

Abstract
Background
One of the primary reasons for referral for reflux testing is to correlate reflux events with symptoms such as cough. Adult studies have suggested that symptom recording is flawed and pediatricians feel this is an even more significant problem as there may be errors in both parental and patient report. We hypothesize that intraesophageal pressure recording (IEPR) provides an objective method to identify coughs during reflux testing in children.
Methods
We recruited 20 children undergoing pH-MII testing for the evaluation of cough. We placed simultaneous intraesophageal pressure and pH-MII catheters. Tracings were blindly scored by 2 observers without knowledge of patient/parent symptom report. After the blinded scoring, patient/parent report of symptoms was recorded.
Results
94% of all coughs were detected by IEPR and only 48% of all coughs were reported by patients/parents. The mean time from the IEPR cough to the patient/parent cough was 11±16 seconds. Using IEPR as the gold standard for the detection of cough, the sensitivity of patient report for the detection of cough is 46%. Using varying symptom windows because of the increased precision of IEPR, the number of patients with a positive symptom index could be reduced from 30% down to 0%, preventing children from being falsely categorized as having reflux-related lung disease.
Conclusions
Parental and patient symptom recording in children is inadequate for making the diagnosis of reflux-related lung disease. If patients undergo pH-MII testing for reflux-related cough, IEPR should become the new standard by which to correlate reflux with cough.
Introduction
The association between gastroesophageal reflux and cough is not clear. Even though some patients clearly benefit from anti-reflux therapy, many others do not, leading often to treatments that have potential significant side effects (1–6). Therefore finding tools to better select those patients with reflux-associated symptoms will have a major impact on clinical care. Currently to correlate reflux events with cough, the patient/parent record in a log the occurrence of symptoms while the patient is undergoing reflux testing either with ph-metry or multichannel intraluminal impedance testing (pH-MII). Then, at the conclusion of the study, the responsible physician enters the patient/parent recorded symptoms into the reflux testing software. Even though symptom recording seems to be a simple process, there are many steps along the way that create errors; parents or patients may forget to record symptoms, there may be a lag between symptom occurrence and recording symptoms on the log, symptoms occurring in close temporal proximity may omitted, the time on the recording device may not match the time used for the log (from a wall clock, watch etc), or the symptoms may occur during sleep when both the patient/parents are asleep and therefore cannot complete the log. Therefore, new, objective methods for recording symptoms are needed to avoid the bias of omission seen in clinical practice and reported in the literature (7–9).
To improve the accuracy of detecting coughs during reflux testing, intraesophageal pressure recording (IEPR) at the time of reflux monitoring has been proposed (7). IEPR can accurately measure the occurrence of cough which appears as simultaneous high pressure spikes in the esophagus at the time of coughing (7). Limited studies, one in adults and one in children have shown that esophageal pressure monitoring detects 70–90% more coughs than the standard patient/parent log report and that accurate detection of cough during reflux testing can change the diagnosis of reflux-associated cough in some patients (7, 9).
It is the goal of this prospective study to determine the sensitivity of patient report relative to IEPR monitoring, to determine the relationship between cough and reflux events, as well as the characteristics of reflux events associated with cough, and to determine the difference in symptom index positivity between patient report and IEPR.
Materials and Methods
This was a prospective study in which 20 patients, ages 4–18 years, with a history of chronic intractable cough were included. Any patient presenting to the Aerodigestive Center with a chief complaint of cough and who was undergoing bronchoscopy and endoscopy with pH-MII testing was approached for participation. If patients consented, the patient underwent pH-MII with IEPR. This study was approved by the Boston Children’s Hospital Institutional Review Board on 10/09/2006, and informed consent was obtained from each family unit/patient.
pH-MII with IEPR
A 4 channel esophageal pressure catheter was placed at the time of the endoscopy and the pH-MII. Both catheters were sutured together using absorbable sutures prior to placement, and the sutures were placed in an area of the catheter away from pressure or impedance transducers. Also the pressure sensors were aligned so that they were not in direct contact with the pH or MII sensors. Location of the catheter was confirmed using intraoperative fluoroscopy such that the distal pH sensor was located at the third vertebral angle above the diaphragm (10).
