

BACKGROUND
Many U.S. adolescents of all races/ethnicities engage in multiple behaviors that increase their risk for poor reproductive health outcomes (Eaton, 20101; Everett Jones, Anderson, Lowry, & Conner, 2011; Ramisetty-Mikler & Ebama, 2011; Rutman, Park, Castor, Taualii, & Forquera, 2008). American Indian and Alaska Native (AI/AN) youth are disproportionately affected by poor reproductive health outcomes, including high rates of sexually transmitted diseases (STDs) and teen pregnancy. Peer-reviewed literature on AI/AN reproductive health issues is sparse and often not generalizable to all AI/AN because of small and geographically specific study populations. In the limited studies that have been conducted, some have shown high rates of STDs and teen pregnancy among AI/AN adolescents may result from a lack of familial support, a history of sexual and physical abuse, and early sexual debut (Palacios & Kennedy, 2010); alcohol and substance use and low and inconsistent condom use (Kaufman, 2006); and multiple sex partners (Marsiglia, Nieri, & Stiffman, 2006).
The Journal of American Indian and Alaska Native Mental Health Research disseminated the call for submissions for this special issue through its extensive formal and informal networks. The journal received 11 submissions; 9 of those are included in this special issue of the journal and 2 will appear in a later issue. No submission was rejected. Authors were instructed to attain necessary approvals prior to submission. Every author was assigned a mentor to help polish and finalize the manuscripts; the articles were reviewed by two external reviewers with expertise in the manuscripts’ subject areas.
We hope that this special journal issue on sexual risk behaviors and assets among AI/AN youth will lead to increased attention and efforts to meet the health care needs of Native youth and that the tracks that we leave will lead to the elimination of health disparities.
STD rates among AI/AN youth are among the highest in the country
In 2009, non-Hispanic AI/ANs had the second highest rates of STDs in the U.S.; compared to non-Hispanic White (NHW) youth, they were 4.5 times as likely to be diagnosed with chlamydia, more than three times as likely to be diagnosed with gonorrhea, and twice as likely to be diagnosed with primary or secondary syphilis (Centers for Disease Control and Prevention [CDC], 2010). Between 2000 and 2004, young people (15 to 24 years old) accounted for 68% of AI/AN chlamydia cases and 60% of AI/AN gonorrhea cases (Kaufman, 2007). For all U.S. races/ethnicities, female chlamydia rates are higher than those of males; the higher rate among females is mostly due to the far greater number of females screened for chlamydia (CDC, 2010). In 2009, chlamydia rates for NHW females were 3.2 times higher than the rates for NHW males; chlamydia rates for non-Hispanic AI/AN females were 3.8 times the rates for non-Hispanic AI/AN males (CDC, 2010). There are striking geographic differences in STD rates among AI/AN, which are especially pronounced among AI/AN adolescent females (see Figure 1).
Figure 1. Chlamydia Rates per 100,000 Population of 15- to 19-Year-Old Non-Hispanic AI/AN Females, in Indian Health Service (IHS) Areas*, IHS overall^, and the U.S.†, 2009 (CDC & IHS, 2012).

* IHS is divided into 12 administrative areas: Alaska (the state of Alaska); Aberdeen (Iowa, Nebraska, North Dakota, South Dakota); Albuquerque (Colorado, New Mexico); Bemidji (Michigan, Minnesota, Wisconsin); Billings (Montana, Wyoming); Nashville (states not included in the other areas); Navajo (the Navajo Nation); California (the state of California); Oklahoma City (Oklahoma, Kansas, Texas), Phoenix (parts of Arizona, Nevada, Utah); Portland (Idaho, Oregon, Washington);Tucson (southern Arizona).
^ IHS overall: denoted by “IHS” geographic region
† U.S.: denoted by “U.S.” geographic region
HIV cases among AI/ANs are undercounted because of low levels of HIV screening
AI/ANs—especially those living in rural areas—may be less likely than people of other races/ethnicities and urban AI/ANs to seek HIV testing because of concerns about confidentiality in small, close-knit communities, where someone seeking HIV testing may encounter a relative or an acquaintance at the local health clinic (CDC, 2007). Furthermore, there are considerable data limitations concerning HIV/AIDS among AI/ANs. For example, several states with large AI/AN populations have not consistently conducted or reported HIV surveillance data to the Centers for Disease Control and Prevention, and AI/ANs in some states are often racially misclassified (CDC, 2007). Although HIV/AIDS data for AI/ANs are sparse, in 2007, non-Hispanic AI/AN youth younger than 25 years accounted for 19% of new HIV/AIDS diagnoses among AI/ANs, compared to 14% nationwide (CDC, 2011). Because of late diagnosis and poor access to specialized care, AI/ANs have one of the lowest HIV/AIDS survival rates of any racial/ethnic group, with just one in four living more than three years after diagnosis (CDC, 2007).
