

Abstract
Background:
With the report of high prevalence rate of Vitamin D deficiency in the literature since the 1980s, the condition can be considered an epidemic in Saudi Arabia. However, no specific steps have been taken by the Ministry of Health to tackle the problem. Moreover, little is known about general practitioners’ (GPs) knowledge, attitude, and practice (KAP) of Vitamin D supplementation for infants.
Objectives:
To measure the KAP of GPs, of Vitamin D supplementation for infants in Dammam, Saudi Arabia.
Materials and Methods:
This was a cross-sectional study of GPs practicing in primary healthcare centers in the Dammam area of Saudi Arabia. All the 110 GPs working in primary health centers (PHCs) in Dammam were invited to participate in the study. Data was collected with the help of a self-administered questionnaire. Data was analyzed using SPSS 20.0. Statistical analysis included descriptive analysis of all the variables, expressed as the mean (standard deviation [SD]) or the median if not normally distributed.
Results:
Ninety-three GPs working in the Dammam area participated in the study. Thirty percent had excellent knowledge of Vitamin D. Ninety two percent had a positive attitude toward Vitamin D supplementation and sixty percent regularly prescribed Vitamin D supplementation for infants.
Conclusion:
The majority of GPs had a positive attitude toward Vitamin D supplementation for infants. However, their knowledge and practice need improvement.
Keywords: Attitude, general practitioners, infants, knowledge, practice, Vitamin D supplementation
INTRODUCTION
Vitamin D deficiency has emerged as a major health problem in Saudi Arabia in both genders[1,2] and all age groups.[3,4,5,6] The reported prevalence in patients visiting primary health care centers (PHCs) is between 28% in healthy adult males, 80% in healthy school children, and 100% in young adult females.[1,2,3,4,5,6] This reported wide variability in the prevalence could be related to the use of different cut-off points for the definition of Vitamin D deficiency, or the differences in the methods used in analyzing the blood samples for Vitamin D levels.
Related literature since 1983 indicates that the problem of Vitamin D deficiency in Saudi Arabia is not recent.[7,8] In articles published in the last few years to highlight the size of the problem,[1,2,3,4,5,6] several factors have been identified as contributors to the low level of Vitamin D in the Saudi population. These include the religious practice whereby women wear Hijab, limited exposure to the sun in spite of abundant sunlight all year round, and poor dietary intake.[2,4,5]
The relationship between Vitamin D, rickets, osteomalacia and osteoporosis is well established, but Vitamin D has recently been identified as an immunomodulator that could be linked to such conditions as bronchial asthma, atopic dermatitis and food allergy,[9] type 1 diabetes mellitus,[10,11] and an increased susceptibility to infections.[12]
In 2003, the American Academy of Pediatrics recommended giving supplements of 200 IU/day of Vitamin D to all infants starting in the first 2 months after birth as a primary means of preventing rickets.[13] In 2008, the policy was revised and the dose increased to 400 IU/day starting in the first few days of life to continue through childhood to adolescence.[14] Several European countries have different recommendations and guidelines for Vitamin D supplementation.[15] Despite these widely advocated recommendations, few studies have addressed the practice of health care workers with regard to Vitamin D supplementation for infants. A study of military pediatricians and family physicians[16] found that pediatricians were 40% more likely than family physicians to prescribe Vitamin D to exclusively breast-fed infants, and the most common reason for not prescribing Vitamin D was the belief that infants were adequately exposed to sunlight. In this study, 63% of the family physicians prescribed Vitamin D to exclusively breast-fed infants compared to 89% of the pediatricians. In addition, only 29% of the family physicians gave supplements to breast- and bottle-fed infants compared to 66% of the pediatricians. A similar finding was reported in a study of pediatricians and family physicians in Connecticut,[17] USA, where 88.6% of the pediatricians reported counseling parents about vitamin D for infants compared to 52.3% of the family physicians. Another American survey of 155 pediatric primary health care providers published in 2004, showed that 47.7% of the surveyed physicians prescribed supplementation for exclusively breast-fed infants. Of those physicians who prescribed supplementation, 27.1% recommended it for all infants (both breast- and bottle-fed). In this study, females, pediatricians, and those who had 21 or more years of experience were more likely to recommend Vitamin D.[18]
In Saudi Arabia, there are no recommendations on vitamin D supplementation by the Ministry of Health (MOH). Consequently, the practice of giving infants supplements of Vitamin D is left to the health institutions, and therefore varies from one institution to another. Furthermore, no studies were found that address the practice of giving infants in Saudi Arabia supplements of Vitamin D.