pH-MII and IEPR occurred for a minimum of 20 hours and patient/parents were also asked to record on a log the time of any coughs during the study, using the clock on the pH-MII recording device. After 24 hours, the studies were blindly analyzed by one of the authors (RR) both for reflux and the presence of high pressure, simultaneous, intraesophageal pressure spikes (Figure 1). After the manual analysis, the patient/parent reported coughs were added to the tracings. The time from the patient reported cough to the IEPR spikes were recorded as was the time from any reflux event to the IEPR coughs. The symptom index was defined as the number of symptoms associated with reflux/total number of symptoms and is considered positive if it is >50% (11). The symptom sensitivity index was defined as the total number of reflux episodes associated with symptoms/total number of reflux episodes and is considered positive if it is >10% (12). In this study, we used a standard 2 minute window before and after a cough when considering if reflux was associated with the cough (12, 13). Definitions for reflux by pH-MII have been previously described (14). Means were compared using t-testing or non-parametric equivalents and proportions were compared using chi-square analysis. Logistic regression was performed to determine predictors of reflux-associated coughs.
Figure 1.
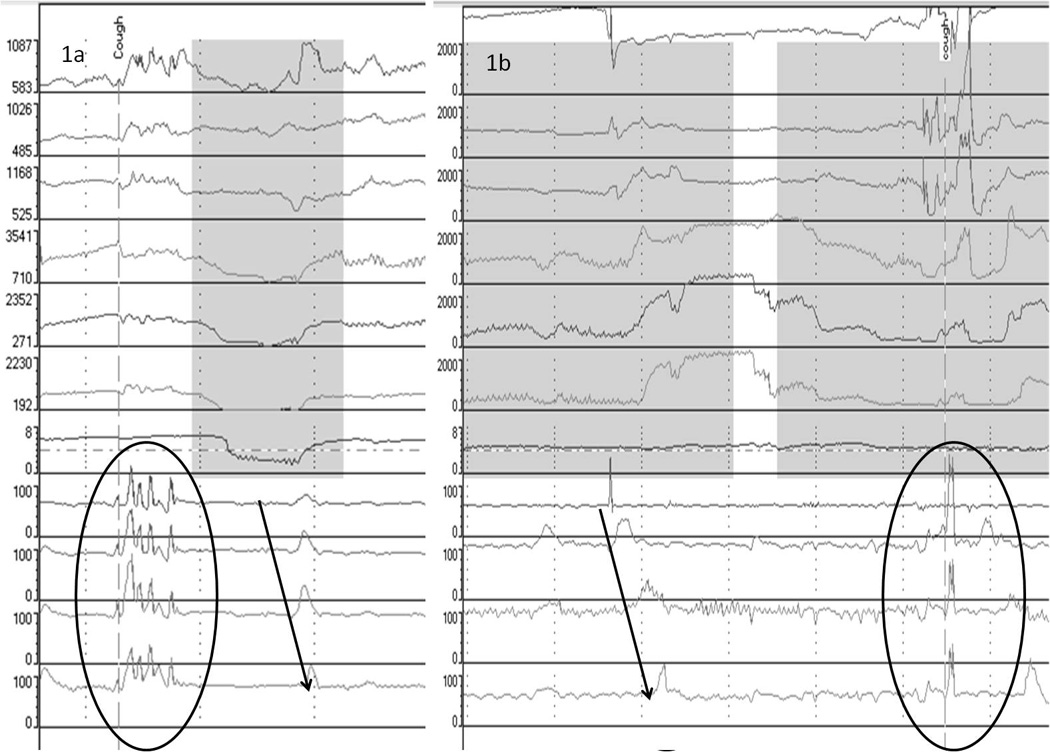
Tracing of a cough preceding reflux (1a) and reflux preceding cough (1b). intraesophageal pressure recording (IEPR) coughs, seen as high amplitude, simultaneous pressure spikes, are shown in the circles. Reflux episodes are shaded gray. The arrow highlights normal, propagating esophageal peristalsis, in contrast to simultaneous pressure spikes with cough.
