WM integrity factor and DDD of antipsychotics, mood-stabilisers and antidepressants (p values ranging from 0.2-0.8).
Discussion
Using microstructural indices derived from DTI, we have shown that reduced integrity in callosal, fronto-occipital and paralimbic WM, as indexed by FA, is a feature of psychosis, irrespective of the categorical diagnostic boundaries. This abnormality is specifically associated with an increase in radial diffusivity and reduction in the mode of anisotropy, suggesting defects in myelination along with a degree of ‘disorganisation’ in the underlying fibre structure in patients with psychosis.
The distribution of the WM factor scores that explain higher FA (and less RD) predicted the interindividual differences in the functional measure SOFAS after taking into account the variance explained by categorical diagnosis, age, gender and medication use. In other words, the degree of aberration in a neurobiological measure associated with the presence of psychosis relates to the degree of functional impairment that results from the illness.
We did not find any relationship between the WM factor and symptom clusters of Reality Distortion, Psychomotor poverty, Disorganisation, Anxiety/Depression or Excitation. This observation is consistent with the similar severity of the white matter abnormality in the two patient groups that differ in symptoms. On the other hand, the white matter abnormality was correlated with severity of occupational and social dysfunction demonstrating a relationship with clinical features present in both disorders. Nevertheless, it is important to note that our sample consisted of clinically stable patients in a medicated state. As a result, the degree of inter-individual variation in the severity of symptoms assessed on the day of the scan was modest.
No differences were observed in FA between SCZ and BPP, even at a lenient threshold. This observation is in agreement with previous reports of lack of differences in FA in both TBSS and tractographic studies (McIntosh et al. 2008; Sussman et al. 2009). In contrast, Lu et al. detected differences in FA between the two diagnostic groups in a first episode sample (Lu et al. 2011). In contrast to the TBSS approach used in our study, Lu et al. employed a voxel-based analysis which is more sensitive for changes in peripheral white matter, but is associated with reduced spatial (tract-to-tract) correspondence (Zalesky, 2011).
These results are also consistent with findings reported in some fMRI studies (Palaniyappan & Liddle, 2014; Argyelan et al. 2014; Brandt et al. 2014), which show that neural deficits in schizophrenia and bipolar disorder lie on a continuum, though in general abnormalities are more marked or more widespread in schizophrenia. However, other studies report more distinct, abnormalities in schizophrenia compared to bipolar disorder (Curtis et al. 2001; Costafreda et al. 2009; Whalley et al. 2009; Hall et al. 2010). It is likely that there are some brain features that do differ between the two disorders, though it should be noted that the finding of excessive activation of frontal cortex during task performance in bipolar disorder (e.g. Curtis et al. 2001; Costafreda et al. 2009) in contrast to underactivity often reported in schizophrenia does not exclude a continuum. Much evidence indicates that mild or moderate cortical inefficiency is associated with increased activation whereas severe disorder is associated with underactivity (Liddle et al. 2012).
A specific strength of this study is the use of MoA, which allowed us to meaningfully interpret FA changes in regions with predominant crossing fibres. Furthermore, the use of a TBSS approach has certain advantages. TBSS allows for microstructural evaluation of white matter tracts, while effectively dealing with alignment inaccuracies and spatial smoothing, which are issues common with VBM-based methods.
Several limitations must be considered while interpreting these findings. This study has a relatively small sample size, particularly for the bipolar group, and it is possible that significant differences between the two diagnostic groups might be detected with larger samples. Nonetheless, such results would not exclude a continuum in which the disorder might be more severe in schizophrenia. Most patients were medicated, with the majority of SCZ patients taking antipsychotics and many BPP patients taking mood stabilizers. A number of studies have shown an effect of prescribed psychotropics on white matter in the brain (Brambilla et al. 2009). For instance, some studies have shown a normalizing effect of lithium on FA values, with higher FA values observed in bipolar patients taking lithium as opposed to those on other medication (Hafeman et al. 2012). However, in our sample, we did not find any significant correlations between antipsychotic DDD or mood stabilizer DDD and white matter indices. Despite this, we cannot completely exclude the effect of prescribed medications on the current observations. Fewer females were included in the study compared to males, and hence all statistical procedures were undertaken by using gender as a covariate. Nevertheless, caution must be exercised when generalising these results to mixed samples.