The objective of this study was to measure knowledge, attitude and practice (KAP) of general practitioners (GPs) working in PHC in the Dammam area, towards Vitamin D supplementation for infants.
MATERIALS AND METHODS
This was a cross-sectional study of GPs working in the MOH PHCs in Dammam, Saudi Arabia. The total number of GPs working in Dammam PHCs during the period of data collection (March 2014) was 110, and all were invited to participate in the study. A 10-min self-administered 2-part questionnaire developed by the researchers after discussions with experts and a literature review was used to achieve the objective of the study. The first part covered demographic data that included: Age, gender, marital status, number of children, nationality, place of graduation, number of years since graduation, number of years of practice as a GP, and previous work experience in institutions other than PHC. The second part had questions on KAP related to Vitamin D supplementation. The participants were asked to state their level of agreement with 20 neutral sentences by choosing from 3 responses (agree, neutral, disagree). For the questions on practice, responses of neutral or disagree were regarded as a negative response.
The questionnaire was pilot tested in 20 GPs working in the neighboring Al Khobar area. Some questions were modified after the analysis of the pilot testing. Before the final form was prepared, the questionnaire was revised after an assessment for content validity by two experts in the field.
The main outcome of the study was to determine GPs’ KAP about Vitamin D supplementation to infants. A set of questions was used to explore GPs information on the importance of Vitamin D, their perception of the role of Vitamin D in preventing disease, their practice of prescribing Vitamin D for infants and whether they asked parents about their compliance with giving their infants the Vitamin D supplements.
All collected questionnaires were screened for completeness of information. The collected data was managed, coded and entered to SPSS 20.0 for Macintosh (SPSS Inc., Chicago, IL, USA; 2010) and was checked for any abnormality before analysis.
Statistical analysis included descriptive analysis of all the variables, expressed as the mean (standard deviation [SD]) or the median if not normally distributed. A knowledge score was calculated by combining the results of the 11 knowledge questions (3 points were given for each correct answer giving an optimum score of 33 to denote that all knowledge questions had been answered correctly). The mean and SD for the knowledge score were calculated. The responses were re-coded as the following: Score 30–33 were regarded as excellent knowledge (mean + 2SD), scores 27–29 were regarded as good knowledge (mean + 1SD), scores 24–26 (mean − 1SD) were regarded as fair knowledge, and scores <24 (mean − 2SD) were regarded as poor knowledge. Practice score was calculated by combining the results of the questions on practice. To check for correlation between different study variables and the outcomes of the study, bivariate correlation was used for categorical variables, and independent t-test was used for continuous variables. In addition, multivariate regression analysis of knowledge and practice scores (as dependent variables) and all demographic variables (as independent variables) was done. This was important to exclude any residual confounding elements arising during bivariate analysis.
RESULTS
Of the 110 GPs who were working in Dammam PHC during the study period, 99 answered the questionnaire. Six questionnaires were excluded from the analysis for being incomplete (missing data more than 30%). The overall response rate was 84.5%.