Statistics
Assuming that there is an average difference of 10 coughs per patient between the patient reported coughs and the IEPR coughs, we would have greater than 90% power to reject the null hypothesis that there is no difference between the two techniques (patient report and IEPR). The Type I error probability associated with this test of this null hypothesis is 0.05. Values are expressed as means ± standard deviation. We compared proportions using chi-square analyses and we compared means using t testing. Paired t tests were used to compare the differences in symptom indices within patients Logistic regression was performed to determine the predictor of symptoms association, between reflux and cough.
Results
20 patients were included in the analysis. The mean duration of the pH-MII testing was 21.5±1.5 hours. The mean age of the patients was 103±41 months. 18/20 patients stopped acid suppression 48 hours prior to testing.
There were 1349 coughs recorded by either the patient or IEPR. An example of a cough triggering a reflux episode and reflux episode triggering a cough using IEPR is shown in Figure 1. The distribution of detected coughs is shown in Figure 2; 94% of all coughs were detected by IEPR, and only 48% of all coughs were reported by patients. The mean time from the IEP cough to the patient reported cough was 11±16 seconds. Using IEPR as the gold standard for the detection of cough, the sensitivity of patient report for the detection of cough is 46%. The specificity of patient report cannot be calculated, as the denominator, no cough by IEPR, cannot be quantified.
Figure 2.
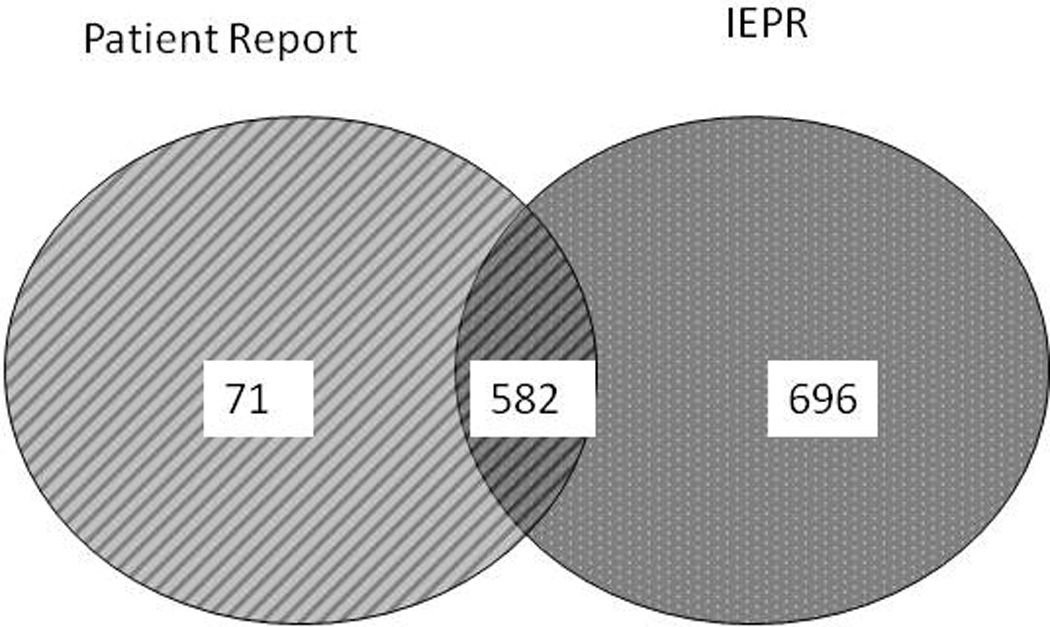
Distribution of coughs detected by patient report and intraesophageal pressure recording (IEPR). Patient report only documents 48% of all coughs.
