

Abstract
It has become increasingly recognized that insufficient sleep is associated with adverse health outcomes. Studies have observed that sleep duration and daytime sleepiness varies by sex and marital status. Few studies have examined the impact of the number of children on sleep. To evaluate the association of marital status and number of children with insufficient sleep and in a large national sample. We analyzed data from the 2008 Behavioral Risk Factor Surveillance System (BRFSS) survey, a population-based telephone survey of non-institutionalized US adults (N = 395,407), in which respondents were asked, “During the past 30 days, for about how many days have you felt you did not get enough rest or sleep?” We used sex-specific, multivariate logistic regression analyses to assess the associations of marital status (married, previously married, never married) and the number of children in the household with frequent insufficient sleep (≥14 days in past 30 days) after adjusting for age, race/ethnicity, and education. In this study population, 23% were never married, 60% were married, and 17% were previously married. Forty-three percent reported having children aged <18 years in the household. Married men (24.3%) were less likely to report frequent insufficient sleep than never married men (28.0%) or previously married men (28.8%). Never married women (33.4%) were more likely to report frequent insufficient sleep than currently married (29.0%) or previously married women (29.0%). The likelihood of frequent insufficient sleep increased in a linear fashion with the number of children in the household for all subgroups (P <0.05) except among never married men. These findings suggest that the presence of children in the household often increases the frequency of insufficient rest or sleep among the adults with whom they reside. Thus, health care providers may wish to consider the presence of children under 18 years of age a potential “risk factor” for insufficient sleep when counseling adults in the household about the importance of sleep to overall health.
Keywords: Sleep, Insufficient sleep, Sleep deprivation, Epidemiology
Introduction
Insufficient sleep poses a substantial economic burden to society and is surprisingly prevalent. Specifically, 40% of respondents to the National Sleep Foundation’s 2005 Sleep in America Poll reported they averaged 6.9 h or less of sleep over the preceding 2 weeks [1]. These findings are particularly important as insufficient sleep can exacerbate the course of chronic conditions and augment the social disability associated with them [2–4]. Additionally, insufficient sleep has been associated with self-reports of fair or poor general health, pain, smoking, obesity, and an increased risk of psychiatric disorders [5–7]. Results from the 2007 Sleep in America Poll similarly found that poor sleep quality and daytime sleepiness were independently associated with poor health and psychological distress among women [8].
Given the gravity of these findings, research has been directed at identifying factors associated with the increased risk of insufficient sleep. Previous research in this area has found that unmarried individuals are significantly more likely to sleep for a short duration and, consistent with these findings, that married people reported less excessive daytime sleepiness than all other groups [9, 10]. In other studies, however, married and single people reported less sleep problems than their divorced or widowed counterparts and, specifically, reported fewer periods of short sleep [11–13]. These results suggest that changes in marital status may conceivably prove disruptive of sleep.
Women have, characteristically, reported more sleep problems than men [11, 12]. However, using data from the American’s Use of Time Project, Hale found that men were significantly more likely than women to be “short sleepers”—defined as sleeping less than 6.5 h per night [9]. Results obtained by other investigators corroborate these findings [13, 14]. Thus, the sleep problems reported by women would seem not to be related to total sleep time, but attributable to other factors. Arber, Bote, and Meadows found that while women reported significantly more sleep problems than men, this appeared to be largely attributable to the relative socioeconomically disadvantaged status of women relative to men [11].
The impact of children on the sleep of adults in the household has not been widely investigated and has frequently been investigated only in the context of the postpartum period [15, 16]. When modeled as a continuous variable, the number of children in the household under 15 years of age was found to be associated with insomnia in adult household members [12]. However, it must be noted that insomnia is but one of several forms of disturbed sleep.
Previous research has indicated that marital status, gender, and the presence of children in the household appear to be important considerations in the sleep of adult household members. Yet, this research also reveals a number of limitations, such as dichotomizing the number of children in the household (≤2, >2) [12], considering the age of children but not the number of children in the household [8], and examining marital status but not the presence of children in the household [9]. These limitations render it difficult to assess possible interactions between gender, marital status, and the number of children in the household.