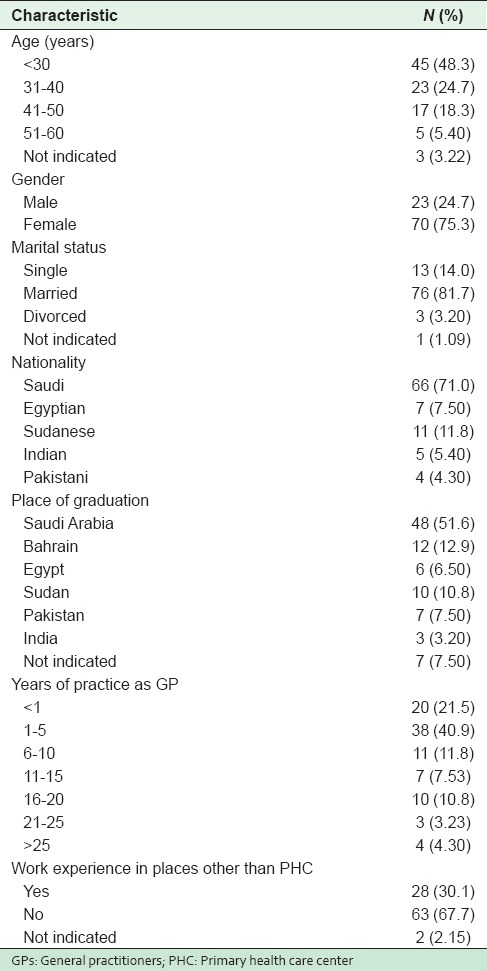
The mean age of participants was 33.4 (SD 5.5) years, and the majority were females (74%). A large proportion was married (81%) with a median number of children of 2. Seventy-three percent of doctors were Saudi and 55.8% had graduated from Saudi Arabian Universities. The mean duration of practice as GP was 6.64 years (SD 1.6). Around 30% of the participants had previous work experience in places other than PHCs [Table 1].
Table 1.
Demographic characteristics of GPs participating in the survey
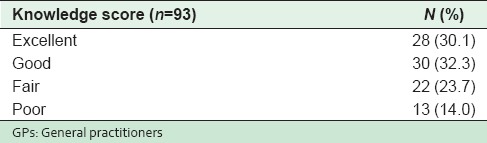
The mean and SD for the knowledge score was: Mean = 27, SD = 3. The analysis showed that 30% of the GPs had excellent knowledge, 32% had good knowledge, 23% had fair knowledge, and 14% had poor knowledge [Table 2].
Table 2.
Frequency distribution of knowledge score of GPs regarding Vitamin D supplementation
The attitudes of GPs were generally positive; 92.2% believed that Vitamin D supplementation was important for infants’ health.
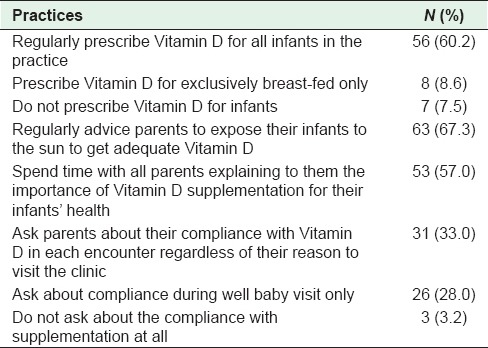
Of the 93 physicians surveyed, 56 physicians (60.2%) regularly prescribed Vitamin D supplementation for all infants, 8 physicians (8.6%) recommended supplementation for exclusively breast-fed infants only, and 7 physicians (7.5%) did not recommend Vitamin D to infants in their practice. Twenty-two GPs (23.6%) did not respond to the questions on the practice of supplementation. On the question of advice given to parents, 63% of physicians stated that they regularly advised parents to expose their infants to the sun in order for them to get adequate Vitamin D. In addition, 53% stated that they spent time explaining to all parents the importance of Vitamin D supplementation for their infants’ health. On the question of follow-up of infants, 33.3% of the physicians stated that they asked parents about their compliance with giving supplements of Vitamin D at each encounter regardless of the reason for the visit to the clinic, 28% asked about compliance during “well baby” visits only, and 3.2% stated that they did not ask about compliance with supplementation at all [Table 3].
Table 3.
Practices of GPs regarding Vitamin D supplementation
There was no significant relationship between knowledge and practice scores, with age, gender, marital status, nationality, place of graduation, years of practice as GP or previous work experience in places other than PHC (P > 0.05).
In addition, the knowledge and practice scores were regressed as dependent variables, while all other variables were entered as independent variables. The model did not include any variable as significant (P > 0.05).