The distribution of reflux types is shown in Table 1. 944 (71%) coughs were not temporally associated with reflux. 385 (29%) coughs were associated with reflux within a 2 minute window before or after the reflux event. For 223 (58%) coughs, reflux preceded the cough. For 162 (42%) coughs, reflux followed the cough. The mean time between a cough and a reflux episode was 42±39 seconds. 39% of the coughs were associated with non-acid reflux, 37% with acid reflux, and 24% with pH only events. Of the reflux-associated coughs, 29% were associated with distal reflux, 33% with mid-esophageal reflux and 38% with proximal reflux. 27% of the reflux events associated with cough reached the top-most esophageal sensor.
Table 1.
Reflux characteristics in 20 Patients undergoing pH-MII with intraesophageal pressure recording (IEPR) testing.
| Acid Events | 30±23 |
| Non-Acid Events | 20±18 |
| pH-Only Events | 12±10 |
| % Full Column | 39±20 |
| % Proximal Reflux | 0.7±0.8 |
| % Distal Reflux | 1.6±2.0 |
Using logistic regression to determine if reflux characteristics predicted cough generation, neither the type of reflux episode (acid/nonacid/pH only) nor the height of the refluxate (full column) were significant predictors of reflux-cough association (p>0.3)
The mean SSI using IEP monitoring was 39±24. The mean SSI determined by patient report was 25±22 (p=0.0001). 85% of patients had a positive SSI using IEP monitoring. 78.9% had a positive SSI using patient report (p=0.04). 2 patients had a negative SSI using patient report that were positive using IEP monitoring. 1 patient had a positive SSI by patient report that was negative using IEP monitoring. Therefore, IEP monitoring changed the underlying diagnosis in 15% of patients.
The mean SI using IEPR was 30±23. The mean SI determined by patient report was 38±28 (p=0. 01). 15% of patients had a positive SI using IEPR. 30% of patients had a positive SI using patient report (p=0.1). 1 patient had a positive SI using IEPR that was negative based on patient report. 3 patients had a positive SI by patient report that would have been called negative using the IEPR. Therefore, IEPR changed the underlying diagnosis in 20% of patients. The mean SI and number of patients with positive SI and different methods of calculating the SI are shown in Table 2. Because IEPR allows for precise identification of cough time, if we only are interested in reflux episodes preceding cough (and therefore exclude all cough followed by reflux episodes in the numerator of the SI), the number of patients with a positive SI is 0.
Table 2.
different SI results in patients with positive symptom index depending on the method of calculation.
| Symptom Index | Number of Patients with a Positive SI |
Mean SI | P Value |
|---|---|---|---|
| A. SI all Patient Coughs | 6 | 38±28 | P=0.01 (SI patient cough vs SI computer cough) |
| B. SI all Computer Coughs | 3 | 30±23 | P=0.0001 (SI for all computer cough vs SI for computer cough if reflux preceding cough) |
| C. SI for computer cough if reflux preceding cough | 0 | 11±11 | |
| D. SI for Acid Events (pH probe detected acid events including pH only events) | 0 | 14±10 | P=0.03 (SI for pH probe detected acid events vs SI for impedance detected events) |
| E. SI for (impedance detected acid and non-acid events) | 1 | 23±20 |
Discussion
The results of this study strongly support the use of IEPR to study the relationship between gastroesophageal reflux and cough. The addition of pressure monitoring changed the diagnosis in 15–20% of patients depending on the index used. Furthermore, IEPR resulted in the detection of 106% more coughs than patient report alone. This technology which precisely identifies the occurrence of cough represents the greatest improvement in reflux testing since the multichannel impedance testing became available.
Using cough as a model, this study confirms that symptom reporting during pH or pH-MII testing is significantly flawed and, if possible, should not alone be used for clinical decision making. Prior studies have shown that symptom indices, relying on patient report, fail to predict therapeutic response to acid suppression or fundoplication (6, 15–17). Previously this lack of predictive value has been blamed on insensitivity of the symptom index. Based on the present study, this lack of predictive value may relate to poor symptom recording rather than a failure of the symptom index itself. Two reasons for poor symptom recording are a complete failure to record symptoms and a time lag from when a symptom occurs to when it is written on the log. In the present study, we found there was a delay of 11±16 sec from the time a symptom occurred to the time it was recorded on the log, and that 52% of coughs were not recorded in the log at all.