The present investigation examines the role of all three of these variables—adult gender, marital status, and the number of children in the household—as well as their potential interaction, in a large sample of adult community-dwellers who indicated how frequently over the past 30 days they perceived that they got adequate rest or sleep.
Methods
We used data from the 2008 Behavioral Risk Factor Surveillance System (BRFSS) survey, an annual, state-based, random-digit-dialed telephone survey of the US civilian, non-institutionalized population aged ≥18 years. The survey is conducted in 50 states, the District of Columbia, and three US territories (Guam, Puerto Rico, and the Virgin Islands). The median response rate to the 2008 BRFSS survey among all 50 states and the District of Columbia was 53.3% (35.8–65.9%), based on Council of American Survey and Research Organizations guidelines, and the median cooperation rate among contacted households was 75.0% (59.3–87.8%).
Included among the sociodemographic questions asked of all participants were questions about marital status and number of children in the household. For the present analysis, respondents were grouped into three marital status categories which included married, previously married (including those who were divorced, separated, or widowed), and never married (including those who never married or were a member of an unmarried couple). The results for members of unmarried couples were more similar to those for never married individuals than those for married individuals: therefore these participants were categorized as never married in our analysis. Participants were also asked, “How many children less than 18 years of age live in your household?” In addition, all respondents were asked, “During the past 30 days, for about how many days have you felt you did not get enough rest or sleep?” Frequent insufficient sleep was defined as a response of C14 days in past 30 days.
There were 414,509 respondents to the 2008 BRFSS survey. We excluded from our analysis those with missing data for marital status (n = 1,673), number of children in the household (n = 1,062), days of insufficient sleep (n = 7,060), age (n = 3,653), race/ethnicity (n = 4,344), and education (n = 1,281), as well as women who indicated that they were pregnant (n = 2,803). Therefore the final study sample consisted of 395,407 US adults (95.4%).
We conducted all analyses using SAS-callable SUDA-AN (version 10.0.0, Research Triangle Park, NC) to account for the complex sampling design of the BRFSS. We calculated the proportion of respondents reporting frequent insufficient sleep during the previous 30 days by sex, marital status, and number of children in the household. We used sex-specific multivariate logistic regression models to assess the separate and independent relationships of marital status and number of children to the likelihood of frequent insufficient sleep. In another sex-specific model, we assessed an interaction term for marital status and number of children. Odds ratios (OR), and 95% confidence intervals (CI) were obtained from these models which included age in years (18–24, 25–34, 35–44, 45–54, 55–64, and ≥65), race/ethnicity (non-Hispanic white, non-Hispanic black, Hispanic, and non-Hispanic other races), and education level (less than high school graduate, high school graduate or GED recipient, some college, and college graduate) as covariates.
Results
Weighted population characteristics are shown in Table 1. Most individuals were married (60.1%), 17.0% were previously married (divorced, separated, or widowed), and 22.9% were never married or a member of an unmarried couple. More than half (57.0%) of adults had no children living in the household, while nearly one in ten (9.9%) had 3 or more children in the household. Frequent insufficient sleep (≥14 days in past 30 days) was reported by 27.9% of the respondents. Women were more likely to report insufficient sleep than men (29.9% vs. 25.7%).
Table 1.