Additionally, we acknowledge the possibility that the shared reduced white matter integrity found in patients with schizophrenia and bipolar disorder in our sample is a feature of psychiatric illness in general and not psychosis in particular as we did not include non-psychotic bipolar patients in our study. Furthermore, another study has shown no relationship between FA and values and lifetime history of psychotic symptoms in bipolar patients (McIntosh et al. 2008) and similar results have been found in a largely overlapping sample (Sussmann et al. 2009).
To conclude, similar white matter connectivity abnormalities in callosal, paralimbic and fronto-occipital regions are observed across the spectrum of psychotic illnesses. This shared dysconnectivity predicts functional outcome in psychosis, better than the clinical diagnostic boundary. Poor outcome is seen as the central feature of Kraepelin’s conception of dementia praecox (Heckers, 2008). While conventional diagnostic descriptions have failed to capture Kraepelin’s concept in a convincing fashion, augmenting this clinical information with neurobiological observations such as the one reported here brings new hopes for making progress in understanding psychosis.
Acknowledgment
This work was funded by Medical Research Council Grant G0601442. L Palaniyappan is supported by the Wellcome Trust (Research Training Fellowship WT096002/Z/11/Z). These funding organizations had no further role in study design, in the collection, analysis and interpretation of data, in the writing of the report, and in the decision to submit the paper for publication. We thank Drs Bert Park, Debasis Das and Raj Dangi for assistance with clinical recruitment and diagnostic consensus.
Footnotes
Declaration of interest: L Palaniyappan received a travel fellowship sponsored by Eli Lilly in 2011. In the past five years, P F Liddle has received honoraria for academic presentations from Janssen-Cilag and Bristol Myers Squibb; and has taken part in advisory panels for Bristol Myers Squibb.
References
- Alexander AL, Lee JE, Lazar M, Field AS. Diffusion tensor imaging of the brain. Neurotherapeutics. 2007;4:316–29. doi: 10.1016/j.nurt.2007.05.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aylward E, Walker E, Bettes B. Intelligence in schizophrenia: meta-analysis of the research. Schizophrenia Bulletin. 1984;10:430–459. doi: 10.1093/schbul/10.3.430. [DOI] [PubMed] [Google Scholar]
- Ammons RB, Ammons CH. The Quick Test (QT): provisional manual. Psychological Reports. 1962;11:111–161. [Google Scholar]
- Andersson JLR, Jenkinson M, Smith S. [Accessed: 10 April 2013];Non-linear optimisation. FMRIB technical report TR07JA1. 2007 www.fmrib.ox.ac.uk/analysis/techrep.
- Andersson JLR, Jenkinson M, Smith S. [Accessed: 10 April 2013];Non-linear registration, aka Spatial normalization. FMRIB technical report TR07JA2. 2007 www.fmrib.ox.ac.uk/analysis/techrep.