To determine the association between symptoms and cough, differing symptom windows have been proposed. There is significant debate in the literature on the optimal time window that should be used to determine a temporal relationship between reflux and cough (11, 12, 18). Traditionally, a 2 minute window has been used but these windows were determined based on the statistical probability that reflux would occur before or after a patient reported symptom and these windows were determined relying on patient report of symptoms which assumes patient report was correct. Two minutes would allow for a patient to delay recording symptoms yet still allow for the symptom to “count” as reflux associated; this may however pose a problem if clinician needs to understand if the cough or the reflux came first as these time delays could result in a different conclusion. If the window was shorter, the fear would be that a patient delay in reporting symptoms would put it outside the association window and would result in a false negative association. Our data confirms this, and previous studies have shown the same. Sifrim et al found that the median time between the patient and IEPR coughs was 28 seconds with a range of 7–80 seconds (7). Because of the wide range of time of up to 2 minutes of delay between actual cough and patient report, the prior symptom windows needed to be long. Now, with the precision of IEPR, this symptom window should be narrowed; interestingly, when we narrowed the symptom window to include only the 2 minutes before a cough episode, none of the patients had a positive SI, a critically important finding as 3 patients would have been incorrectly classified as having reflux-associated cough when, in fact, those positive results were driven by cough preceding reflux. Furthermore, based on this study showing that IEPR increases the cough detection by more than 100%, the accuracy of symptom association may increase significantly. Therefore, based on the increased cough detection and the elimination of time lags with symptom reporting when IEPR is used, the utility of the SI and the SSI needs to be completely reevaluated in large studies to determine if the new symptom correlations predict medical or surgical outcomes and what time window is ideal for predicting clinical outcome.
In this paper, we chose to use the SI and the SSI to determine the degree of reflux-cough correlation. The only other pediatric paper using IEPR by Blondeau et al manually calculated the Symptom Association Probability (SAP) to determine temporal association (9). We chose to use the SI and SSI because they are quickly calculated by hand (making them the most practical for clinical practice) and, recognizing that clinicians will rely on software for SAP generation, our experience suggests that SAP calculation using software is unreliable. Nevertheless, Blondeau et al found that IEPR resulted in a change in diagnosis in 15% of patients which is similar to our percentages by which IEPR changes diagnosis and management (9).
Another important finding of the present study is that we have identified a group of coughs that was associated with non-acid reflux (19, 20); 40% of coughs associated with reflux in this study would have been missed if only pH-metry was performed and 1 patient would have been incorrectly classified as having a negative SI based on pH-metry alone. The finding, that non-acid reflux can be associated with cough, may explain why studies that have tried to use pH criteria to predict clinical outcome after acid suppression therapy have been negative (21, 22).
In this paper, in contrast to our prior studies and studies by other authors, we did not find a significant association between cough production and either the height of the refluxate (1, 2, 14). In this study, there was a similar association between cough and reflux reaching each of the three esophageal height, distal, mid and proximal esophagus. Also, 24% of coughs associated with reflux were associated with pH-only events which are typically felt to be distal acid reflux that does not extend high enough in the esophagus to be detected by the requisite 3 impedance sensors. The additional precision of IEPR merits additional studies to clarify the mechanism of reflux causing cough, either by microaspiration of full column reflux or vagally mediated reflex arcs triggered by distal esophageal distension or acidification. The lack of association between reflux characteristics and cough may be a result of our relatively small sample size, a population of patients that has failed numerous reflux therapies and is therefore less likely to have reflux-related disease, or an important new finding that is only possible because IEPR allows for more precise cough characterization. Clearly, additional studies using IEP pressure recording in untreated and treated patients are needed to determine if there is a clear type of reflux that reliably generates cough.