DISCUSSION
The response rate in the survey was excellent (84.5%). This high rate is important for the reduction of nonresponse bias since the objective of the survey was to measure KAP of physicians.
More than half of the participants in this study had either excellent or good knowledge scores. This could help in the future design of programs to change KAP of GPs by providing a general idea of the current situation.
Of the physicians surveyed, more than half prescribed Vitamin D supplementation for all infants. In addition, just a minority of GPs prescribed Vitamin D for exclusively breast-fed infants only. This result was not comparable to the reported prevalence in other studies. In the American study[18] on the prescribing pattern in Las Vegas, only about one-third (27.1%) of the physicians recommended supplementation for all infants (both breast- and bottle-fed). The study of Military physicians[16] showed a similar finding in which 29% of family physicians advised supplements for both breast- and bottle-fed infants.
These figures show that GPs in Saudi Arabia were more likely to prescribe Vitamin D supplementation for both breast- and bottle-fed infants. This could be due to the high prevalence of Vitamin D deficiency in Saudi Arabia and the higher emphasis put on using Vitamin D supplementation to ameliorate the effect of low exposure to sunlight. In addition, the positive attitude of almost all of the surveyed physicians regarding Vitamin D supplementation could be a factor in the higher rates of prescribing Vitamin D.
There are some limitations to the study. These include small sample size, which might be a reason for the absence of a significant association between demographic variable and knowledge and practice scores. Another limitation is that large percentage of GPs did not respond to the questions on their practice. The reason for this high nonresponse to a specific section of the questionnaire is not clear. It is unlikely to be related to questionnaire design, as we did not have this problem in the pilot study. In addition, the survey was anonymous so participants could not have been worried about any adverse consequences for admitting their true practice. Whatever the reason for their nonresponse, this could have a negative impact on the accuracy of determining prescribing patterns.
Finally, one of the problems that GPs caring for infants in Saudi Arabia may face is that there is no specific recommendation from the Saudi MOH on Vitamin D supplementation. Besides, different pediatric societies have different practice guidelines for Vitamin D supplementation,[14,15] and none of these recommendations has been endorsed by the MOH. The consequence of this is the variation in GPs’ practice as observed in this study. The Saudi MOH should establish its own clinical practice guidelines or endorse one of the existing guidelines for use, to ensure that GPs follow the latest, evidence-based practice and that all health institutions maintain the same standards of care.
CONCLUSIONS
This study is the first to provide data on GPs’ KAP of supplementing infants with Vitamin D in Saudi Arabia. Around one-third of GPs had excellent knowledge of Vitamin D supplementation and almost all of them had a positive attitude toward supplementation. The practice of giving infants supplements of Vitamin D was suboptimal, given the high prevalence rate of Vitamin D deficiency. Consequently, it is important for the MOH to develop clinical practice guidelines to improve the practice of supplementation and to maintain proper standards of care.
Financial support and sponsorship
Nil
Conflict of interest
There are no conflicts of interest.