The teen birth rate among AI/ANs is on the rise
After more than a decade of decline, the teen birth rate increased 12% among AI/ANs between 2005 and 2007—more than for any other race/ethnicity (Hamilton, 2010). Today, one fifth of non-Hispanic AI/AN girls give birth before their 20th birthday (Hamilton, 2010). As with STDs, there is considerable geographic variation in AI/AN teen pregnancy rates (Wingo, 2011; Figure 2.) Furthermore, many Native teens and women enter prenatal care late in pregnancy. In 2007, among those who delivered live births, 30.1% of Native mothers versus 16.2% of all mothers entered prenatal care late or had no prenatal care (Kaiser Family Foundation, 2007). In addition, Native mothers experience higher rates of low birth weight, preterm birth, and post-neonatal and infant mortality (including sudden infant death syndrome, or SIDS) than other mothers of other races/ethnicities (Alexander, Wingate, & Boulet, 2008; IHS, 2009).
Figure 2. Birth Rates per 1,000 Population among 15- to 19-Year-Old U.S. Females and U.S. AI/AN Females*, and by Geographic Region, 2007 (Wingo et al., 2011).
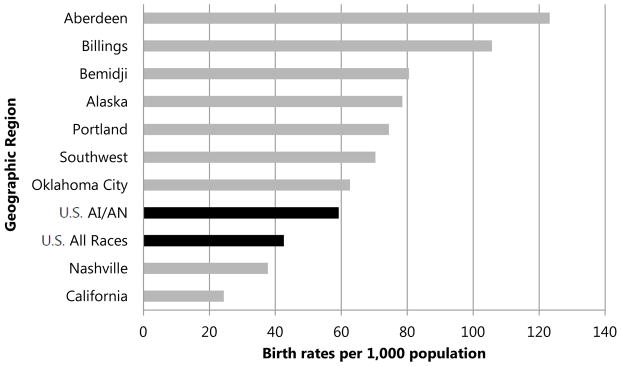
*AI/AN data include Hispanic AI/ANs and non-Hispanic AI/ANs.
AI/AN sexual minorities experience more physical and sexual abuse
Very few studies have been published on the health status of Native gay, lesbian, bisexual, transgender, and questioning youth (Barney, 2003). In one study, AI/AN boys who self-identified as gay/bisexual were significantly more likely than boys who self-identified as heterosexual to report sexual abuse (17.8% vs. 3.4%,p <. 001), physical abuse (26.7% vs. 9.6%, p < .001), and running away (23.3% vs. 13.4%, p < .001; Saewyc, Bearinger, Blum, & Resnick, 1998). In that same study, girls who self-identified as lesbian/bisexual were significantly more likely than self-reported heterosexual girls to report running away (32.0% vs. 21.4%, p < .05), and more often reported sexual abuse (42.4% vs. 31.1%, not significant [NS]) and physical abuse (51.5% vs. 33.6%, NS). Although some of the differences from the latter study were not significant, the proportion of AI/AN girls reporting sexual and physical abuse is striking (Saewyc et al., 1998). In a different study of 5,600 AI/AN male adolescents conducted in Minnesota, gay males were more likely than heterosexual males to report having been physically abused (17.2% vs. 7.5%, p < .01), sexually abused (13.3% vs. 2.4%, p < .001), depressed (35.1% vs. 14.0%, p < .001), and having attempted suicide (23.2% vs. 11.1%, p < .01); additionally, gay males were less likely to have had a physical examination (71.1% vs. 88.3%, p < .001; Barney, 2003).