Characteristics of respondents to perceived insufficient sleep question
| Characteristic | Na | %b |
|---|---|---|
| Total | 395,407 | 100.0 |
| Sex | ||
| Men | 150,106 | 49.4 |
| Women | 245,301 | 50.7 |
| Race/ethnicity | ||
| White, non-hispanic | 315,351 | 68.3 |
| Black, non-hispanic | 30,974 | 9.8 |
| Hispanic | 27,410 | 15.1 |
| Other/multiracialc | 21,672 | 6.8 |
| Age | ||
| 18–24 | 13,183 | 12.2 |
| 25–34 | 36,896 | 18.0 |
| 35–44 | 60,032 | 19.2 |
| 45–54 | 82,248 | 19.3 |
| 55–64 | 85,423 | 14.5 |
| ≥65 | 117,625 | 16.8 |
| Education | ||
| <High school diploma | 38,321 | 11.4 |
| High school diploma or GED | 119,494 | 28.8 |
| Some college | 105,259 | 26.6 |
| College graduate | 132,333 | 33.3 |
| Marital status | ||
| Never married | 47,029 | 19.0 |
| Member of an unmarried couple | 8,673 | 3.9 |
| Married | 222,144 | 60.1 |
| Divorced/separated/widowed | 117,561 | 17.0 |
| Children in householdd | ||
| No children | 278,138 | 57.0 |
| 1 Child | 46,579 | 16.9 |
| 2 Children | 44,140 | 16.2 |
| 3 or more children | 26,550 | 9.9 |
| Frequent insufficient sleepe | 101,285 | 27.9 |
Unweighted n’s
Weighted percentage
Asian, Native Hawaiian or Other Pacific Islander, American Indian/Alaska Native, or multiracial (no preferred race reported)
Number of children under 18 years old living in the household
Report ≥ 14 days of insufficient sleep in past 30 days
Among men, the prevalence of frequent insufficient sleep was 28.0% among those who had never married or were a member of an unmarried couple (Table 2). Compared to that group, the likelihood of frequent insufficient sleep was similar in married men (24.3%; adjusted OR = 1.1; 95% CI: 1.0–1.1) but higher among men who were previously married (28.8%; adjusted OR = 1.5; 95% CI: 1.3–1.6). The prevalence of frequent insufficient sleep was 22.5% among men with no children (Table 2). The prevalence increased with number of children with the likelihood of frequent insufficient sleep being higher among men with ≥3 children (31.4%; adjusted OR = 1.3; 95% CI: 1.2–1.4) compared to men with no children. There was a statistical interaction (P = 0.0217) between marital status and number of children among men. Frequent insufficient sleep was lowest for married men with no children (18.9%) (Fig. 1). After adjustment for age, race/ethnicity, and education in logistic regression analyses, the likelihood of frequent insufficient sleep increased linearly with the number of children for currently married (P <0.0001) and previously married men (P <0.0001), but additional children in the household had no significant effect on the likelihood of frequent insufficient sleep among men who were never married or were a member of an unmarried couple (P = 0.3536).
Table 2.
Independent effects of marital status and number of children on likelihood of frequent insufficient sleep (≥14 days in past 30 days) among adults aged ≥18 years, by sex: behavioral risk factor surveillance system survey, 2008
| ≥14 Days of insufficient sleep in past 30 days
|
|||||
|---|---|---|---|---|---|
| %a | ORb | (95% CI) | ORc | (95% CI) | |
| Men | |||||
| Total | 25.7 | ||||
| Marital status | |||||
| Never married/member of an unmarried couple | 28.0 | 1.00 | (Referent) | ||
| Married | 24.3 | 1.06 | (0.99–1.15) | ||
| Divorced/separated/widowed | 28.8 | 1.47 | (1.34–1.61) | ||
| Number of children | |||||
| No children | 22.5 | 1.00 | (Referent) | ||
| 1 Child | 28.9 | 1.14 | (1.05–1.23) | ||
| 2 Children | 30.8 | 1.25 | (1.16–1.35) | ||
| ≥3 Children | 31.4 | 1.28 | (1.16–1.40) | ||
| Women | |||||
| Total | 29.9 | ||||
| Marital status | |||||
| Never married/member of an unmarried couple | 33.4 | 1.00 | (Referent) | 1.00 | (Referent) |
| Married | 29.0 | 0.98 | (0.92–1.04) | 0.91 | (0.85–0.97) |
| Divorced/separated/widowed | 29.0 | 1.32 | (1.23–1.41) | 1.24 | (1.16–1.33) |
| Number of children | |||||
| No children | 25.0 | 1.00 | (Referent) | 1.00 | (Referent) |
| 1 Child | 34.6 | 1.24 | (1.16–1.31) | 1.24 | (1.17–1.32) |
| 2 Children | 35.9 | 1.29 | (1.22–1.37) | 1.32 | (1.24–1.41) |
| ≥3 Children | 39.3 | 1.47 | (1.36–1.58) | 1.50 | (1.39–1.62) |
Weighted unadjusted proportion
Weighted odds ratios (OR) and 95% confidence interval (CI) from multivariate logistic regression model that included age, race/ethnicity, and education as covariates and either marital status or number of children
Weighted OR and 95% CI from multivariate logistic regression model that included age, race/ethnicity, and education as covariates and both marital status and number of children as independent variables among women only. Among men there was a statistical interaction (P = 0.0217) between marital status and number of children in their relationship with insufficient sleep. Therefore it would not be appropriate to report results of the model given this interaction term among men
Fig. 1.