- Annett M. A classification of hand preference by association analysis. The British Journal of Psychology. 1970;61:303–321. doi: 10.1111/j.2044-8295.1970.tb01248.x. [DOI] [PubMed] [Google Scholar]
- APA . Diagnostic and statistical manual of mental disorders. 4th edn American Psychiatric Association; Washington, DC: 1994. [Google Scholar]
- APA . Diagnostic and statistical manual of mental disorders. 4th edn. American Psychiatric Association; Washington, DC: 1994. pp. 760–761. Axis V. [Google Scholar]
- Argyelan M, Ikuta T, DeRosse P, Braga RJ, Burdick KE, John M, Kingsley PB, Malhotra AK, Szeszko PR. Resting-state FMRI connectivity impairment in schizophrenia and bipolar disorder. Schizophrenia Bulletin. 2014;40:100–10. doi: 10.1093/schbul/sbt092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Behrens TE, Berg HJ, Jbabdi S, Rushworth MF, Woolrich MW. Probabilistic diffusion tractography with multiple fibre orientations: What can we gain? Neuroimage. 2007;34:144–55. doi: 10.1016/j.neuroimage.2006.09.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Behrens TEJ, Woolrich MW, Jenkinson M, Johansen-Berg H, Nunes RG, Clare S, Matthews PM, Brady JM, Smith SM. Characterization and propagation of uncertainty in diffusion-weighted MR imaging. Magnetic Resonance in Medicine. 2003;50:1077–1088. doi: 10.1002/mrm.10609. [DOI] [PubMed] [Google Scholar]
- Benedetti F, Absinta M, Rocca MA, Radaelli D, Poletti S, Bernasconi A, Dallaspezia S, Pagani E, Falini A, Copetti M, Colombo C, Comi G, Smeraldi E, Filippi M. Tract-specific white matter structural disruption in patients with bipolar disorder. Bipolar Disorders. 2011;13:414–424. doi: 10.1111/j.1399-5618.2011.00938.x. [DOI] [PubMed] [Google Scholar]
- Benedetti F, Yeh P, Bellani M, Radaelli D, Nicoletti MA, Poletti S, Falini A, Dallaspezia S, Colombo C, Giuseppe S, Smeraldi E, Soares JC, Brambilla P. Disruption of White Matter Integrity in Bipolar Depression as a Possible Structural Marker of Illness. Biological Psychiatry. 2011;69:309–317. doi: 10.1016/j.biopsych.2010.07.028. [DOI] [PubMed] [Google Scholar]
- Berrettini WH. Are Schizophrenic and Bipolar Disorders Related? A Review of Family and Molecular Studies. Biological Psychiatry. 2011;48:531–538. doi: 10.1016/s0006-3223(00)00883-0. [DOI] [PubMed] [Google Scholar]
- Brambilla P, Bellani M, Yeh PH, Soares JC. Myelination in bipolar patients and the effects of mood stabilizers on brain anatomy. Current Pharmaceutical Design. 2009;15:2632–6. doi: 10.2174/138161209788957519. [DOI] [PubMed] [Google Scholar]
- Brandt CL, Eichele T, Melle I, Sundet K, Server A, Agartz I, Hugdahl K, Jensen J, Andreassen OA. Working memory networks and activation patterns in schizophrenia and bipolar disorder: comparison with healthy controls. The British Journal of Psychiatry. 2014;204:290–8. doi: 10.1192/bjp.bp.113.129254. [DOI] [PubMed] [Google Scholar]
- Chan WY, Yang GL, Chia MY, Lau IY, Sitoh YY, Nowinski WL, Sim K. White matter abnormalities in first-episode schizophrenia: A combined structural MRI and DTI study. Schizophrenia Research. 2010;119:52–60. doi: 10.1016/j.schres.2009.12.012. [DOI] [PubMed] [Google Scholar]
- Chan WY, Yang GL, Chia MY, Woon PS, Lee J, Keefe R, Sitoh YY, Nowinski WL, Sim K. Cortical and subcortical white matter abnormalities in adults with remitted first-episode mania revealed by Tract-Based Spatial Statistics. Bipolar Disorders. 2010;12:383–389. doi: 10.1111/j.1399-5618.2010.00829.x. [DOI] [PubMed] [Google Scholar]