This study has several limitations. First, our sample size is small though comparable to both the prior pediatric and adult study using IEPR. Because of discomfort with placing the catheters in small children, currently the probes are placed with sedation. Therefore, the numbers of patients who consent to placement with sedation is smaller than the standard unsedated patient undergoing pH-MII testing. While other technologies have been trialed such as microphone recording of cough, this still-experimental technology has only been paired with pH monitoring in children in a single institution which is not optimal because of the high rates of non-acid reflux in children (23). Second, the discomfort from placing the catheter also limits the utility of the technique in small children so advances in technology to combine pressure and pH-MII into a single catheter are also needed to improve tolerability during placement. Third, we did not calculate how the SAP changes with the addition of IEPR. At our institution, we use the SI based on studies that have shown that SI and SAP have a comparable positive predictive value and sensitivity (15).
In summary, IEPR significantly improves the detection of cough in children undergoing pH-MII testing, and allows a better characterization of its relationship with reflux. The degree of symptom association varies dramatically depending on how symptoms are recorded and if the analysis is restricted only to reflux preceding coughs. This new technique opens the possibility of better defining the windows used for symptom association. Studies are now needed to determine if this increased detection improves therapeutic outcomes but clearly relying on symptom reporting by patients is flawed and clinical decision making based on patient report alone should be done with caution.
Acknowledgments
Funding Source: This work was supported through NIH K23 DK073713-05 (RR) 1R03DK089146-02 (RR), K24DK082792A (SN) and Translational Research Program Junior Investigator Award (RR).
Abbreviations
- pH-MII
Multichannel intraluminal impedance with pH
- SI
Symptom Index
- SSI
Symptom Sensitivity Index
- SAP
Symptom Association Probability
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflict of Interest: None.
Financial Disclosures: None.
References
- 1.Mainie I, Tutuian R, Agrawal A, et al. Fundoplication eliminates chronic cough due to non-acid reflux identified by impedance pH monitoring. Thorax. 2005;60(6):521–523. doi: 10.1136/thx.2005.040139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Tutuian R, Mainie I, Agrawal A, et al. Nonacid reflux in patients with chronic cough on acid-suppressive therapy. Chest. 2006;130(2):386–391. doi: 10.1378/chest.130.2.386. [DOI] [PubMed] [Google Scholar]
- 3.Swoger J, Ponsky J, Hicks DM, et al. Surgical fundoplication in laryngopharyngeal reflux unresponsive to aggressive acid suppression: a controlled study. Clin Gastroenterol Hepatol. 2006;4(4):433–441. doi: 10.1016/j.cgh.2006.01.011. [DOI] [PubMed] [Google Scholar]
- 4.Wassenaar E, Johnston N, Merati A, et al. Pepsin detection in patients with laryngopharyngeal reflux before and after fundoplication. Surg Endosc. 2011;25(12):3870–3876. doi: 10.1007/s00464-011-1813-z. [DOI] [PubMed] [Google Scholar]
- 5.del Genio G, Tolone S, del Genio F, et al. Prospective assessment of patient selection for antireflux surgery by combined multichannel intraluminal impedance pH monitoring. J Gastrointest Surg. 2008;12(9):1491–1496. doi: 10.1007/s11605-008-0583-y. [DOI] [PubMed] [Google Scholar]
- 6.Rosen R, Levine P, Lewis J, et al. Reflux events detected by pH-MII do not determine fundoplication outcome. J Pediatr Gastroenterol Nutr. 2010;50(3):251–255. doi: 10.1097/MPG.0b013e3181b643db. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sifrim D, Dupont L, Blondeau K, et al. Weakly acidic reflux in patients with chronic unexplained cough during 24 hour pressure pH, and impedance monitoring. Gut. 2005;54(4):449–454. doi: 10.1136/gut.2004.055418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Paterson WG, Murat BW. Combined ambulatory esophageal manometry and dual-probe pH-metry in evaluation of patients with chronic unexplained cough. Dig Dis Sci. 1994;39(5):1117–1125. doi: 10.1007/BF02087567. [DOI] [PubMed] [Google Scholar]
