

Abstract
Selecting the proper treatment strategy for locally advanced lung cancer, such as T4 tumors, is difficult. Therefore, obtaining an accurate diagnosis of T4 tumors is required. It can be difficult to determine whether the tumor invades adjacent structures. We describe the case of a patient easily diagnosed to be without aortic invasion using cine magnetic resonance imaging (MRI). We herein report the case of an 80-year-old male who presented a lung tumor. The transbronchial lung washing cytology findings were consistent with those of adenocarcinoma. In addition, the computed tomography findings indicated suspected aortic invasion of the lung tumor, as the mass girdled the descending aorta beyond 120° adjoining at a length of 10 cm. However, cine MRI display clearly demonstrated a clear area of isolation between the aorta and lung tissue based on differences in the heart rhythm from the patient's respiratory movements. Therefore, the lesion was clinically diagnosed as a stage IIB (T3N0M0) tumor. Radiation was administered due to the patient's advanced age and comorbidities such as chronic obstructive pulmonary disease. He remains alive without disease progression 6 months after the therapy. Our findings, therefore, indicate the usefulness of easily diagnosing the absence of aortic invasion in patients with lung cancer using cine MRI without the need for a special software program.
Key Words: Cine magnetic resonance imaging, Diagnosis, Aorta, Invasion, Lung cancer
Introduction
Locally advanced lung cancer, such as T4 tumors, has a significantly worse prognosis than earlier-stage disease, and selecting the proper treatment strategy for these tumors is difficult [1]. Therefore, obtaining an accurate diagnosis of T4 tumors is required [2]. It can be difficult to determine whether the tumor invades adjacent structures, especially the aorta, in clinical practice due to limitations in the diagnostic capability of usual computed tomography (CT) and magnetic resonance imaging (MRI) examinations. We herein describe the case of a patient easily diagnosed to be without aortic invasion using cine MRI.
Case Presentation
The patient, an 80-year-old male presenting with a left lung tumor during the course of follow-up for chronic obstructive pulmonary disease (COPD), was referred to our hospital for an evaluation of an abnormal shadow observed on a chest X-ray film. CT showed a tumor in the left lower lobe beside the descending aorta. The transbronchial lung washing cytology findings were consistent with a diagnosis of adenocarcinoma. The preoperative CT findings indicated suspected aortic invasion of the lung tumor, as the mass girdled the aorta beyond 120° adjoining at a length of 10 cm (fig. 1). However, cine MR imaging display clearly demonstrated a clear area of isolation between the aorta and lung tissue, with differences in the heart rhythm from the patient's respiratory movements (online supplementary video). Therefore, the lesion was clinically diagnosed to be at stage IIB (T3N0M0). Radiation was administered due to the patient's advanced age and comorbidities such as COPD. He currently remains alive without disease progression 6 months after therapy.
Fig. 1.
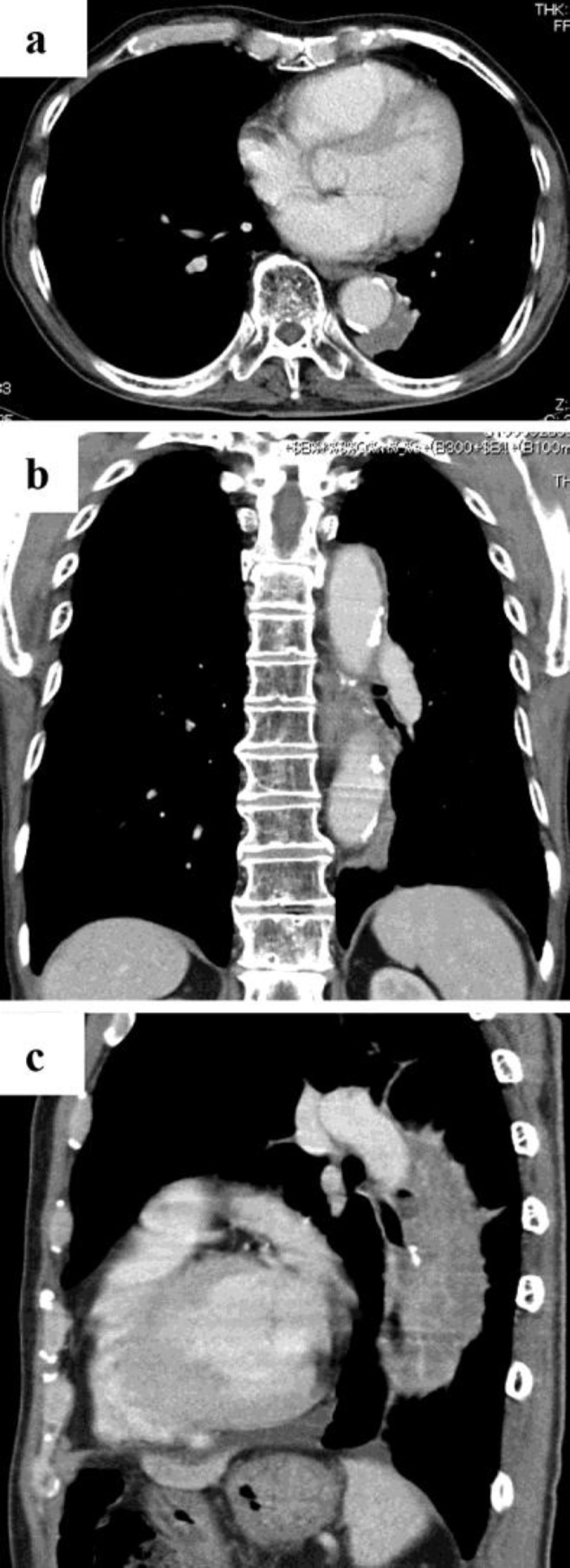
a A chest CT shows a tumor in the left lower lobe. b, c Aortic invasion of the left lung tumor was suspected.