REFERENCES
- 1.Naeem Z, Almohaimeed A, Sharaf FK, Ismail H, Shaukat F, Inam SB. Vitamin D status among population of Qassim region, Saudi Arabia. Int J Health Sci (Qassim) 2011;5:116–24. [PMC free article] [PubMed] [Google Scholar]
- 2.Al-Mogbel ES. Vitamin D status among Adult Saudi females visiting primary health care clinics. Int J Health Sci (Qassim) 2012;6:116–26. doi: 10.12816/0005987. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mansour MM, Alhadidi KM. Vitamin D deficiency in children living in Jeddah, Saudi Arabia. Indian J Endocrinol Metab. 2012;16:263–9. doi: 10.4103/2230-8210.93746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ardawi MS, Sibiany AM, Bakhsh TM, Qari MH, Maimani AA. High prevalence of vitamin D deficiency among healthy Saudi Arabian men: Relationship to bone mineral density, parathyroid hormone, bone turnover markers, and lifestyle factors. Osteoporos Int. 2012;23:675–86. doi: 10.1007/s00198-011-1606-1. [DOI] [PubMed] [Google Scholar]
- 5.Al-Ghamdi MA, Lanham-New SA, Kahn JA. Differences in vitamin D status and calcium metabolism in Saudi Arabian boys and girls aged 6 to 18 years: Effects of age, gender, extent of veiling and physical activity with concomitant implications for bone health. Public Health Nutr. 2012;15:1845–53. doi: 10.1017/S1368980011003612. [DOI] [PubMed] [Google Scholar]
- 6.Sadat-Ali M, AlElq A, Al-Turki H, Al-Mulhim F, Al-Ali A. Vitamin D levels in healthy men in eastern Saudi Arabia. Ann Saudi Med. 2009;29:378–82. doi: 10.4103/0256-4947.55168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sedrani SH, Elidrissy AW, El Arabi KM. Sunlight and vitamin D status in normal Saudi subjects. Am J Clin Nutr. 1983;38:129–32. doi: 10.1093/ajcn/38.1.129. [DOI] [PubMed] [Google Scholar]
- 8.Fonseca V, Tongia R, el-Hazmi M, Abu-Aisha H. Exposure to sunlight and vitamin D deficiency in Saudi Arabian women. Postgrad Med J. 1984;60:589–91. doi: 10.1136/pgmj.60.707.589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Searing DA, Leung DY. Vitamin D in atopic dermatitis, asthma and allergic diseases. Immunol Allergy Clin North Am. 2010;30:397–409. doi: 10.1016/j.iac.2010.05.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Alpert PT, Shaikh U. The effects of vitamin D deficiency and insufficiency on the endocrine and paracrine systems. Biol Res Nurs. 2007;9:117–29. doi: 10.1177/1099800407308057. [DOI] [PubMed] [Google Scholar]
- 11.Takiishi T, Gysemans C, Bouillon R, Mathieu C. Vitamin D and diabetes. Endocrinol Metab Clin North Am. 2010;39:419–46. doi: 10.1016/j.ecl.2010.02.013. [DOI] [PubMed] [Google Scholar]
- 12.Chesney RW. Vitamin D and The magic mountain: The anti-infectious role of the vitamin. J Pediatr. 2010;156:698–703. doi: 10.1016/j.jpeds.2010.02.002. [DOI] [PubMed] [Google Scholar]
- 13.Gartner LM, Greer FR. Section on Breastfeeding and Committee on Nutrition. American academy of pediatrics. Prevention of rickets and vitamin D deficiency: New guidelines for vitamin D intake. Pediatrics. 2003;111:908–10. doi: 10.1542/peds.111.4.908. [DOI] [PubMed] [Google Scholar]
- 14.Wagner CL, Greer FR. American Academy of Pediatrics Section on Breastfeeding, American Academy of Pediatrics Committee on Nutrition. Prevention of rickets and vitamin D deficiency in infants, children, and adolescents. Pediatrics. 2008;122:1142–52. doi: 10.1542/peds.2008-1862. [DOI] [PubMed] [Google Scholar]
- 15.Dratva J, Merten S, Ackermann-Liebrich U. Vitamin D supplementation in Swiss infants. Swiss Med Wkly. 2006;136:473–81. doi: 10.4414/smw.2006.11456. [DOI] [PubMed] [Google Scholar]
- 16.Sherman EM, Svec RV. Barriers to vitamin D supplementation among military physicians. Mil Med. 2009;174:302–7. doi: 10.7205/milmed-d-01-4708. [DOI] [PubMed] [Google Scholar]
- 17.Silk H, Thiede S, Trojian T. Counseling about vitamin D supplementation for infants: Results of a survey of pediatric and family medicine physicians in Connecticut. Conn Med. 2007;71:133–7. [PubMed] [Google Scholar]
- 18.Shaikh U, Alpert PT. Practices of vitamin D recommendation in Las Vegas, Nevada. J Hum Lact. 2004;20:56–61. doi: 10.1177/0890334403260617. [DOI] [PubMed] [Google Scholar]