- 9.Blondeau K, Mertens V, Dupont L, et al. The relationship between gastroesophageal reflux and cough in children with chronic unexplained cough using combined impedance-pH-manometry recordings. Pediatr Pulmonol. 2010 doi: 10.1002/ppul.21365. [DOI] [PubMed] [Google Scholar]
- 10.Vandenplas Y, Rudolph CD, Di Lorenzo C, et al. Pediatric gastroesophageal reflux clinical practice guidelines: joint recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) J Pediatr Gastroenterol Nutr. 2009;49(4):498–547. doi: 10.1097/MPG.0b013e3181b7f563. [DOI] [PubMed] [Google Scholar]
- 11.Wiener GJ, Richter JE, Copper JB, et al. The symptom index: a clinically important parameter of ambulatory 24-hour esophageal pH monitoring. Am J Gastroenterol. 1988;83(4):358–361. [PubMed] [Google Scholar]
- 12.Breumelhof R, Smout AJ. The symptom sensitivity index: a valuable additional parameter in 24-hour esophageal pH recording. Am J Gastroenterol. 1991;86(2):160–164. [PubMed] [Google Scholar]
- 13.Omari TI, Schwarzer A, vanWijk MP, et al. Optimisation of the reflux-symptom association statistics for use in infants being investigated by 24-hour pH impedance. J Pediatr Gastroenterol Nutr. 2011;52(4):408–413. doi: 10.1097/MPG.0b013e3181f474c7. [DOI] [PubMed] [Google Scholar]
- 14.Rosen R, Nurko S. The importance of multichannel intraluminal impedance in the evaluation of children with persistent respiratory symptoms. Am J Gastroenterol. 2004;99(12):2452–2458. doi: 10.1111/j.1572-0241.2004.40268.x. [DOI] [PubMed] [Google Scholar]
- 15.Taghavi SA, Ghasedi M, Saberi-Firoozi M, et al. Symptom association probability and symptom sensitivity index: preferable but still suboptimal predictors of response to high dose omeprazole. Gut. 2005;54(8):1067–1071. doi: 10.1136/gut.2004.054981. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Broeders JA, Draaisma WA, Bredenoord AJ, et al. Long-term outcome of Nissen fundoplication in non-erosive and erosive gastro-oesophageal reflux disease. Br J Surg. 2010;97(6):845–852. doi: 10.1002/bjs.7023. [DOI] [PubMed] [Google Scholar]
- 17.Francis DO, Goutte M, Slaughter JC, et al. Traditional reflux parameters and not impedance monitoring predict outcome after fundoplication in extraesophageal reflux. Laryngoscope. 2011;121(9):1902–1909. doi: 10.1002/lary.21897. [DOI] [PubMed] [Google Scholar]
- 18.Lam HG, Breumelhof R, Roelofs JM, et al. What is the optimal time window in symptom analysis of 24-hour esophageal pressure and pH data? Dig Dis Sci. 1994;39(2):402–409. doi: 10.1007/BF02090215. [DOI] [PubMed] [Google Scholar]
- 19.Ghezzi M, Guida E, Ullmann N, et al. Weakly acidic gastroesophageal refluxes are frequently triggers in young children with chronic cough. Pediatr Pulmonol. 2012 doi: 10.1002/ppul.22581. [DOI] [PubMed] [Google Scholar]
- 20.Borrelli O, Marabotto C, Mancini V, et al. Role of gastroesophageal reflux in children with unexplained chronic cough. J Pediatr Gastroenterol Nutr. 2011;53(3):287–292. doi: 10.1097/MPG.0b013e318216e1ad. [DOI] [PubMed] [Google Scholar]
- 21.Holbrook JT, Wise RA, Gold BD, et al. Lansoprazole for children with poorly controlled asthma: a randomized controlled trial. JAMA. 2012;307(4):373–381. doi: 10.1001/jama.2011.2035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Mastronarde JG, Anthonisen NR, Castro M, et al. Efficacy of esomeprazole for treatment of poorly controlled asthma. N Engl J Med. 2009;360(15):1487–1499. doi: 10.1056/NEJMoa0806290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Chang AB, Connor FL, Petsky HL, et al. An objective study of acid reflux and cough in children using an ambulatory pHmetry-cough logger. Arch Dis Child. 2011;96(5):468–472. doi: 10.1136/adc.2009.177733. [DOI] [PubMed] [Google Scholar]