Discussion
Most physicians suspect aortic invasion based on CT findings, including cancerous lesions that are both wide and long, abutting the descending aorta without a clear fat plane between the aorta and cancer mass. In fact, Glazer et al. [3] reported 4 (out of 8) cases of mediastinal invasion (tumors contacting more than 90° of the aortic circumference) that was not technically resectable. This interpretation suggests the difficulty of providing treatment due to contraindications for surgery and the use of anti-angiogenic therapy. However, it is difficult to determine whether the tumor invades the aorta in clinical practice because the diagnostic capability of usual CT and MR imaging examinations is limited [4]. Furthermore, there are differences in thinking among different professionals, for example surgeons, radiation oncologists and medical oncologists, because of the emphasis on radiological findings relevant for each specialty [4]. However, the fact remains that accurate staging is required to select appropriate treatment. Recently, we also experienced a similar case in which the patient had a 9-cm cancerous lesion in the left lower lobe that was both wide and long, abutting the descending aorta. No clear fat plane was visible between the aorta and cancer mass, although an intraoperative assessment showed the resectability of the lesion, with the absence of invasion. Left lower lobectomy combined with the resection of 6–8 ribs and partial resection of the left upper lobe plus standard lymph node dissection without transfusion was performed [2]. CT may have overestimated the lesion because the large left lower mass was displaced dorsally by the effects of gravity and aortic invasion. Cine MRI (suppl. video) does not provide a consecutive movie, but rather offers several stationary pictures without the use of a special software program. However, there is fortunately a gap between the cardiac motion and respiratory movements. We recently performed complete left upper lobectomy safely in another surgical case after obtaining confirmation of the lack of aortic invasion using this method.
Physicians should pay attention to the potential of the absence of aortic invasion, even if the angle in contact with the tumor indicates a wide field of view without lymph node metastasis, in order to provide a chance for a cure. When considered in combination with the use of antiangiogenic therapy, this diagnostic tool is easy to apply and has broad utility among medical oncologists to avoid the risk of hemosputum in the great vessels [5]. Our findings, therefore, indicate the usefulness of easily diagnosing the absence of aortic invasion in patients with lung cancer using cine MRI without the need for a special software program.
Statement of Ethics
Informed consent was obtained from the patient for the use of his data in the analyses described herein.
Disclosure Statement
None declared.
Supplementary Material
Supplemental Video
References
- 1.Uramoto H, Shimokawa H, Hanagiri T, Ichiki Y, Tanaka F. Factors predicting the surgical outcome in patients with T3/4 lung cancer. Surg Today. 2014;44:2249–2254. doi: 10.1007/s00595-014-0861-0. [DOI] [PubMed] [Google Scholar]
- 2.Uramoto H, Kinoshita H. Careful diagnosis of aortic invasion in patients with lung cancer using modern diagnostic imaging. Asian Pac J Cancer Prev. 2015;16:2105. doi: 10.7314/apjcp.2015.16.5.2105. [DOI] [PubMed] [Google Scholar]
- 3.Glazer HS, Kaiser LR, Anderson DJ, Molina PL, Emami B, Roper CL, Sagel SS. Indeterminate mediastinal invasion in bronchogenic carcinoma: CT evaluation. Radiology. 1989;173:37–42. doi: 10.1148/radiology.173.1.2781028. [DOI] [PubMed] [Google Scholar]
- 4.Munden RF, Swisher SS, Stevens CW, Stewart DJ. Imaging of the patient with non-small cell lung cancer. Radiology. 2005;237:803–818. doi: 10.1148/radiol.2373040966. [DOI] [PubMed] [Google Scholar]
- 5.Uramoto H, Yamada S, Tanaka F. Angiogenesis of lung cancer utilizes existing blood vessels rather than developing new vessels using signals from carcinogenesis. Anticancer Res. 2013;33:1913–1916. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental Video