- Costafreda SG, Fu CH, Picchioni M, Kane F, McDonald C, Prata DP, Kalidindi S, Walshe M, Curtis V, Bramon E, Kravariti E, Marshall N, Toulopoulou T, Barker GJ, Davis AS, Brammer MJ, Murray RM, McGuire PK. Increased inferior frontal activation during word generation: a marker of genetic risk for schizophrenia but not bipolar disorder? Human Brain Mapping. 2009;30:3287–98. doi: 10.1002/hbm.20749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Craddock N, O’Donovan MC, Owen MJ. The genetics of schizophrenia and bipolar disorder: dissecting psychosis. Journal of Medical Genetics. 2005;42:193–204. doi: 10.1136/jmg.2005.030718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cui L, Chen Z, Deng W, Huang X, Li M, Ma X, Huang C, Jiang L, Wang Y, Wang Q, Collier DA, Gong Q, Li T. Assessment of white matter abnormalities in paranoid schizophrenia and bipolar mania patients. Psychiatry Research: Neuroimaging. 2011;194:347–353. doi: 10.1016/j.pscychresns.2011.03.010. [DOI] [PubMed] [Google Scholar]
- Curtis VA, Dixon TA, Morris RG, Bullmore ET, Brammer MJ, Williams SC, Sharma T, Murray RM, McGuire PK. Differential frontal activation in schizophrenia and bipolar illness during verbal fluency. Journal of Affective Disorders. 2001;66:111–21. doi: 10.1016/s0165-0327(00)00240-8. [DOI] [PubMed] [Google Scholar]
- Douaud G, Jbabdi S, Behrens TE, Menke RA, Gass A, Monsch AU, Rao A, Whitcher B, Kindlmann G, Matthews PM, Smith S. DTI measures in crossing-fibre areas: increased diffusion anisotropy reveals early white matter alteration in MCI and mild Alzheimer’s disease. Neuroimage. 2011;55:880–90. doi: 10.1016/j.neuroimage.2010.12.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ennis DB, Kindmann G. Orthogonal tensor invariants and the analysis of diffusion tensor magnetic resonance images. Magnetic Resonance in Medicine. 2006;55:136–46. doi: 10.1002/mrm.20741. [DOI] [PubMed] [Google Scholar]
- Farah MJ, Shera DM, Savage JH, Betancourt L, Giannetta JM, Brodsky NL, et al. Childhood poverty: specific associations with neurocognitive development. Brain Research. 2006;1110:166–174. doi: 10.1016/j.brainres.2006.06.072. [DOI] [PubMed] [Google Scholar]
- Hafeman DM, Chang KD, Garrett AS, Sanders EM, Phillips ML. Effects of medication on neuroimaging findings in bipolar disorder: an updated review. Bipolar Disorders. 2012;14:375–410. doi: 10.1111/j.1399-5618.2012.01023.x. [DOI] [PubMed] [Google Scholar]
- Hall J, Whalley HC, Marwick K, McKirdy J, Sussmann J, Romaniuk L, Johnstone EC, Wan HI, McIntosh AM, Lawrie SM. Hippocampal function in schizophrenia and bipolar disorder. Psychological Medicine. 2010;40:761–70. doi: 10.1017/S0033291709991000. [DOI] [PubMed] [Google Scholar]
- Heckers S. Making Progress in Schizophrenia Research. Schizophrenia Bulletin. 2008;34:591–594. doi: 10.1093/schbul/sbn046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heng S, Song AW, Sim K. White matter abnormalities in bipolar disorder: insights from diffusion tensor imaging studies. Journal of Neural Transmission. 2010;117:639–54. doi: 10.1007/s00702-010-0368-9. [DOI] [PubMed] [Google Scholar]
- Hill SK, Reilly JL, Margret SH, Harris, Rosen C, Marvin RW, DeLeon O, Sweeney JA. A comparison of neuropsychological dysfunction in first-episode psychosis patients with unipolar depression, bipolar disorder and schizophrenia. Schizophrenia Research. 2009;113:167–175. doi: 10.1016/j.schres.2009.04.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnstone EC, Frith CD, Crow TJ, Owens DG, Done DJ, Baldwin EJ, Charlette A. The Northwick Park ‘Functional’ Psychosis Study: diagnosis and outcome. Psychological Medicine. 1992;22:331–46. doi: 10.1017/s0033291700030270. [DOI] [PubMed] [Google Scholar]