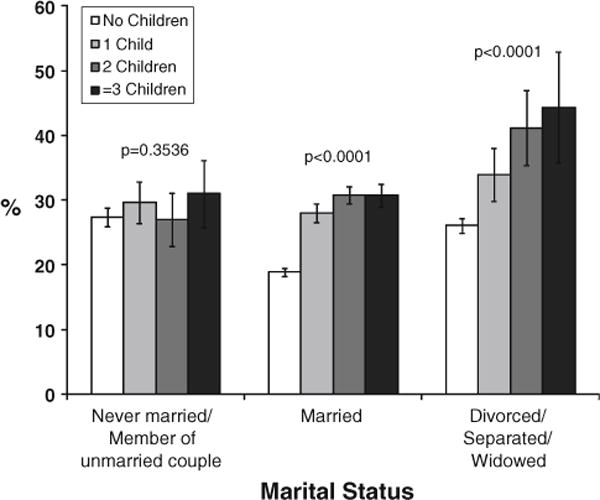
Unadjusted prevalence of frequent insufficient sleep (≥14 days in past 30 days) among men by marital status and number of children in household. P-value of Wald-F test for linear trend for number of children indicated above corresponding bars was obtained from multivariate logistic regression analyses that included age, race/ethnicity, and education
Among women, the prevalence of frequent insufficient sleep was 33.4% among those who had never married or were a member of an unmarried couple (Table 2). The likelihood of frequent insufficient sleep was similar in married women (29.0%; adjusted OR = 1.0; 95% CI: 0.9–1.0) but higher among women who were previously married (29.0%; adjusted OR = 1.3; 95% CI: 1.2–1.4). Similar relationships remained after including number of children in the logistic regression model. The prevalence of frequent insufficient sleep was 25.0% among women with no children (Table 2). The prevalence increased with the number of children such that the likelihood of frequent insufficient sleep was higher among women with ≥3 children (39.3%; adjusted OR = 1.5; 95% CI: 1.4–1.6) compared to women with no children. This relationship remained significant after including number of children in the logistic regression model. There was no significant interaction (P = 0.3218) between marital status and number of children among women. Similar to the findings among men, frequent insufficient sleep was lowest for married women with no children (23.3%) (Fig. 2). After adjustment for age, race/ethnicity, and education in logistic regression analyses, the likelihood of frequent insufficient sleep among women increased linearly with the number of children (P <0.0001), regardless of marital status.
Fig. 2.