AI/AN youth initiate alcohol and drug use early and use is high
Alcohol use is high among all youth in the U.S.; according to the Youth Risk Behavior Surveillance System (YRBSS), in 2009 74.0% of non-Hispanic AI/AN high school students had ever drunk alcohol, compared to 73.8% of White students, 67.6% of Black students, and 76.6% of Hispanic students (CDC, n.d.). Having ever used marijuana is also similar for youth of all races: 50.8% of non-Hispanic AI/AN students, 35.7% of White students, 41.2% of Black students, and 39.9% of Hispanic students (CDC, n.d.). However, compared to students of other races/ethnicities, non-Hispanic AI/AN students were more likely to initiate alcohol and drug use before age 13 (36.0% of non-Hispanic AI/AN students used alcohol before age 13 compared to 18.1% White students, 24.9% of Black students, and 27.1% of Hispanic students; 18.1% of non-Hispanic AI/AN students used marijuana before age 13 compared to 5.7% of White students, 10.2% of Black students, and 10.3% of Hispanic students; CDC, n.d.).
EFFORTS TO MEET THE NEEDS OF AI/AN YOUTH
Many efforts across the country are building on the assets and strengths of Native culture to improve the reproductive health of these youth; commonly, these efforts are locally or regionally focused. They exhibit a wide range of infrastructure and capacity to evaluate and disseminate successes beyond their respective communities. This special issue highlights some of these innovative interventions and promising research efforts to identify and address sexual risks and assets of Native youth.
The prevention efforts described in this special issue focus on identifying the priority reproductive health needs of Native youth, describing key strategies to develop effective and appropriate prevention interventions to reach this population, and developing messages that are youth-focused and culturally relevant to meet their unique and varied needs.
Identifying the Reproductive Health Needs of Youth
The Alaska Native Tribal Health Consortium conducted a series of community-based focus groups with Alaska Native youth to better understand the knowledge, attitudes, and beliefs of rural adolescents and communities regarding STD, HIV/AIDS, and unplanned pregnancy and to identify the best methods to educate and facilitate behavior change.
Sage Associates, Inc. surveyed Native girls from many different Tribes who were attending a residential school and who participated in BLING (BeLieving In Native Girls), a juvenile delinquency and HIV prevention curriculum. Sage found the participants to have considerable mental health and social concerns, including having poor critical thinking, coping, communication, and relationship skills; high levels of depression; high levels of current sexual activity and early sexual debut; and high rates of alcohol and drug use.
The Minnesota Indian Women’s Resource Center describes its program for Native girls who have been victims of human trafficking and commercial sexual exploitation. Although data are scarce, several studies strongly suggest that this population is significantly over-represented in the sex trade.
The Fort Peck Men’s Sexual Health Study is a community-based participatory research (CBPR) project that explores the extent of knowledge, attitudes, and beliefs about sex, intimate relationships, social/emotional health influence, and sexual and reproductive health among young men living on the Fort Peck Indian reservation in northeast Montana.
Designing Creative Strategies to Reach Youth
Project Red Talon describes CBPR activities used to identify and review technology-based sexual health interventions for youth and the participating Native youths’ recommendations for optimizing these applications.
The Wyoming Health Council describes its CBPR project for HIV prevention with a Native youth group on the Wind River Indian Reservation in Wyoming.
Developing Messages that Resonate with Youth
A group of Navajo health educators shares the community-based development process and foundational concepts of the Tools for Iina (Life) curriculum, designed for youth in grades four through six to address their health, relationships, identity, and sense of the future, using core concepts from Diné oral tradition.
Sacred Beginnings is a CBPR project designed to improve preconception health among Native adolescent women on a Northern Plains reservation. It examines the effectiveness of a culturally appropriate intervention developed by Tribal community members and elders.
The Circle of Life is an HIV prevention intervention designed for Native youth. The content is based on Native learning theories embodied by the medicine wheel and emphasizes skills development through symbols, stories, and ways of learning familiar to Native youth.
COMMUNITY INVOLVEMENT
One theme woven throughout the articles in this issue is the value of community input and involvement in research efforts. While the level and extent of community involvement varied by project, many used aspects of a community-based participatory research (CBPR) approach. CBPR—or Tribal participatory research (TPR)—approaches are seen as particularly respectful of research partnerships with Tribes; using TPR, research can be responsive to community needs, culturally appropriate, and strengths-based while paying heed to past transgressions against Tribes on the part of researchers (Thomas, Rosa, Forcehimes, & Donovan, 2011). Some important tenants of applying CBPR/TPR approaches in Tribal settings include: acknowledging historical experience with research and researchers, recognizing Tribal sovereignty, differentiating between Tribal and community membership, understanding Tribal diversity and its implications, plan for extended timelines, recognize key gatekeepers, prepare for leadership turnover, interpret data within the cultural context, and utilize Indigenous ways of knowing (LaVeaux & Christopher, 2009).