- Jolapara M, Kesavadas C, Radhakrishnan VV, Saini J, Patro SN, Gupta AK, Kapilamoorthy TR, Bodhey N. Diffusion tensor mode in imaging of intracranial epidermoid cysts: one step ahead of fractional anisotropy. Neuroradiology. 2009;51:123–9. doi: 10.1007/s00234-008-0464-9. [DOI] [PubMed] [Google Scholar]
- Kaur M, Battisti RA, Lagopoulos J, Ward PB, Hickie IB, Franz CP, Hermens DF. Neurophysiological biomarkers support bipolar-spectrum disorders within psychosis cluster. Journal of Psychiatry & Neuroscience. 2012;37:313–21. doi: 10.1503/jpn.110081. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keshavan MS, Morris DW, Sweeney JA, Pearlson G, Thaker G, Seidman LJ, Eack SM, Tamminga C. A dimensional approach to the psychosis spectrum between bipolar disorder and schizophrenia: The Schizo-Bipolar Scale. Schizophrenia Research. 2011;133:250–254. doi: 10.1016/j.schres.2011.09.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kraepelin E. Dementia praecox and paraphrenia (trans.) 8th edn Livingstone; Edinburgh UK: 1919. [Google Scholar]
- Kunimatsu N, Aoki S, Kunimatsu A, Abe O, Yamada H, Masutani Y, Kasai K, Yamasue H, Ohtomo K. Tract-specific analysis of white matter integrity disruption in schizophrenia. Psychiatry Research: Neuroimaging. 2012;201:136–143. doi: 10.1016/j.pscychresns.2011.07.010. [DOI] [PubMed] [Google Scholar]
- Leckman JF, Sholomskas D, Thompson WD, Belanger A, Weissman MM. Best estimate of lifetime psychiatric diagnosis: a methodological study. Archives of General Psychiatry. 1982;39:879–883. doi: 10.1001/archpsyc.1982.04290080001001. [DOI] [PubMed] [Google Scholar]
- Levitt JL, Alvarado JL, Nestor PG, Rosow L, Pelavin PE, McCarley RW, Kubicki M, Shenton ME. Fractional anisotropy and radial diffusivity: Diffusion measures of white matter abnormalities in the anterior limb of the internal capsule in schizophrenia. Schizophrenia Research. 2012;136:55–62. doi: 10.1016/j.schres.2011.09.009. [DOI] [PubMed] [Google Scholar]
- Liddle EB, Bates AT, Das D, White TP, Groom MJ, Jansen M, Jackson GM, Hollis C, Liddle PF. Inefficient cerebral recruitment as a vulnerability marker for schizophrenia. Psychological Medicine. 2012;14:1–14. doi: 10.1017/S0033291712000992. [DOI] [PubMed] [Google Scholar]
- Liddle PF, Ngan ETC, Duffield G, Kho K, Warren AJ. Signs and Symptoms of Psychotic Illness (SSPI): a rating scale. The British Journal of Psychiatry. 2002;180:45–50. doi: 10.1192/bjp.180.1.45. [DOI] [PubMed] [Google Scholar]
- Lu LH, Zhou XJ, Keedy SK, Reilly JL, Sweeney JA. White matter microstructure in untreated first episode bipolar disorder with psychosis: comparison with schizophrenia. Bipolar Disorders. 2011;13:604–613. doi: 10.1111/j.1399-5618.2011.00958.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mandl RCW, Rais M, van Baal GCM, van Haren NEM, Cahn W, Kahn RS, Hulshoff Pol HE. Altered White Matter Connectivity in Never-Medicated Patients with Schizophrenia. Human Brain Mapping. 2013;34:2353–65. doi: 10.1002/hbm.22075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McIntosh AM, Maniega SM, Lymer GKS, McKirdy J, Hall J, Sussmann JED, Bastin ME, Clayden JD, Johnstone EC, Lawrie SM. White Matter Tractography in Bipolar Disorder and Schizophrenia. Biological Psychiatry. 2008;64:1088–1092. doi: 10.1016/j.biopsych.2008.07.026. [DOI] [PubMed] [Google Scholar]