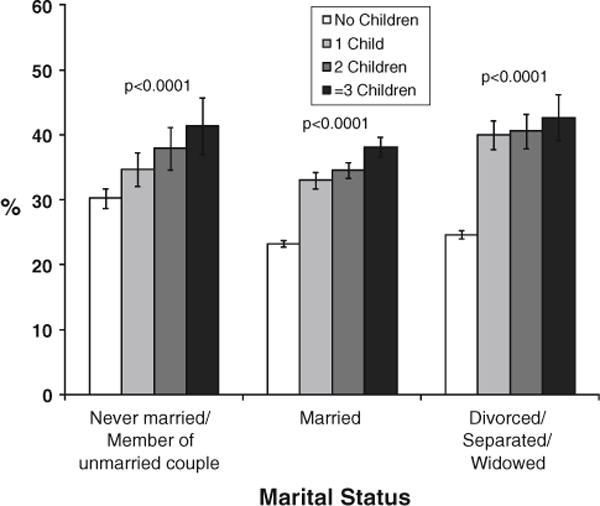
Unadjusted prevalence of frequent insufficient sleep (≥14 days in past 30 days) among women by marital status and number of children in household. P-value of Wald-F test for linear trend for number of children indicated above corresponding bars was obtained from multivariate logistic regression analyses that included age race/ethnicity, and education
Discussion
These data suggest that the presence of children influences self-reported sleep insufficiency among adults residing in the household, but several other factors must be considered in the interpretation of these findings. One such factor is marital status. Notably, for both men and women, married individuals with no children in the household were least likely to report frequent insufficient sleep. In contrast, previously married men and women reported more frequent insufficient sleep than their married counterparts, regardless of the number of children in the household. These results are partially in keeping with those of Ohayon, who, in a review of the literature, reported a higher prevalence of insomnia symptoms among separated/divorced or widowed individuals relative to married persons but, unlike the present investigation, noted a stronger association of this relationship in women than men [17]. Similarly, women who were dissatisfied with their quality of sleep and had insomnia symptoms were more likely to be separated, divorced, or widowed [18]. Our results also are similar to the findings of Arber et al. [11] who found that divorced, separated, or widowed men and women were more likely to report sleep difficulties than their married or single counterparts. Collectively, these findings corroborate our results indicating that marital status plays an important role in adult perceived sleep sufficiency.
The number of children in the household appears largely unexplored in previous research [19–21], which was examined dichotomously [12] or restricted to very young children [15]. Notably, we found that the likelihood of frequent insufficient sleep followed a linear trend with number of children for married and previously married men and women. Children in the household did not have a significant effect on the sleep of never married men, but the sleep of never married women was significantly impacted by children similarly to that of married and previously married women. The latter result appears consistent with previous research addressing the “gendered nature” of caring, inasmuch as the sleep of never married women was adversely affected by the presence of children in the household, while the sleep of never married men was not [22]. These results suggest the presence of an interaction between parental marital status and the number of children in the household among men.
While this study featured a sufficiently large sample size that enabled us to analyze data obtained from men and women respondents separately, as well as to assess the interaction between marital status and number of children, several limitations must also be noted. Specifically, these data are cross-sectional, which renders the inference of causality impossible. Second, the wording of the question, “During the past 30 days, for about how many days have you felt you did not get enough rest or sleep?” does not permit differentiation of rest from sleep. Also, the question posed elicits a subjective response, although this need not be viewed as a bias. Baker et al. [8] noted that subjective complaints regarding sleep are key facets of people’s motivation to seek professional help, are associated with mortality, and are generally correlated with objective measures. Previous studies have found racial differences in perceived insufficient sleep [23]. Although we adjusted for race/ethnicity in our analysis, we did not assess for a possible interaction between this variable with either marital status or number of children in the association of these demographic variables with insufficient sleep. Finally, the data do not reflect the nature of the relationship of the children to the respondent. Therefore, the respondent may not bear the primary responsibility for the child.
Insufficient sleep has become increasingly associated with adverse health outcomes. The presence of children in the household was associated with frequent insufficient sleep among adult household members in our study. In those instances where there is a discrepancy between men and women, it is invariably women who experience greater sleep insufficiency. From the vantage point of public health, these results suggest the need for instruction regarding the essential nature of sleep as a facet of parenting education. Ideally, such education would foster healthy sleep patterns in the entire family and more equitable sharing of nighttime childcare responsibilities, which may contribute, in part, to gender differences in sleep sufficiency. Sleep is essential and sufficient, healthy sleep should be as important as smoking cessation, healthy nutrition, and adequate physical activity in promoting overall health.