CONCLUSIONS/RECOMMENDATION
The editors and authors of this special issue are proud to share these innovative efforts to address adolescent reproductive health from across Indian Country. More support, training, technical assistance, and capacity building are needed to engage the community in meaningful ways, develop and implement behavioral interventions, assess the effectiveness of interventions through evaluation, and disseminate the findings to others who may benefit from them.
Other reproductive health interventions and research projects are taking place across the country to address the reproductive health needs of Native youth. Some of these, such as RESPECT, Native Voices, Native Students Together Against Negative Decisions (STAND), and It’s Your Game … Keep it Real, are evidence-based interventions that are currently being adapted for AI/AN youth. In the small and close-knit community of researchers and public health practitioners who work with Native youth, there is already a substantial amount of inter-Tribal dissemination, sharing, and informal technical assistance. This form of sharing and exchange is powerful despite being constrained by resources and data. To build a stronger foundation for this work, we need improved data collection and reporting among AI/ANs and greater inclusion of AI/ANs in national, state, and county data collection systems. Establishing an evidence base—and rethinking what evidence means for AI/ANs—is another crucial step toward promoting programs that work for this population. Although AI/ANs make up a small percentage of the U.S. population, they are disproportionately affected by health disparities.
Our hope is that the research and prevention efforts described in this special journal issue will lead to increased attention and efforts to meet the health care needs of Native youth and that the tracks that we leave will lead to the elimination of health disparities.
Footnotes
Race/ethnicity data from the 2009 Youth Risk Behavior Survey are presented only for non-Hispanic Black, non-Hispanic White, and Hispanic students (of any race); the numbers of students from other racial/ethnic groups were too small for meaningful analysis.
DISCLAIMER
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Contributor Information
Lori de Ravello, Email: leb8@cdc.gov, Centers for Disease Control and Prevention, Division of Reproductive Health, Indian Health Service, National STD Program.
Scott Tulloch, Email: sdt2@cdc.gov, Centers for Disease Control and Prevention, Division of STD Prevention, Indian Health Service, National STD Program.
Melanie Taylor, Email: smdt7@cdc.gov, Centers for Disease Control and Prevention, Division of STD Prevention, Indian Health Service, National STD Program.
References
- Alexander GR, Wingate MS, Boulet S. Pregnancy outcomes of American Indians: Contrasts among regions and with other ethnic groups. Maternal and Child Health Journal. 2008;12(Suppl 1):S5–S11. doi: 10.1007/s10995-007-0295-z. [DOI] [PubMed] [Google Scholar]
- Barney DD. Health risk-factors for gay American Indian and Alaska Native adolescent males. Journal of Homosexuality. 2003;46(1/2):137–157. doi: 10.1300/J082v46n01_04. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention (CDC) 1991–2009 High School Youth Risk Behavior Survey Data. Atlanta, GA: Author; n.d. Retrieved from http://apps.nccd.cdc.gov/youthonline. [Google Scholar]
- CDC. HIV/AIDS among American Indians and Alaska Natives. (Fact Sheet) 2007 Retrieved from http://www.cdc.gov/hiv/resources/factsheets/PDF/aian.pdf.