- Mori S, Wakana S, Nagae-Petscher LM, van Zijl PCM. MRI Atlas of Human White Matter. Elsevier; Amsterdam: 2005. p. 284. [Google Scholar]
- Murray RM, Sham P, van OS J, Zanelli J, Cannon M, McDonald C. A developmental model for similarities and dissimilarities between schizophrenia and bipolar disorder. Schizophrenia Research. 2004;71:405–416. doi: 10.1016/j.schres.2004.03.002. [DOI] [PubMed] [Google Scholar]
- Noble KG, Norman MF, Farah MJ. Neurocognitive correlates of socioeconomic status in kindergarten children. Developmental Science. 2005;8:74–87. doi: 10.1111/j.1467-7687.2005.00394.x. [DOI] [PubMed] [Google Scholar]
- Palaniyappan L, Liddle PF. Diagnostic Discontinuity in Psychosis: A Combined Study of Cortical Gyrification and Functional Connectivity. Schizophrenia Bulletin. 2014;40:675–84. doi: 10.1093/schbul/sbt050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parrott B, Lewine R. Socioeconomic status of origin and the clinical expression of schizophrenia. Schizophrenia Research. 2005;75:417–424. doi: 10.1016/j.schres.2004.12.006. [DOI] [PubMed] [Google Scholar]
- Rose D, Pevalin DJ. A Researcher’s Guide to the National Statistics Socio-economic Classification. Sage Publications; London: 2003. [DOI] [PubMed] [Google Scholar]
- Seal ML, Yucel M, Fornito A, Wood SJ, Harrison BJ, Walterfang M, Pell GS, Pantelis C. Abnormal white matter microstructure in schizophrenia: a voxelwise analysis of axial and radial diffusivity. Schizophrenia Research. 2008;101:106–10. doi: 10.1016/j.schres.2007.12.489. [DOI] [PubMed] [Google Scholar]
- Sidak Z. Rectangular Confidence Regions for the Means of Multivariate Normal Distributions. Journal of the American Statistical Association. 1967;62:626–633. [Google Scholar]
- Smith SM. Fast robust automated brain extraction. Human Brain Mapping. 2002;17:143–155. doi: 10.1002/hbm.10062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith SM, Jenkinson M, Johansen-Berg H, Rueckert D, Nichols TE, Mackay CE, Watkins KE, Ciccarelli O, Cader MZ, Matthews PM, Behrens TEJ. Tract-based spatial statistics: Voxelwise analysis of multi-subject diffusion data. Neuroimage. 31:1487–1505. doi: 10.1016/j.neuroimage.2006.02.024. [DOI] [PubMed] [Google Scholar]
- Sussmann JE, Lymer GKS, McKirdy J, Moorhead TWJ, Munoz MS, Job D, Bastin ME, Johnstone EC, Lawrie SM, McIntosh AM. White matter abnormalities in bipolar disorder and schizophrenia detected using diffusion tensor magnetic resonance imaging. Bipolar Disorders. 2009;11:11–18. doi: 10.1111/j.1399-5618.2008.00646.x. [DOI] [PubMed] [Google Scholar]
- Whalley HC, McKirdy J, Romaniu L, Sussmann J, Johnstone EC, Wan HI, McIntosh AM, Lawrie SM, Hall J. Functional imaging of emotional memory in bipolar disorder and schizophrenia. Bipolar Disorders. 2009;11:840–56. doi: 10.1111/j.1399-5618.2009.00768.x. [DOI] [PubMed] [Google Scholar]
- WHO Collaborating Centre for Drug Statistics and Methodology . Guidelines for ATC Classification and DDD Assignment. WHO Collaborating Centre for Drug Statistics and Methodology; Oslo, Norway: 2003. [Google Scholar]
- Woodberry KA, Giuliano AJ, Seidman LJ. Premorbid IQ in schizophrenia: a meta-analytic review. The American Journal of Psychiatry. 2008;165:579–587. doi: 10.1176/appi.ajp.2008.07081242. [DOI] [PubMed] [Google Scholar]
- Zalesky Moderating registration misalignment in voxelwise comparisons of DTI data: a performance evaluation of skeleton projection. Magnetic Resonance Imaging. 2011;29:111–25. doi: 10.1016/j.mri.2010.06.027. [DOI] [PubMed] [Google Scholar]