Acknowledgments
AGW received support from a fellowship through a cooperative agreement (award number 3U50CD300860) between the Association for Prevention Teaching and Research and the Centers for Disease Control and Prevention.
Footnotes
Disclaimer: The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention or the Association for Prevention Teaching and Research.
Contributor Information
Daniel P. Chapman, Email: DChapman@cdc.gov, Division of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, 4770 Buford Highway NE Mailstop K-67, Atlanta, GA 30041, USA.
Anne G. Wheaton, Division of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, 4770 Buford Highway NE Mailstop K-67, Atlanta, GA 30041, USA
Geraldine S. Perry, Division of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, 4770 Buford Highway NE Mailstop K-67, Atlanta, GA 30041, USA
Stephanie L. Sturgis, Division of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, 4770 Buford Highway NE Mailstop K-67, Atlanta, GA 30041, USA
Tara W. Strine, Division of Behavioral Surveillance, Public Health Surveillance Program Office, Centers for Disease Control and Prevention, Atlanta, GA 30041, USA
Janet B. Croft, Division of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, 4770 Buford Highway NE Mailstop K-67, Atlanta, GA 30041, USA
References
- 1.National Sleep Foundation. Summary of Findings. Sleep in America poll, methodology. 2005 Available at: http://www.sleepfoundation.org/sites/default/files/2005_summary_of_findings.pdf. Accessed 25 July 2011.
- 2.Manocchia M, Keller S, Ware JE. Sleep problems, health-related quality of life, work functioning and health care utilization among the chronically ill. Quality of Life Research. 2001;10(4):331–345. doi: 10.1023/a:1012299519637. [DOI] [PubMed] [Google Scholar]
- 3.Katz DA, McHorney CA. The relationship between insomnia and health-related quality of life in patients with chronic illness. The Journal of Family Practice. 2002;51(3):229–235. [PubMed] [Google Scholar]
- 4.Leger D, Scheuermaier K, Philip P, Paillard M, Guilleminault C. SF-36: Evaluation of quality of life in severe and mild insomniacs compared with good sleepers. Psychosomatic Medicine. 2001;63(1):49–55. doi: 10.1097/00006842-200101000-00006. [DOI] [PubMed] [Google Scholar]
- 5.Strine TW, Chapman DP. Associations of frequent sleep insufficiency with health-related quality of life and health behaviors. Sleep Medicine. 2005;6(1):23–27. doi: 10.1016/j.sleep.2004.06.003. [DOI] [PubMed] [Google Scholar]
- 6.Vandeputte M, de Weerd A. Sleep disorders and depressive feelings: A global survey with the Beck depression scale. Sleep Medicine. 2003;4(4):343–345. doi: 10.1016/s1389-9457(03)00059-5. [DOI] [PubMed] [Google Scholar]
- 7.Ford DE, Kamerow DB. Epidemiologic study of sleep disturbances and psychiatric disorders. An opportunity for prevention? JAMA. 1989;262(11):1479–1484. doi: 10.1001/jama.262.11.1479. [DOI] [PubMed] [Google Scholar]
- 8.Baker FC, Wolfson AR, Lee KA. Association of sociodemographic, lifestyle, and health factors with sleep quality and daytime sleepiness in women: Findings from the 2007 National Sleep Foundation “Sleep in America Poll”. Journal of Womens Health (Larchmt) 2009;18(6):841–849. doi: 10.1089/jwh.2008.0986. [DOI] [PubMed] [Google Scholar]