- CDC. Diagnoses of HIV infection and AIDS in the United States and dependent areas, 2009. HIV Surveillance Report. 2011;21 Retrieved from http://www.cdc.gov/hiv/surveillance/resources/reports/2009report. [Google Scholar]
- CDC Division of STD Prevention. Sexually transmitted disease surveillance 2009 (Tables 11B, 21B, 34B) Atlanta: U.S. Department of Health and Human Services; 2010. Retrieved from http://www.cdc.gov/std/stats09/surv2009-Complete.pdf. [Google Scholar]
- CDC & Indian Health Service. Indian health surveillance report—Sexually transmitted diseases 2009. Atlanta, GA: U.S. Department of Health and Human Services; 2012. Retrieved from http://www.cdc.gov/std/stats/IHS/default.htm. [Google Scholar]
- Eaton DK, Kann L, Kinchen S, Shanklin S, Ross J, Hawkins J, Wechsler H. Youth Risk Behavior Surveillance—United States, 2009. Morbidity and Mortality Weekly Report—Surveillance Summaries. 2010;59(SS-5) Retrieved from http://www.cdc.gov/mmwr/pdf/ss/ss5905.pdf. [PubMed] [Google Scholar]
- Everett Jones S, Anderson K, Lowry R, Conner H. Risks to health among American/Indian Alaska Native high school students in the United States. Preventing Chronic Disease. 2011;8(4):A76. [PMC free article] [PubMed] [Google Scholar]
- Hamilton BE, Martin JA, Ventura SJ. Births: Preliminary data for 2009. National Vital Statistics Reports. 2010;59(3) Retrieved from http://www.cdc.gov/nchs/data/nvsr/nvsr59/nvsr59_03.pdf. [PubMed] [Google Scholar]
- Indian Health Service. Trends in Indian health. Rockville, MD: Department of Health and Human Services; 2009. 2002–2003. [Google Scholar]
- Kaiser Family Foundation. Putting women’s health care disparities on the map: Late initiation of or no prenatal care, by state and race/ethnicity, 2007. 2007 [Interactive database]. Retrieved from http://statehealthfacts.org/comparereport.jsp?rep=34&cat=15.
- Kaufman CE, Desserich J, Big Crow CK, Holy Rock B, Keane E, Mitchell CM. Culture, context, and sexual risk among Northern Plains American Indian youth. Social Science & Medicine. 2007a;64:2152–2164. doi: 10.1016/j.socscimed.2007.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaufman CE, Shelby L, Mosure D, Marrazzo J, Wong D, de Ravello L, Cheek JE. Within the hidden epidemic: Sexually transmitted diseases and HIV/AIDS among American Indians and Alaska Natives. Sexually Transmitted Diseases. 2007b;34:767–777. doi: 10.1097/01.olq.0000260915.64098.cb. [DOI] [PubMed] [Google Scholar]
- LaVeaux D, Christopher S. Contextualizing CBPR: key principles of CBPR meet the Indigenous research context. Pimatisiwin. 2009;7(1):1–16. Retrieved from http://www.pimatisiwin.com/online/ [PMC free article] [PubMed] [Google Scholar]
- Marsiglia FF, Nieri T, Stiffman AR. HIV/AIDS protective factors among urban American Indian youths. Journal of Health Care for the Poor & Underserved. 2006;17:745–758. doi: 10.1353/hpu.2006.0128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Palacios J, Kennedy HP. Reflections of Native American teen mothers. Journal of Obstetric, Gynecologic, & Neonatal Nursing. 2010;39(4):425–434. doi: 10.1111/j.1552-6909.2010.01149.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rutman S, Park A, Castor M, Taualii M, Forquera R. Urban American Indian and Alaska Native youth: Youth Risk Behavior Survey 1997–2003. Maternal and Child Health Journal. 2008;12(Suppl 1):76–81. doi: 10.1007/s10995-008-0351-3. [DOI] [PubMed] [Google Scholar]
- Saewyc EM, Skay CL, Bearinger LH, Blum RW, Resnick MD. Sexual orientation, sexual behaviors, and pregnancy among American Indian adolescents. Journal of Adolescent Health. 1998;23:238–247. doi: 10.1016/S1054-139X(98)00016-0. [DOI] [PubMed] [Google Scholar]
- Ramisetty-Mikler S, Ebama MS. Alcohol/drug exposure, HIV-related sexual risk among urban American Indian and Alaska Native youth: Evidence from a national survey. Journal of School Health. 2011;81(11):671–679. doi: 10.1111/j.1746-1561.2011.00643.x. [DOI] [PubMed] [Google Scholar]
- Thomas LR, Rosa C, Forcehimes A, Donovan DM. Research partnerships between academic institutions and American Indian and Alaska Native Tribes and organizations: Effective strategies and lessons learned in a multisite clinical trials network study. American Journal of Drug and Alcohol Abuse. 2011;37:333–338. doi: 10.3109/00952990.2011.596976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wingo PA, Lesesne CA, Smith RA, de Ravello L, Espey DK, Arambula Solomon TG, Thierry J. Trends, geographic variation in trends and characteristics of teen childbearing among American Indians and Alaska Natives, 1990–2007. Maternal and Child Health Journal. 2011 doi: 10.1007/s10995-011-0924-4. Advance online publication. [DOI] [PubMed] [Google Scholar]