- 9.Hale L. Who has time to sleep? Journal of Public Health (Oxf) 2005;27(2):205–211. doi: 10.1093/pubmed/fdi004. [DOI] [PubMed] [Google Scholar]
- 10.Theorell-Haglow J, Lindberg E, Janson C. What are the important risk factors for daytime sleepiness and fatigue in women? Sleep. 2006;29(6):751–757. doi: 10.1093/sleep/29.6.751. [DOI] [PubMed] [Google Scholar]
- 11.Arber S, Bote M, Meadows R. Gender and socioeconomic patterning of self-reported sleep problems in Britain. Social Science Medicine. 2009;68(2):281–289. doi: 10.1016/j.socscimed.2008.10.016. [DOI] [PubMed] [Google Scholar]
- 12.Chen YY, Kawachi I, Subramanian SV, Acevedo-Garcia D, Lee YJ. Can social factors explain sex differences in insomnia? Findings from a national survey in Taiwan. Journal of Epidemiol Community Health. 2005;59(6):488–494. doi: 10.1136/jech.2004.020511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kronholm E, Harma M, Hublin C, Aro AR, Partonen T. Self-reported sleep duration in Finnish general population. Journal of Sleep Research. 2006;15(3):276–290. doi: 10.1111/j.1365-2869.2006.00543.x. [DOI] [PubMed] [Google Scholar]
- 14.Schoenborn CA, Adams PE. Health behaviors of adults: United States, 2005–2007. Vital Health Stat. 2010;10(245):1–132. [PubMed] [Google Scholar]
- 15.Medina AM, Lederhos CL, Lillis TA. Sleep disruption and decline in marital satisfaction across the transition to parenthood. Families, Systems, and Health. 2009;27(2):153–160. doi: 10.1037/a0015762. [DOI] [PubMed] [Google Scholar]
- 16.Matthey S, Speyer J. Changes in unsettled infant sleep and maternal mood following admission to a parentcraft residential unit. Early Human Development. 2008;84(9):623–629. doi: 10.1016/j.earlhumdev.2008.04.003. [DOI] [PubMed] [Google Scholar]
- 17.Ohayon MM. Epidemiology of insomnia: what we know and what we still need to learn. Sleep Medicine Reviews. 2002;6(2):97–111. doi: 10.1053/smrv.2002.0186. [DOI] [PubMed] [Google Scholar]
- 18.Ohayon MM, Caulet M, Guilleminault C. How a general population perceives its sleep and how this relates to the complaint of insomnia. Sleep. 1997;20(9):715–723. doi: 10.1093/sleep/20.9.715. [DOI] [PubMed] [Google Scholar]
- 19.Grandner MA, Patel NP, Gehrman PR, et al. Who gets the best sleep? Ethnic and socioeconomic factors related to sleep complaints. Sleep Medicine. 2010;11(5):470–478. doi: 10.1016/j.sleep.2009.10.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Leger D, Guilleminault C, Dreyfus JP, Delahaye C, Paillard M. Prevalence of insomnia in a survey of 12, 778 adults in France. Journal of Sleep Research. 2000;9(1):35–42. doi: 10.1046/j.1365-2869.2000.00178.x. [DOI] [PubMed] [Google Scholar]
- 21.Ursin R, Bjorvatn B, Holsten F. Sleep duration, subjective sleep need, and sleep habits of 40- to 45-year-olds in the Hordaland Health Study. Sleep. 2005;28(10):1260–1269. doi: 10.1093/sleep/28.10.1260. [DOI] [PubMed] [Google Scholar]
- 22.Venn S, Arber S, Meadows R, Hislop J. The fourth shift: Exploring the gendered nature of sleep disruption among couples with children. The British Journal of Sociology. 2008;59(1):79–97. doi: 10.1111/j.1468-4446.2007.00183.x. [DOI] [PubMed] [Google Scholar]
- 23.McKnight-Eily LR, Liu Y, Perry GS, et al. Perceived insufficient rest or sleep among adults: United States, 2008. MMWR Morbidity and Mortality Weekly Report. 2009;58(42):1175–1179. [PubMed] [Google Scholar]